
Abstract
Objectives:
Multifocal fibrosclerosis is a rare disorder causing progressive fibrosis of multiple organ systems. Existing data on the disease show that there are multiple manifestations of the disease, with different outcomes. However, quantitative data are scarce, prompting the need for our investigation.
Method:
A comprehensive systematic review was performed from inception to November 16, 2022, with the restriction of English language, not including review articles. Article screening and extraction was performed independently, and shortlisted articles were assessed for bias. Analysis was performed using SPSS Version 25 (IBM® SPSS® Statistics; Chicago, IL, USA). Data were presented as frequencies and percentages, with a confidence interval of 95%.
Result:
This review included 134 patients, with 78 (58.2%) males. Mean age was 53.6 years and included two pediatric patients. The most common comorbidity was diabetes (9.7%). Prevalent presenting symptoms included pain (47.8%) and swelling (35.1%). A mean of 2.51 organs or anatomical sites was affected, retroperitoneum (64.2%) being most affected. The pancreas (30.0%) and digestive system (47.0%) were the organs/organ systems most affected. Patients had favorable outcomes in 79.1% of cases, 87.3% had no relapse, and 91.8% of patients survived the condition.
Conclusion:
The findings in this study provide a quantitative measurement of the demographics, presentations, organ manifestations, and outcomes of multifocal fibrosclerosis. We found the disease to be prevalent in males in Japan or the United States, with the abdomen and its organs being commonly involved.
Introduction
Multifocal fibrosclerosis (MFS; also known as idiopathic MFS, familial MFS) is a rare, fibrosing disease affecting multiple organs, especially the thyroid gland, mediastinum, and retroperitoneum. The orbits, pancreas, and gallbladder are also less commonly affected in this condition. 1 The disorder was first reported by Comings et al. in 1967. 2 The study reported two brothers to have developed multiple similar fibrotic processes in the retroperitoneum, mediastinum, thyroid, orbit, and hepatobiliary system, therefore proposing a possible genetic link in the disease. The study went on to classify all the lesions as the product of one disease process. However, as it was the first incidence of such a disease, the authors did not label it as a distinct fibrosing syndrome. Over the years, many studies came forward describing similar fibrotic processes in other organs. 3 According to Goldman’s Cecil Medicine, MFS is a rare condition, with an incidence of 20 in 100,000. 4 It may present with symptoms such as flank or abdominal pain, diarrhea and dehydration, renal failure, or edema. 4
The single major factor required for classification of a disease process as MFS is the presence of fibrosis in at least one organ; therefore, multiorgan diseases without any fibrosis are not included as part of MFS. However, it must be noted that not all diseases with fibrosing elements should be considered MFS. Complications of the condition include superior vena cava syndrome, portal hypertension, and esophageal varices. 4 Widely used treatment includes surgery and corticosteroids, although immunosuppressants may also be added. 4
In 2001, the first incidence of a case of sclerosing pancreatitis presenting with increased IgG4 levels was reported by Hamano et al. 5 IgG4 was later found to be elevated in multiorgan fibrosing diseases as well. 6 The clinical manifestations of the disease due to the involvement of multiple organs may be confused with similar multiorgan presentations such as Erdheim–Chester disease, lymphoma, and Castleman disease.7,8 Diagnosis of IgG4-RD is made through non-invasive techniques including radiological imaging, polyclonal hypergammaglobulinemia (specifically serum IgG and IgG4 levels), as well as through invasive methods such as biopsy with histopathology.9,10 Treatment includes systemic corticosteroids such as prednisone, as well as rituximab, an anti-CD20 antibody used to cause B-cell depletion. 11
At a conference in 2012, the term IgG4-related disease (IgG4-RD) was coined and recommended for the single-organ and multiorgan manifestations of diseases with raised IgG4 levels, such as that described by Hamano et al. 12 This term now encompassed all other names used to refer to the disease, such as IgG4-related systemic disease and IgG4-related sclerosing disease, among others. These recommendations also considered MFS to be a part of the IgG4-RD spectrum. 12
While it may be wrongly assumed that all cases of MFS are related to IgG4-RD, this is not the case, as some studies have reported the disease with normal IgG subclass levels. These conditions have been termed as non-IgG4-related MFS.13,14 In addition, as MFS is simply a subtype of IgG4-RD, not all cases of IgG4-RD are MFS either. Our review aims to answer questions related to MFS without involving IgG4-RD into the argument, as although the two conditions are linked, it is not suitable to place them both in one review.
Our systematic review aims to answer the following questions to have an outline that would help summarize the clinical presentations and outcomes of MFS: [1] what are the different clinical presentations of MFS? [2] how many and which organ systems are commonly affected? and [3] what is the prognosis and outcome of the disease? Are there any significant factors that affect the outcome?
Materials and methods
This study was conducted in accordance with the latest guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). The completed PRISMA Checklist for Systematic Reviews is shown in Supplemental Table 1. The review protocol was registered on PROSPERO (CRD42022347927). 15
Search strategy
A literature search of PubMed, Google Scholar, Science Direct, and Cochrane databases was conducted from inception to the last updated date of November 16, 2022. The search terms included are “familial multifocal fibrosclerosis,” “Riedel thyroiditis,” and “retroperitoneal fibrosis” to formulate a comprehensive search string, which is provided in Supplemental Table 2. To expand the search parameter, preprint articles on MedRxiv and BioRxiv were screened. The bibliographies of included articles were also screened for any articles that fit the criteria.
Study selection
Observational human studies on MFS were included. The main exclusion criteria were (1) articles not in English, (2) review articles, clinical trials, randomized control trials, opinion articles, commentaries, (3) articles with any one of clinical presentation, diagnosis, organs involved, or outcomes not discussed, (4) patients having underlying malignancies or lymphoproliferative disorders, and (5) cases of IgG4-RD that where patients did not have MFS. In case series, only cases fitting the criteria were included, while others were not.
The title and abstract screening were performed by two authors (ASV and SST) who strictly followed the inclusion and exclusion criteria. These same authors also performed the full-text screening. Any conflicts were settled by a third author (YC).
Data extraction
Data including study details (author names, year of publication, study design, country of origin), patient demographics (age, gender, race, comorbidities), presenting complaint, symptoms, physical exam findings, number and names of the organs involved, whether outcome was favorable, the status of symptoms after treatment, the size of swelling on radiology or on looking after treatment, the status of laboratory findings after treatment, survival status, cause of death, and the length of follow-up was extracted from the shortlisted articles by two authors (ASV and SST) independently on to a unified Excel Sheet.
Statistical analysis
Means, ranges, and standard deviations were calculated for continuous variables, such as age, while frequencies and percentages were tabulated for descriptive data. Significance analysis was done via chi-square test on SPSS Version 25 (IBM® SPSS® Statistics; Chicago, IL, USA). A p value of less that 0.05 was considered significant with a confidence interval of 95% (95% CI). In cases where expected values were less than 5, significance analysis was done by Fischer’s exact test instead.
We analyzed whether the relation between the number of organs affected and the outcome, as well as that between number of organs affected and the survival status, was significant. We also checked if there was any significance between number of organs affected and relapse of the condition.
Bias assessment
Risk of bias was assessed using the Joanna Briggs Institute Checklists for case reports 16 and case series 17 by one author (ASV). Case reports were ranked as high quality (low risk of bias, score 7–8), intermediate quality (average risk of bias, score 5–6), and low quality (high risk of bias, score<5). Therefore, case reports having a score greater than or equal to 5 were included for extraction. Case series were ranked as high quality and included for extraction if their scores were greater than or equal to 8 (low risk of bias).
Results
Study selection and bias assessment
After application of filters, 18,962 studies were included for title and abstract screening. The full texts of 530 articles were read, and 116 articles were shortlisted for the final extraction, 112 of which were case reports and 4 were case series.3,18–130 The PRISMA flowchart in Figure 1 shows the flow of articles at each stage of screening.

PRISMA diagram of included studies (n = 116).
All the shortlisted studies were rated as either high or intermediate quality in the bias assessment. The results of bias assessment are summarized in Supplemental Table 3. A chart of studies by year is also presented in Supplemental Figure 1.
Patient demographics
This study included a total of 134 patients with 78 (58.2%) males. The mean age of the patients was 53.6 ± 14.6 (10–78) years. Two patients were from the pediatric population, aged 10 and 15 years. The youngest patient among adult population was 19 years.
A striking majority of studies belonged to Japan (12.8%) and the United States (12.2%), with a combined total of 49 (25.0%) studies originating from these two countries. Other countries of note included the United Kingdom, Netherlands, and Turkey. The country of origin was not significantly related to the number of organs affected, the outcome of disease, or to the relapse status.
In all, 70 (51.4%) patients reported at least one comorbidity, and 28 (20.6%) patients reported more than one comorbidity. Diabetes (9.7%), autoimmune conditions (8.5%), and hypertension (8.5%) were the most common conditions, while other comorbidities included asthma, previous surgeries, and chronic kidney disease.
Presenting symptoms
Due to the multiorgan nature of the disorder, the presenting symptoms are vastly distributed among all organ systems. Table 1 summarizes the frequency of the various encountered symptoms along with percentages and the 95% CI. In short, the most common presenting symptom was pain (47.8%, 95% CI: 39.1–56.6). Locations of pain included the abdomen (13.8%), back (6.9%), head (3.0%), chest (4.2%), etc. Pain was followed by swelling or masses in various body parts as the second most common presenting symptom (35.1%, 95% CI: 27.0–43.8). As with pain, swellings and masses were also present in various parts of the body such as the salivary glands, eye, and abdomen.
Frequency of symptoms.

CI: confidence interval; RAPD: relative afferent pupillary defect.
Organ manifestations
MFS can affect a multitude of organs, organ systems, and anatomical sites. We have evaluated a mean of 2.51 ± 0.78 (2–5) and a median of 2 (interquartile range = 2–3) organs affected. Table 2 shows the proportion of population with number of organs involved. The most affected anatomical region is the retroperitoneum, affecting 86 patients (64.2%). In 20 (14.9%) of these cases, it is affected in combination with the mediastinum. The digestive system (47.0%, 95% CI: 33.4–49.7) is the most highly affected organ system. Individual organ system manifestations, along with 95% CI are mentioned in Table 3. Specific affected organs of note include the pancreas (30.0%). Six (4.5%) cases of pancreatic involvement occurred in association with the salivary glands, while the overall involvement of salivary glands was 8.2%. The lungs (11.2%) and the orbit (25.4%) were also heavily involved. Thyroid manifestations usually present as Riedel’s Thyroiditis, as seen in 26 (19.4%) of patients in our study.
The number of organs/systems affected.

CI: confidence interval.
Organ system manifestations.
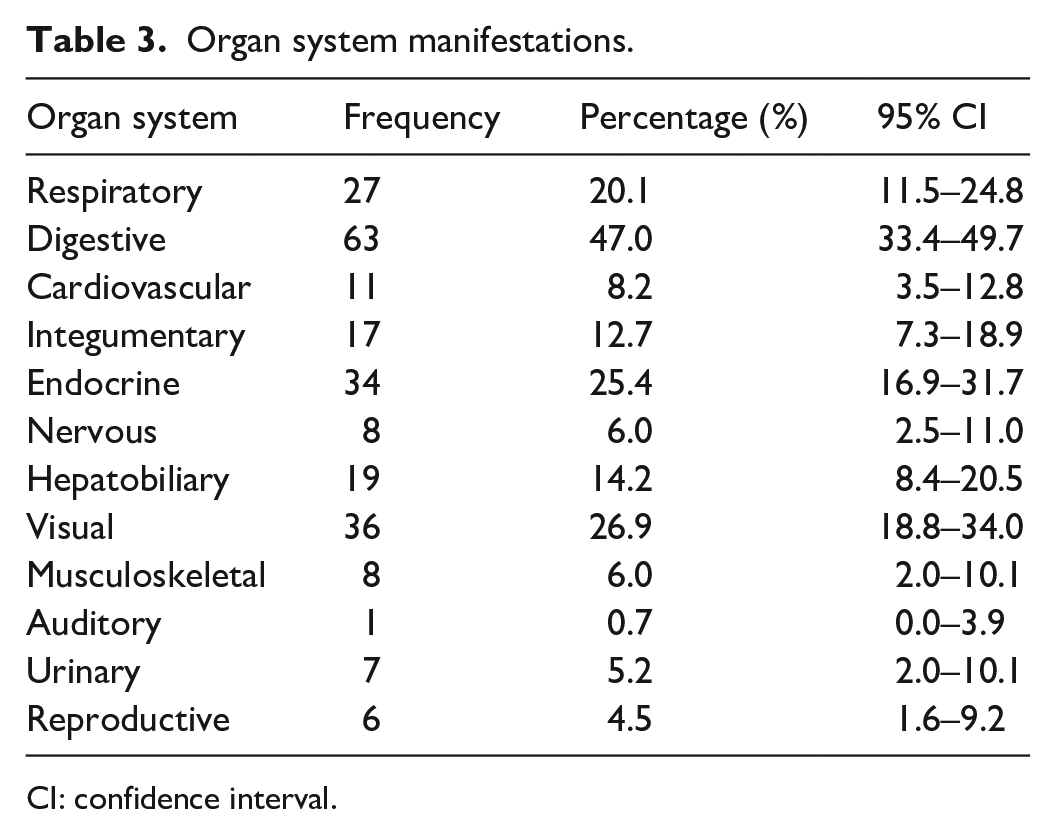
CI: confidence interval.
Patient outcomes
Patient outcomes were either favorable (79.1%, 95% CI: 71.2–85.6) or not favorable (20.9%, 95% CI: 14.4–28.8) over latest follow-up. Outcomes were considered favorable when either the symptoms improved or resolved, the size of swelling or mass decreased or resolved (on inspection or radiology), or when the laboratory results improved or normalized. Length of follow-up was available for 67 (50.0%) of patients, and the mean length of follow-up was 22.3 (0.5–264.0) months. Majority of patients (87.3%, 95% CI: 80.5–92.4) had no relapse over their individual follow-up periods. 7.5% (95% CI: 3.6–13.3) of patients had more than one relapse, while 5.2% (95% CI: 2.1–10.5) of patients had one relapse.
We evaluated a survival status of 91.8% (95% CI: 85.8–95.8) patients as per latest follow-up. Out of the 11 patients who died on follow-up, 6 (4.5%) patients died due to complications associated with MFS. These complications involved GI hemorrhage (one case), respiratory failure (one case), and laparotomy-related complications such as peritonitis or wound infection (four cases). These patients had a mean of 3 (2–4) organs affected, with the retroperitoneum and mediastinum being involved in all cases. Mesentery (two cases), hepatobiliary system (two cases), orbits (two cases), skin (one case), and heart (one case) were also involved.
Favorability, where available, was assessed using measures such as status of symptoms, size of swelling (either on radiology or on viewing), and laboratory results, details of which are summarized in Table 4.
Patient outcomes.

CI: confidence interval.
Relationships such as gender, number of organs involved with outcome, organ system involved with outcome, age, and presence of relapse with number of organs involved and outcome, were all found to be nonsignificant.
Discussion
Among 116 studies, we have obtained data on clinical presentations, number and names of affected organs and anatomical sites, as well as outcomes for 134 patients. To the best of our knowledge, this is the first systematically reviewed study on the presentations, involved organs, and outcomes of MFS. Brito-Zerón et al. 131 revealed in 2014 that 74% of cases of IgG4-RD originated in Japan. Albeit not by such a striking majority, Japan is the country with the most cases in our systematic review as well. Although the relationships were nonsignificant in our study, it may be interesting to see whether the prevalence of the disease in Japan has to do with the already established prevalence of gastric cancers or lymphoma in the country.132,133
According to Goldman’s Cecil Medicine, 4 MFS affects different genders in a male:female ratio of 3:1 with a mean age of presentation from 56 to 64 years. Our study also shows similar demographics, as we have found a higher incidence of the disease in males, with a mean age at presentation of approximately 54 years.
Although no quantitative data could be found on clinical presentation of the disease, multiple sources134,135 state that swelling of the affected region is a common finding of IgG4-RD. This swelling is usually the reason clinical attention is given to the patient, and the disease is uncovered. We found swelling to be the second most common presenting symptom amongst all patients. Edema and pain are defined as typical presentations of MFS by Wilmer L. Sibbit. 4 Eye symptoms such as uveitis are also mentioned. In a study done on pancreatic involvement in MFS, 21 the authors have stated jaundice, anorexia, weight loss, and fatigue as common observations of the disorder. Therefore, it may be said that the common symptoms found in our study are also those that are commonly described in the literature.
In a study by Sekiguchi et al., 136 the median number of organs involved in IgG4-related disease is 2, with an interquartile range of 2–3 organs, much like the mean and median number of organs involved in our study.
We could not find any quantitative data on the incidence of retroperitoneal involvement in MFS, but the high incidence in our study is still well explained by the fact that retroperitoneal fibrosis is considered the most major subset of MFS.
According to a retrospective study done in the United States in 2016, 136 15.0% of patients with IgG4-RD had lung involvement at baseline. This goes well with our estimation of about 11.2%. This same study, based on 166 patients, calculated 35.0% of patients to have pancreatic involvement, close to our number of 30.0%. The study also states that the proportion of patients diagnosed with IgG4-RD having genitourinary system involvement is 14.0%, while we have calculated a similar cumulative proportion of urinary and reproductive system (9.7%) involvement. Cardiovascular system involvement in the retrospective study is 6.0%, while that in our study is 8.2%.
An epidemiological study on IgG4-RD explored the various organ manifestations of the disease including cholangitis, a manifestation hepatobiliary involvement in IgG4-RD. 131 The study calculated the incidence of cholangitis as 19.0%, comparable to our calculated proportion of hepatobiliary system involvement of 14.2%.
In our study, most of the visual system manifestations were related to orbital involvement. Orbital pseudotumor has been heavily implicated as a common finding in MFS. 4 Aylward et al. 137 reported three separate cases of orbital involvement in MFS and went on to describe other cases of similar degree. As with earlier variables, a quantitative measurement of visual system involvement could not be found in the literature, but the high volume of articles describing the condition should not be ignored.
In a study done on the treatment responses of retroperitoneal fibrosis, 138 10.2% of patients had recurrence of the disease. We also found a similar number of patients having recurrences, as the total number of recurrences, whether singular or multiple, is 12.7%.
Sekiguchi et al. 136 found an initially favorable clinical and radiological response to treatment in 131 out of 166 patients (78.9%). Although that study had a much higher recurrence rate (59%) than what we found, the initial favorable response is almost similar.
In a 2019 annual meeting, Wallwork et al. 139 investigated the causes of mortality in a cohort study. In all, 205 patients were included, out of which 10 (4.9%) passed away. However, only four (2.0%) of these patients died due to complications associated with IgG4-RD. Our results on survival status and death due to complications of disease are like what Wallwork et al. have found.
This study has several limitations. The first and most important one is that it does not include multiorgan IgG4-RD, even though it is a disorder relevant with MFS. However, there exists a multitude of cases in the literature that mention single as well as multiorgan manifestations of IgG4-RD. As the focus of our study was just MFS, such articles have not been included to avoid confusion in the article. Further research should be performed to uncover manifestations that may not be present in this study. Not all the studies we included thoroughly explored the details of outcomes; therefore, data on measures such as lab results were limited. There was a lack of standardization between included studies and those used for comparison. Moreover, as most of the included studies belong to high-income areas such as Japan or the United States, this study may only apply to those states. Further case studies in low-middle income countries would be required for a more holistic review.
Conclusion
We strived to collectively analyze all the existing data on MFS and state relevant organ manifestations along with outcomes, as the proportions of organ manifestations were rarely present in the literature. The most common presenting symptom was pain (47.8% of patients), while the retroperitoneum was the most affected anatomical site (64.2% of patients). Outcomes were usually favorable (79.1% of patients), and most patients (91.8%) survived the disorder. With this study, we have managed to achieve an overview of the measures explored. This makes way for further research to be done on the specific organ manifestations of MFS/ IgG4-MFS. Each system may be individually investigated and analyzed, and outcomes analyzed using scale variables, such as quantified laboratory values.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231178046 – Supplemental material for Clinical presentation and organ-based outcomes of Multifocal fibrosclerosis: A systematic review
Supplemental material, sj-docx-1-smo-10.1177_20503121231178046 for Clinical presentation and organ-based outcomes of Multifocal fibrosclerosis: A systematic review by Ahmed Safi Vahidy, Sameer Saleem Tebha, Yeny Chavarria, Sandip KC and Shristi Sharma in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank Dr. Abubakr Yosufi for his contribution in reviewing the article. We want to appreciate Aabiya Arif, Ziauddin Medical College, Karachi, Pakistan for their help during article review and suggesting relevant edits.
Author contributions
ASV, SST, YC, SKC, and SS contributed to research conceptualization and study design. ASV, SST, and YC were responsible for data acquisition. ASV, SKC, and SS were involved in statistical analysis and interpretation. All authors read and approved the final version of the article for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
As this was a systematic review and only used published data, IRB approval was not required.
Informed consent
Not applicable.
Data availability statement
All data are available within the main article and supplemental file.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.