
Abstract
Objective:
The continuing COVID-19 pandemic is a coronavirus-related health emergency (severe acute respiratory syndrome coronavirus 2). Inadequate efforts are still being made to address the illness situation in Libya, and this must change. To address these issues, we looked into the demography and trend of the disease as well as the potential risk factors for infection.
Methods:
This study is a retrospective case–control study conducted online among 616 COVID-19 patients. The p0.05 value, odds ratios, and 95% confidence intervals were calculated and analyzed from the drawn data.
Results:
Males were at high risk of COVID-19 than females (odds ratio = 1.3, 95% confidence interval: 1.042–1.622; p = 0.02). Anosmia and ageusia were more prominent in females. Patients with an “AB” blood group are significantly susceptible to infection. Adults (31 and above) are highly liable to infection. The univariate logistic regression analysis revealed that smoking is a risk factor for those above 60 years (odds ratio = 2.228, 95% confidence interval: 1.145–4.336; p = 0.018). Individuals with chronic diseases such as diabetes and/or hypertension are more prone to COVID-19 (odds ratio = 10.045, 95% confidence interval: 3.078–32.794; p = 0.000 and odds ratio = 11.508, 95% confidence interval: 3.930–33.695; p = 0.000, respectively).
Conclusion:
This study provided for the first time the demographic data and the trend of COVID-19 infection in Libya, which will assist the stakeholders and governmental bodies in planning protection strategies against the pandemic.
Introduction
COVID-19, the pandemic disease caused by the coronavirus (severe acute respiratory syndrome coronavirus 2, SARS-CoV-2), was initially discovered in late 2019 in Wuhan city of Hubei Province in China, from where it struck almost the entire globe, leaving behind millions of infections and thousands of lost lives. 1 Its ability to result in a severe illness that could culminate in septic shock, acute dyspnea, and/or hypoxemia could lead to a respiratory collapse. They may eventually lead to the victim’s death. 2 The relationship between COVID-19 contraction and blood group types was still being debated. Although many have used big sample sizes to illustrate the presence of a clear link,3–6 several other investigations have shown no connection between COVID-19 infection and blood types.7–10 The ABO locus has been linked to genetic connections with both infection risk and disease severity. With the use of preliminary experimental data, certain fundamental hypotheses have been proposed to explain the found connections.11,12 The A (Rh +ve) blood group seems most vulnerable, while O (Rh +ve) is least subject to the virus infection. 3 A genome-wide association study using 1980 blood samples further supported the previous observation concerning A and O blood types. 13 While many reports linked the susceptibility to COVID-19 infection with A and O blood groups, a study showed that only females with the A blood group were at significantly higher risk of COVID-19 infection.14,15 Sixty-seven thousand three hundred forty French individuals were involved in a multiple cohorts’ project. ELISA was used to identify anti-SARS-CoV-2 antibodies by focusing on the protein spike (S) and nucleocapsid (NP). These findings demonstrated that non-O people—particularly types A and AB—were more likely to have anti-SARS-CoV-2 antibodies. Hence, highlighting a lower risk for blood type O and a higher sensitivity to infection for those with blood types A and AB. 16 Given that monoclonal or naturally occurring human anti-A antibodies specifically inhibit the spike protein/angiotensin-converting enzyme 2 (ACE2)-dependent adhesion to ACE2-expressing cell lines, cellular models have proposed an explanation for the modulation of infection by blood type. As a result, people with non-A blood types, specifically O and B, which produce anti-A antibodies, may be less vulnerable to the SARS-CoV-2. 12 While hypertension (HT) and diabetes mellitus are being repeatedly reported among the high-risk factors, 17 researchers have shown that the death rate among COVID-19 patients with diabetic mellitus and HT is not essentially different from the ordinary death prevalence rates. 18 Identifying the target groups at high risk is among many measures needed to be addressed to provide them with protective measures. Old age, chronic diseases, gender, 19 immunocompromised condition, blood type A (Rh +ve), and other factors are known risk factors for contracting and later developing severe COVID-19. 19 See the studies by Shibeeb and Khan, 20 Abuawwad et al., 21 Turhan et al., 22 and Hafez et al. 23 for comprehensive recent reviews on the relationship between the ABO blood system and the Rh factor and their association with COVID-19 infection, susceptibility, and severity. Although the initial virus that caused the first-ever SARS in Hong Kong in March 2003 19 is no longer a concern, the known characteristics of the current SARS-CoV-2 do not appear to disappear quickly, and many countries are now experiencing the second wave of the outbreak. 19 Thus, knowing how this virus disseminates, its favorable conditions, mechanism of action, and so on is urgently needed. In Libya, where most less protective measures and poor medical facilities and accessibility are present, since the onset of the outbreak in late March 2020 and until August 2022, the disease has left almost half a million infected and thousands dead, with 85,529 cumulative cases.19,24 This rapid dissemination of the infection urged WHO to issue a situation report expressing worries and concerns about the transmission rate of the virus in the country. 25 Although epidemiological surveillance generally catches a limited number of confirmed COVID-19 cases, it still provides vital information on determining the demand of affected populations, the behavior of the disease, or exposure, and helps with governmental control initiatives. Therefore, this case–control study was planned to shed light on the vulnerable gender, age group, the relation of SARS-CoV-2 infection with ABO blood groups, the implication of social distancing, the variability of symptoms associated with these factors, and so on.
Materials and methods
Determination of sample size
To determine the minimum sample size to provide significant results, the following Thompson 26 equation was used:

where n is the sample size; N, population size (6.654 million, estimated at the time of the study); z, the confidence level at 95% (1.96); d, the error proportion (0.05); and p, probability (50%). The minimum required sample size was 384.
Study design and sample collection
An online poll was used to conduct a case–control study on COVID-19 infection in Libya between the period of August and December 2020. The healthy participants were considered as the control and the SARS-CoV-2 individuals were the cases. All collected questionnaires were included except for 46 responses—out of a total of 1455—that were rejected because they were incomplete. The final number was 1399 (616 COVID-19 cases and 783 healthy controls). Details related to demographic data, the history of chronic diseases, adherence to social distancing regulations, smoking information, and so on were collected in this survey. The questionnaire is based on the questions used by Taha et al. 3 with slight modifications (https://docs.google.com/forms/d/1npzS1zLOcwxi01d1GFK0CAKr5tfDes6BtObB8YMkN2M/edit; Supplemental Material S1). The bias for using an online questionnaire is described as one of the study limitations and is examined in Discussion section. The STROBE guidelines for case–control design was followed in this study. The STROBE checklist is provided in Supplemental Material S2.
COVID-19 cases confirmation
Everyone who responded to the survey stated that their diagnosis was made in a hospital with the necessary equipment(s). Real-time reverse transcription-polymerase chain reaction (RT-PCR) was carried out to detect both the beta coronavirus E and RdRp genes. Following it, the rapid SARS-CoV-2 antigen tests developed by the Institute of International Health, Charité, Berlin, were used to determine whether a patient had SARS-CoV-2 infection.27,28 A rapid serological test using the lateral flow immunoassay technique (Right Sign TM kits manufactured by Biotest, Lot No. COV20030003, Dreieich, Germany)was also used to assess the presence of SARS-CoV-2 immunoglobulin M/G.
Statistical analysis
Descriptive statistics using cross-tabulation and chi-square analysis was performed. Two-tailed multivariate logistic regression was used to calculate the odds ratio (OR) at statistical significance (p < 0.05). The logistic regression model was adjusted for the gender, age demography, blood groups, adherence to social distancing protocol, and history for chronic diseases and smoking to give an overview of the susceptible and protected individuals under the studied factor. The multivariate logistic regression was performed by considering the infected individuals with COVID-19 as dependent with the healthy individuals as the reference category, and the other factors as covariates, the analysis were done under default statistical setting. The statistical analysis was performed using SPSS software version 26 (IBM SPSS Statistics for Windows, Version 26.0, IBM Corp, Armonk, NY, USA).
Ethical consideration
All participants were informed about the aim and objectives of this study either directly through the informed consent statement provided in the questionnaire that declared that by taking the poll, participants are consenting to the use of the provided data for the scientific purposes of the study or was taken verbally by reading the statement to the participant. The study was approved by the Ethical Committee of the University of Benghazi.
Results
Based on the data collected from the online poll between the period of August and December 2020, the gender ratio among COVID-19 patients was 1.5 female:1 male; yet male patients were more susceptible to SARS-CoV-2 infection than females (OR = 1.3, 95% confidence interval (CI): 1.042–1.622; p = 0.02). The OR related to age demography indicated that in the adult age groups (31 years and above) individuals above 60, were the most vulnerable to infection (OR = 40.633, 95% CI: 18.036–91.538; p = 0.000); 70% of the COVID-19 patients are distributed within this age demography (30 <) which is comparable to the 38% of the healthy cases (Table 1). Males above 60 years (18%) had a higher frequency when compared to females (8%). With respect to chronic diseases such as diabetes, HT, and any combination of the chronic diseases, this age group had a higher frequency (OR = 10.045, 95% CI: 3.078–32.794; p = 0.000), (OR = 11.508, 95% CI: 3.930–33.695; p = 0.000), and (OR = 4.941, 95% CI: 2.534–9.636; p = 0.000), respectively. Male patients were two times more delinquent to preventative measures, that is, social distancing and wearing masks than females. Among participants, while there was no direct correlation between smoking and the risk of infection by SARS-CoV-2, there was an indirect association between age (above 60 years) and smoking (OR = 2.228, 95% CI: 1.145–4.336; p = 0.018), and those participants were solely males. This is only evident in univariate analysis but not in the multivariate regression analysis (Tables 1 and 2 and Figure 1). It is important to mention that to avoid misrepresentation that might result from what is known as Table 2 fallacy, 29 the data analysis presented in Table 2 is derived from the univariate- and multivariate-adjusted associations based on age groups in the COVID-19 patients based on the same regression model described in Table 1. This was done to study the impact of age as a secondary cofactor for contracting COVID-19 and how it might influence the outcome of the other factors. Table 2 presents only the significant association found between the specific group and chronic diseases and smoking. And there were no significant associations reported between any age groups and the other studied cofactors reported in Table 1.
Sociodemographic data analysis and related OR associated with COVID-19 infection.

bold values represent the significant results at p0.05.
Significant logistic regression and OR among age subgroups of COVID-19 patients against the history of chronic diseases and smoking habit.
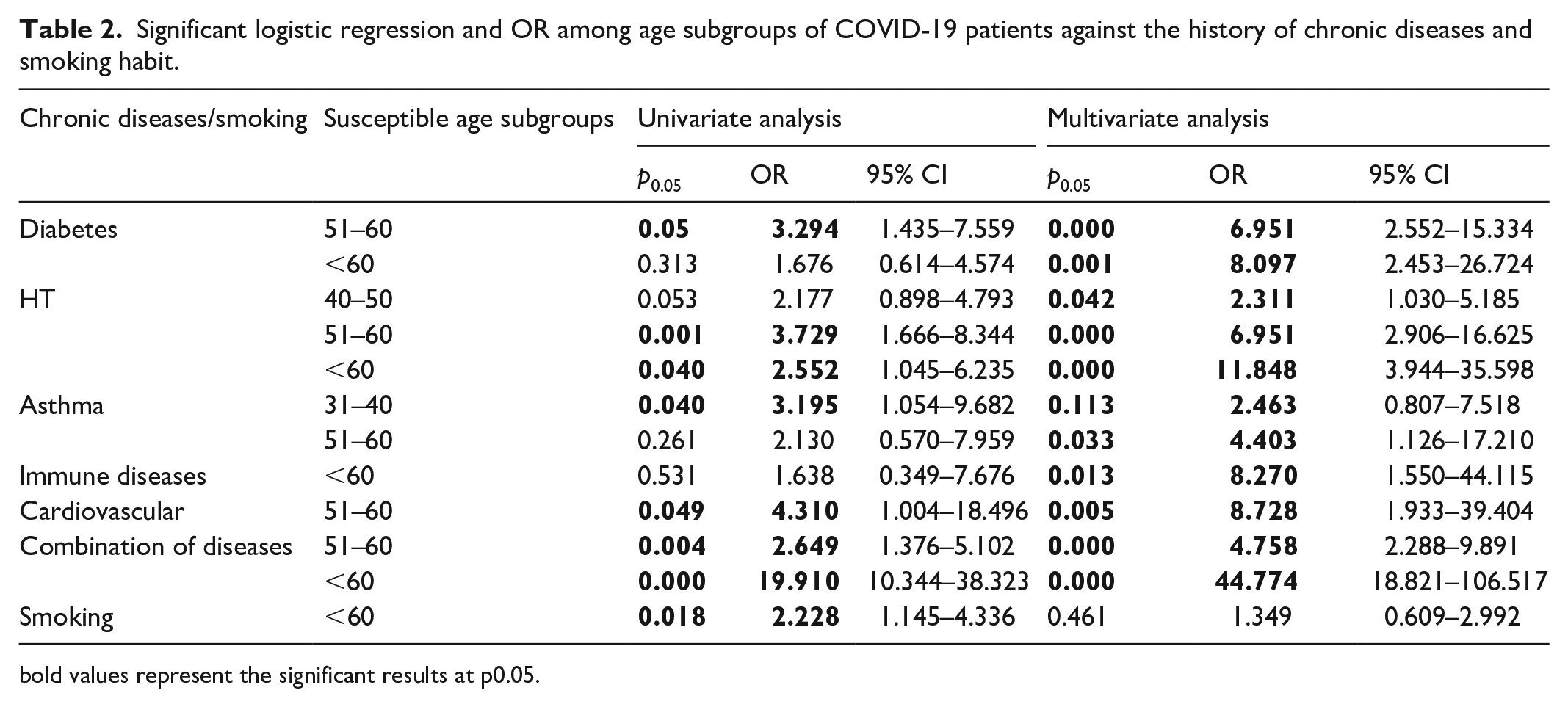
bold values represent the significant results at p0.05.

Demographic trend among COVID-19 patients (N, 616). Gender distribution and dissemination in (a) age subgroups, (b) blood groups, (c) patients with a history of chronic diseases, (d) adherence to social distancing, and (e) smokers and nonsmokers.
The distribution of blood groups varied between the case and control. There was an increased rate of infection among A and B blood groups, with a significant result noted for the latter for both Rhesus factors (AB+: OR = 2.397, 95% CI: 1.200–4.788; p = 0.013 and AB−: OR = 4.538, 95% CI: 1.267–16.249; p = 0.020) (Table 1). The age cluster (31 to <60 years) covers around 70% of each blood-group-infected patients; 10% of AB+ COVID-19 patients had diabetes, while 6% suffered from HT, asthma, and a combination of these diseases (Figure 2).
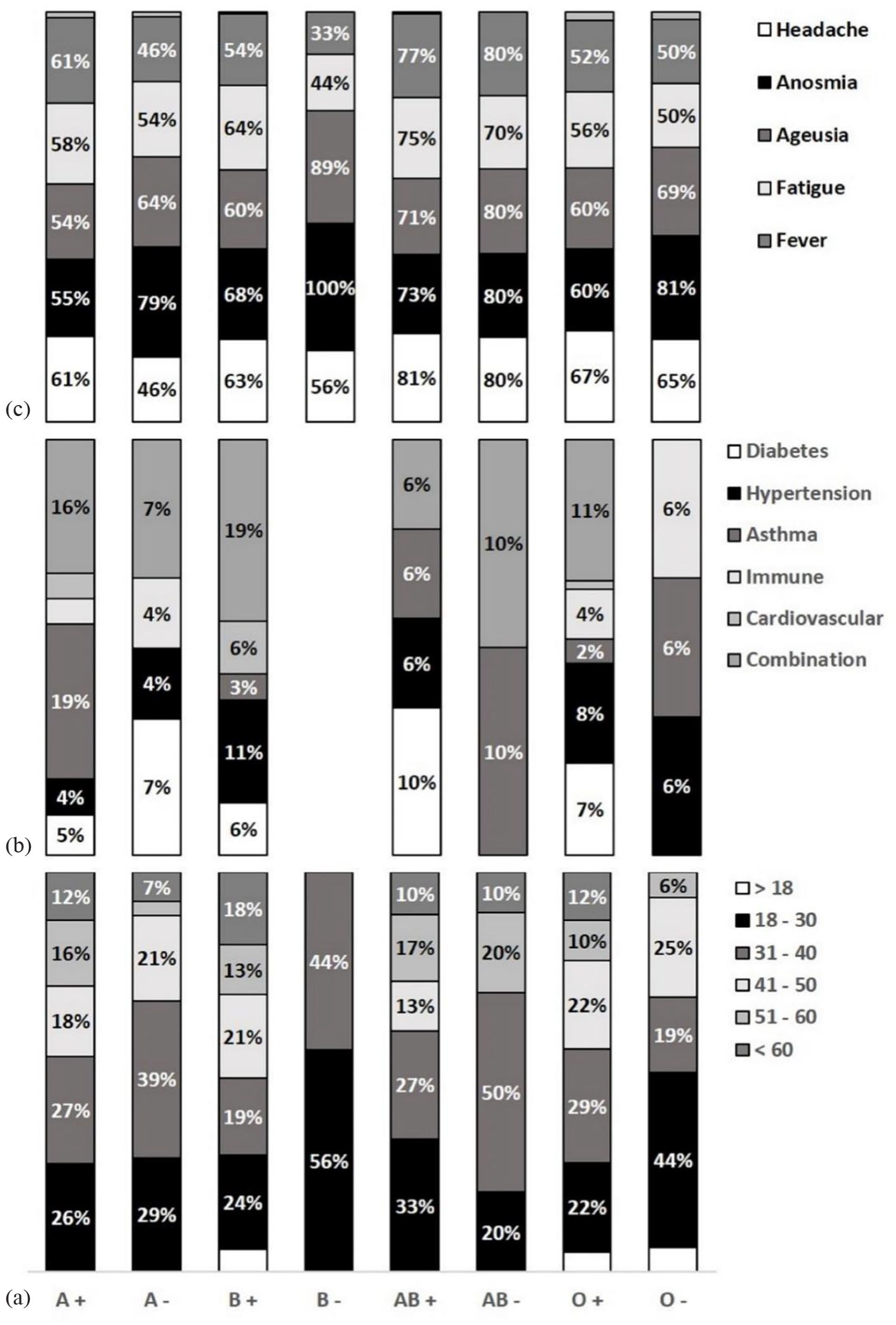
Dissemination of (a) age subgroups, (b) history of chronic diseases, and (c) infection’s major symptoms among COVID-19 patients’ (N, 616) blood groups.
Of the 616 participants confirmed patients in this survey, 5% have remained asymptomatic. Symptoms such as headache, anosmia, fatigue, ageusia, fever, and/or a different combination of them were the most frequent and experienced by more than 50% of them; 70%–80% of these significant symptoms were observed in the AB blood group patients. Anosmia and ageusia were manifested in higher frequency among the female patients than in the male patients. Around 49% of patients remained symptomatic for 2 weeks, yet some, though few, had symptoms for up to 8 weeks (Figures 3 and 4).
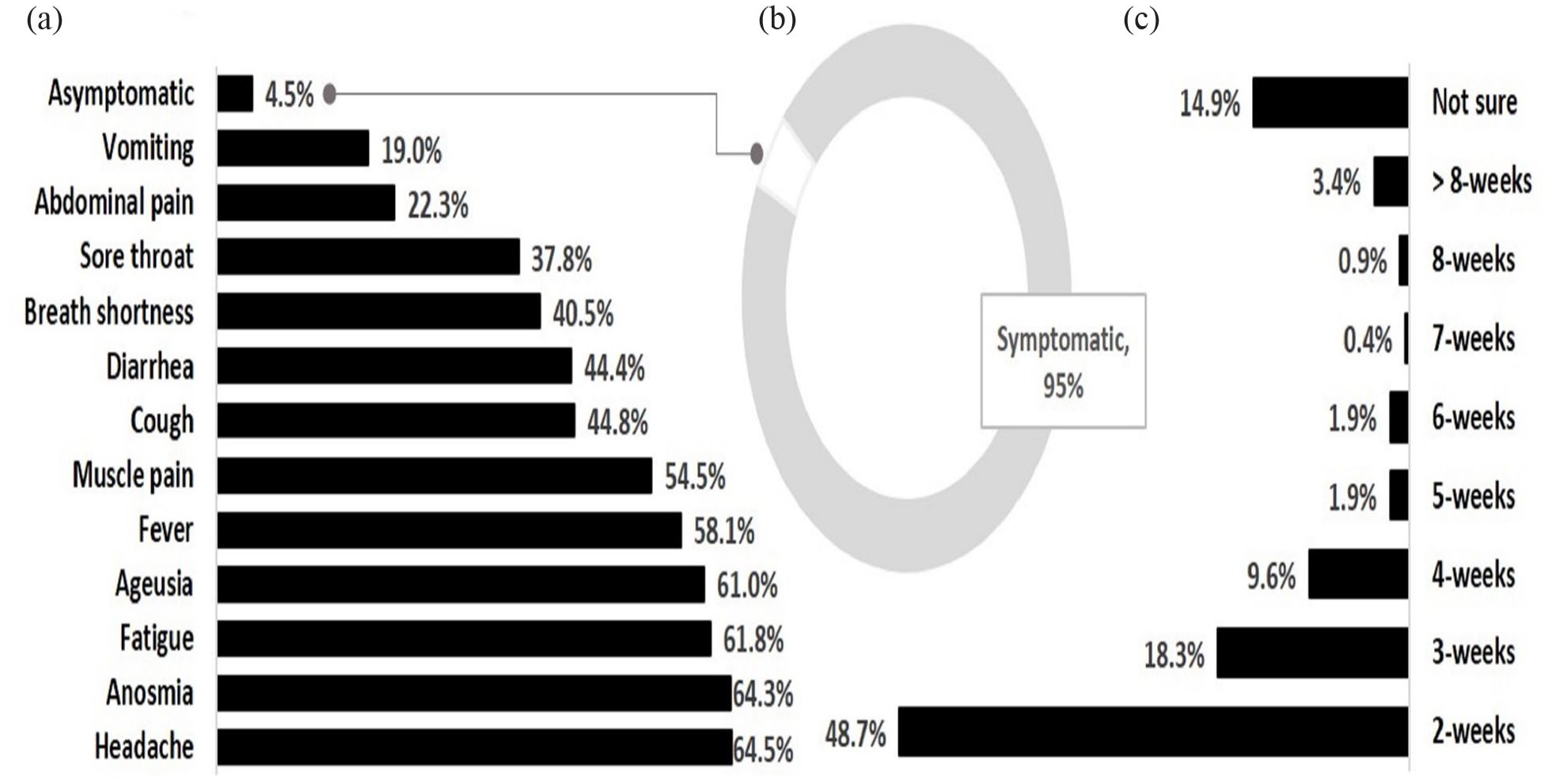
COVID-19 symptoms as described by patients (N, 616). (a) Symptoms, (b) symptomatic patients against asymptomatic, and (c) duration of symptoms after diagnosis confirmation.

Distribution of anosmia and ageusia between COVID-19 male and female patients (N, 616).
Discussion
This online retrospective case–control study was conducted from August to December 2020 to gain an idea of the COVID-19 infection regarding the demographic data, factors enhancing the virus dissemination, and contraction of the infection. In all, 616 COVID-19 patients volunteered to participate in the study; their infections were either confirmed by RT-PCR or by detecting blood-circulating SARS-CoV-2 antibodies. 30 The tendency to catch the virus was significantly more in the case of males than in females. This result was contrary to the findings of Taha et al. who conducted a similar retrospective study in Khartoum, Sudan; females were found to be significantly more prone to infection than males. 3 The data on the vulnerability of men to infection are rather piling up; for example, in Korea, although the prevalence of infection was more in men than in women, the differences were insignificant. 27 The higher contractibility of men to COVID-19 has been ascribed to multiple factors such as (1) higher expression level of ACE2, the host cell receptor that is known to mediate SARS-CoV-2 entry into the victim’s cells; (2) bad habits such as smoking and drinking 31 ; (3) possible harboring of the virus in the testis; (4) delayed SARS-CoV-2 clearance from the bloodstream 32 ; and (5) the stronger immune response in females than in males. 33 In the previous coronavirus, MERS, and SARS-CoV attacks, the male gender was linked with worse results. 34 Moreover, the available current evidence linking men to COVID-19 showed escalated mortality. 35 However, in some other studies, morbidity rates were shown to be equal among both genders, while mortality was inclined toward males, 36 suggesting that other elements such as cultural, economic, and social behaviors might also be equally important to consider. Although older people were struck harder by the pandemic, 37 in this study, the amenability to virus infection was significantly higher in all age groups that fell between 30 and <60 years. The inclusion of the young age was not surprising. It could likely be attributed to the fact that young people are involved more in social activities, and some might see themselves as invincible. 38 In the present investigation, we have found a significant correlation between smoking and the age group above 60. Smoking has been significantly linked with COVID-19 morbidity and mortality rates, through upregulating ACE2 receptor expression. 39 Around 73 patients (15%) of the total were smokers, and they were all men. Although the relationship between smoking and COVID-19 morbidity gave an insignificant result, blood groups are already known to associate with many diseases such as malaria, heart ailments, and cholera, and with COVID-19 infection too. For reviews, see the study by Cakir. 40 Blood group “O” may have a lower risk of COVID-19 infection, whereas “A” blood type was with the highest risk.3,41 The obvious vulnerability of blood type “A” has been attributed to a potential interaction between the spike virus glycoprotein and the cell surface receptor of blood type “A.” 42 The relationship between COVID-19 and blood group susceptibility has been genetically established. 13 It is interesting to note that in this study we were unable to find any conclusive evidence of a link with the “O” or “A” blood groups. However, people with the blood group “A” showed a clear increase in infection rates, whereas people with the blood group “O” showed a clear drop in infection rates. On the other hand, those with the blood type “AB” are far more likely to contract SARS-CoV-2 infection, especially if they have a negative RH. Such susceptibility was also seen in Nepalian population from the district of Rupandehi, where the COVID-19 infection was significantly linked to “AB” blood group. 43 In a different investigation carried out in India by Singh and colleagues, carriers of the blood group AB had the highest quantity of SARS-CoV-2-neutralizing antibodies. These findings show that people with blood type AB are more susceptible than those with other blood types. 44 According to a similar study done in Iraq, the blood type AB is substantially more likely than other blood types to require respiratory support, experience persistent palpitations, and dizziness. 45 The risk of intubation and/or mortality was found to be high with the “AB” blood group and low with the “A” blood group by Zietz et al. when they investigated the relationship between the severity of COVID-19 and the ABO blood group system. 41 While Ad’hiah et al. termed the “AB” blood type as a possible biomarker for COVID-19 susceptibility. 19 In an interesting study done in Saudi Arabia by Hindawi and colleagues, it was found that those with blood group B had the highest risk of contracting the virus compared to people with blood groups A and AB. 46 In contrast to many other investigations,47–49 these authors did not find a connection between the disease and Rh factors. To further substantiate their findings, the authors recommended a bigger sample size. 46 Yet, research that revealed no correlation between the Rh factor and COVID-19 morbidity is not scarce.50,51 Although anosmia (loss of smell) was among the symptoms reported earlier with the SARS-CoV epidemic attack in 2003, 52 its manifestation with SARS-CoV-2 was rather virulent. This urged WHO and other research scientists to consider anosmia and ageusia (loss of taste), which were interestingly found to be more frequent in females than in males, as biomarkers for COVID-19 diagnosis. 53 Anosmia has been attributed to possible damage caused by the virus to the olfactory epithelial cells. 54 We have also found anosmia and ageusia to be more prominent in females than in males (Figure 4). Headache, anosmia, fatigue, and ageusia were the major symptoms experienced by most patients, with 5% of confirmed patients remaining asymptomatic. According to Taha and colleagues’ investigation, fatigue, headache, and fever were the three main symptoms; 13% of confirmed COVID-19 cases, however, were still asymptomatic. 3 In the current investigation, we found a strong relationship between diabetes and HT, and SARS-CoV-2 infection. Numerous COVID-19 individuals have been reported to have additional chronic conditions, and it is thought that these comorbid conditions raise the risk and severity of the disease. 55 This study, however, has certain limitations. First, because there is such a large body of literature on the newly developing illness, our group may have missed some studies published during the epidemic. Second, we did not perform a pilot test for the questionnaire in Libya, and the study was mostly computer based. Many patients with limited access to computers or cell phones may have been unable to participate. Third, around 1400 people took part in this study, representing approximately 0.3% of all Libyans who developed COVID-19. As a result, this cohort may represent a small number of patients who had access to the online questionnaire and so may not accurately reflect the state of the nation’s health. Keep in mind that the literacy rate in Libya, according to UNESCO data, is as low as 16.3% for vulnerable age groups (>65 years). 56 As a result, a larger population sample may be needed to draw a definitive conclusion.
Conclusion
In conclusion, this case–control study has bestowed an insight into the demographic data, trends, and factors associated with COVID-19 infection for the first time in Libya. A high proportion of cases is reported among the active persons in the working-age groups, with the “AB” blood group having a higher significant risk of infection. Individuals with chronic diseases, regardless of their age group, are liable to be victimized by comorbidity. These data will be of importance for governmental decision-makers and stakeholders in the fields related to healthcare and other allied sectors to educate the public about the dissemination and ways of prevention and can be used for future planning and preparations. The apparent disparities in the results seen in the present work in comparison to other publications with regard to demographic data and factors associated with the disease, such as age, gender, ABO blood system, symptoms, and so on, may indicate a high degree of complexity of this virus and its resultant physio-pathogenicity and may necessitate further intensive investigations.
Supplemental Material
sj-doc-2-smo-10.1177_20503121231187736 – Supplemental material for Association of ABO blood types and clinical variables with COVID-19 infection severity in Libya
Supplemental material, sj-doc-2-smo-10.1177_20503121231187736 for Association of ABO blood types and clinical variables with COVID-19 infection severity in Libya by Sara A Abdulla, Hayam A Elawamy, Negia AE Mohamed, Enas H Abduallah, Habsa AA Amshahar, Nadir K Abuzaeid, Mohamed AM Eisa, Makarim Elfadil M Osman and Emadeldin Hassan E Konozy in SAGE Open Medicine
Supplemental Material
sj-pdf-1-smo-10.1177_20503121231187736 – Supplemental material for Association of ABO blood types and clinical variables with COVID-19 infection severity in Libya
Supplemental material, sj-pdf-1-smo-10.1177_20503121231187736 for Association of ABO blood types and clinical variables with COVID-19 infection severity in Libya by Sara A Abdulla, Hayam A Elawamy, Negia AE Mohamed, Enas H Abduallah, Habsa AA Amshahar, Nadir K Abuzaeid, Mohamed AM Eisa, Makarim Elfadil M Osman and Emadeldin Hassan E Konozy in SAGE Open Medicine
Supplemental Material
sj-pdf-3-smo-10.1177_20503121231187736 – Supplemental material for Association of ABO blood types and clinical variables with COVID-19 infection severity in Libya
Supplemental material, sj-pdf-3-smo-10.1177_20503121231187736 for Association of ABO blood types and clinical variables with COVID-19 infection severity in Libya by Sara A Abdulla, Hayam A Elawamy, Negia AE Mohamed, Enas H Abduallah, Habsa AA Amshahar, Nadir K Abuzaeid, Mohamed AM Eisa, Makarim Elfadil M Osman and Emadeldin Hassan E Konozy in SAGE Open Medicine
Footnotes
Author contributions
Conceptualization and writing the original draft were performed by EHEK, SAA, and MEMO. Data collection, investigation, and formal analysis were conducted by SAA, MEMO, HAE, EHA, and NKA. Data validation and visualization were done by NAEM, HAA, and MAME. All authors revised the manuscript and approved the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.