
Abstract
Objective:
This systematic review and meta-analysis aimed to synthesize the available data on rheumatic heart disease in Ethiopia to provide a true figure on the prevalence and distribution of the disease.
Methods:
Different articles were selected using search terms by different search engines like PubMed, Scopus, Google Scholars, and ScienceDirect and also by obtaining hard copies of locally published articles. The search for original research articles was conducted from December 1 to December 30, 2022. Finally, the priority reporting items of the systematic review and meta-analysis guidelines were used for the literature search strategy, publication selection, data extraction, and reporting of review results. Data quality was checked by the author for similarity of study design and inclusion and exclusion criteria.
Results:
A total of sixteen original research articles were included. Nine included articles were from different cardiac patients and seven of the included articles were from children and asymptomatic population. All research papers were summarized in the table clearly with the key information and findings. The prevalence of rheumatic heart disease in cardiac patients from nine included studies was 49.04 (−30.84, 128.92) whereas the prevalence of rheumatic heart disease in children and asymptomatic participants from seven study included was 2.70 (−1181.99, 1187.39) or 27/1000.
Conclusions:
This review and meta-analysis found that the prevalence of rheumatic heart disease in Ethiopia is very high in cardiac patients, children, and the asymptomatic population. Therefore, well-designed and evidence-based national prevention and treatment strategies must be in place to prevent the disease and provide timely treatment for patients.
Introduction
Cardiovascular disease continues to represent a significant disease burden worldwide. However, the epidemiology of cardiovascular disease differs between developing and developed countries. Rheumatic heart disease (RHD) is the leading cause of valvular heart disease and early heart failure in developing countries. Now developing countries face a growing burden of chronic diseases that pose a “double burden” alongside infectious diseases and nutritional problems. 1
In most developing countries, one of the leading causes of cardiovascular disease is bacterial group A Streptococcus infection, which causes acute rheumatic fever (ARF). 2 ARF can lead to RHD. RHD is an autoimmune disease in which an excessive immune response damages heart valves. Increased damage over time can result in heart failure, stroke, valve infections, and death. However, regular penicillin injections can halt progression of RHD in early stages, but heart valve replacement would be necessary for patients with advanced disease. 2
The prevalence of RHD is estimated to be higher in developing countries as compared to developed countries, at 24 per 1000 against 0.3 per 1000, respectively.3 –5 RHD remains the most common form of acquired heart disease in all age groups, accounting for up to 50% of all cardiac hospitalizations in resource-limited countries. 6 In Ethiopian schoolchildren, the prevalence of RHD has been estimated at 4.6–6.4 per 1000 of the children,7,8 and surprisingly enough, not more than 15% of parents of these children knew their children had some form of heart disease related to infection and only 22% receive regular prophylaxis, indicating low knowledge and awareness of the disease. 7
Almost all cases of RHD and associated deaths are preventable.9 –11 Although eliminated in most developed countries, RHD remains a problem in developing countries and affects approximately 15 million people worldwide. 12 In sub-Saharan Africa, it is one of the most common causes of heart failure and has a poor prognosis due to the lack of specialized cardiology centers for optimal case management 13 and the fact that much of the public were ignorant and knew nothing.6,7 RHD is a preventable and treatable cardiovascular disease. However, misconceptions and misunderstandings about the burden of disease cause significant mortality and disability in developing countries. Several studies have also demonstrated RHD to be a major public health problem among non-communicable diseases in Ethiopia.13,14 Therefore, this systematic review and meta-analysis was performed to show that RHD is still a major problem in Ethiopia.
Methods
Study design
A systematic review and meta-analysis was conducted to estimate the prevalence of RHD in Ethiopia. The study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist. 15
Literature search strategy
Literature searches were performed on PubMed, Google Scholar, Scopus, ScienceDirect, and manually by obtaining hard copies of locally published articles. The article search was conducted from December 1 to December 30, 2022. Prevalence, RHD, rheumatic fever (RF), and Ethiopia were used as search terms. For search engines like PubMed, Scopus, Google Scholars and ScienceDirect: ((((Prevalence) AND (rheumatic heart disease)) OR (RHD)) OR (rheumatic heart) and (RF)) AND (Ethiopia))) search terms were used using Boolean operator.
Study selection and eligibility criteria
A stepwise relevance selection/screening was done repeatedly. All available studies and data were included based on the following predefined eligibility criteria. Inclusion criteria include: studies conducted in Ethiopia, discussed the prevalence of RHD, and articles published in English. Exclusion criteria include: articles with duplicate or overlapping data and no full text. The title and abstract were first reviewed to select and avoid duplication of the article. Then, any article that seemed relevant was passed through observation and review of the full-text article. Finally, eligible articles were selected for detailed review and evaluation. Finally, the reference list of all included articles was manually searched for another related article.
Data extraction
All necessary data from included articles were extracted using a standardized data extraction format. The data extraction format incuded primary author, year of study and publication, study population and setting, age and sex distribution of participant, place of study, study design, means of screening for RHD, and conclusion and recommendation.
Quality assessment
Literature search was performed three times with predefined search terms. Then a stepwise relevance selection/screening was also done three times. All available studies and data were included based on the predefined eligibility criteria. Each original study was assessed for risk of selection bias. Study quality was assessed using the Newcastle-Ottawa Scale, adapted for observational and cross-sectional studies, 16 and a 10 point rating was given. It consists of three main sections: methodological quality (five stars), comparability of studies (two stars), and results related to statistical analysis (three stars). The sum of these stars is 10. Based on this, the quality was checked for each study and studies with a score of 5 or above were included.
Statistical analysis
Microsoft Excel 2013 was used for data extraction and results were then exported to Microsoft word 2013. Data was entered to OpenMetaAnalyst version R.3.1.0 software 17 for each study after copying each column from Excel to the software and a meta-analysis was conducted. The pooled prevalence of RHD at 95% confidence interval was determined with a binary random-effect model by the DerSimonian–Laird method. 18
Result
A data abstraction tool was used to construct data from each article selected for review and presented in a table according to the PRISMA protocol. 15 A total of 1301 articles were initially retrieved for the prevalence of RHD in Ethiopia. Among the total, 715 articles were removed after duplicates, and again after screening 543 articles were removed. And also 27 were removed due to eligibility criteria and finally a total of 16 original research articles were obtained for analysis (Figure 1). From the included articles, nine of them were describing the prevalence of RHD from different cardiac patients while seven of the included articles were done on children and asymptomatic population. All research papers were summarized in the table clearly with the key information and findings (Tables 1 and 2).

The PRISMA flow diagram of articles on prevalence of rheumatic heart disease in Ethiopia: A systematic review and meta-analysis.
Prevalence of rheumatic heart disease in cardiac patients in Ethiopia: A systematic review and meta-analysis.

IQ: Interquartile.
Prevalence of rheumatic heart disease in children and asymptomatic population in Ethiopia: A systematic review and meta-analysis.

Description of the included article
All the included 16 articles were obtained from different kinds of study design and were published from 1978 to 2022. Among the total included articles, nine articles were from different cardiac patients (Table 1), while the others were from children and asymptomatic participants (Table 2). From nine articles describing the prevalence of RHD from different cardiac patients, the smallest and the largest sample size was 897 and 9388 respectively. From articles describing the prevalence of RHD from children and asymptomatic participant; the smallest and the largest sample size was 54 and 6275 respectively. All studies used different types of screening methods like questionnaires on sociodemographic variable, clinical finding, laboratory test, record books, and echocardiographic data. In cardiac patients, the highest prevalence 114 (100%) was obtained from patients at Gondar College of Medical Science Teaching Hospital, while the smallest prevalence 22 (13.7%) was obtained from ischemic stroke adult patients who presented to Tikur anbessa specialized hospital. From children and asymptomatic participants, the highest prevalence (56.7/1000) was obtained from studies of rural communities done in Jimma, while the smallest prevalence (3.2/1000) was obtained from public and private primary schools done at Shashemene.
Prevalence of RHD in cardiac patients
In the present systematic and meta-analysis, the pooled prevalence of RHD in different cardiac patients from nine included studies was 49.04 (−30.84, 128.92). There was no heterogeneity observed across the included studies (I2 (variation in effect size (ES) attributable to heterogeneity) = 0.0%), p = 1.000). However, random effect model with restricted maximum likelihood method was used to estimate the pooled prevalence (Figure 2).
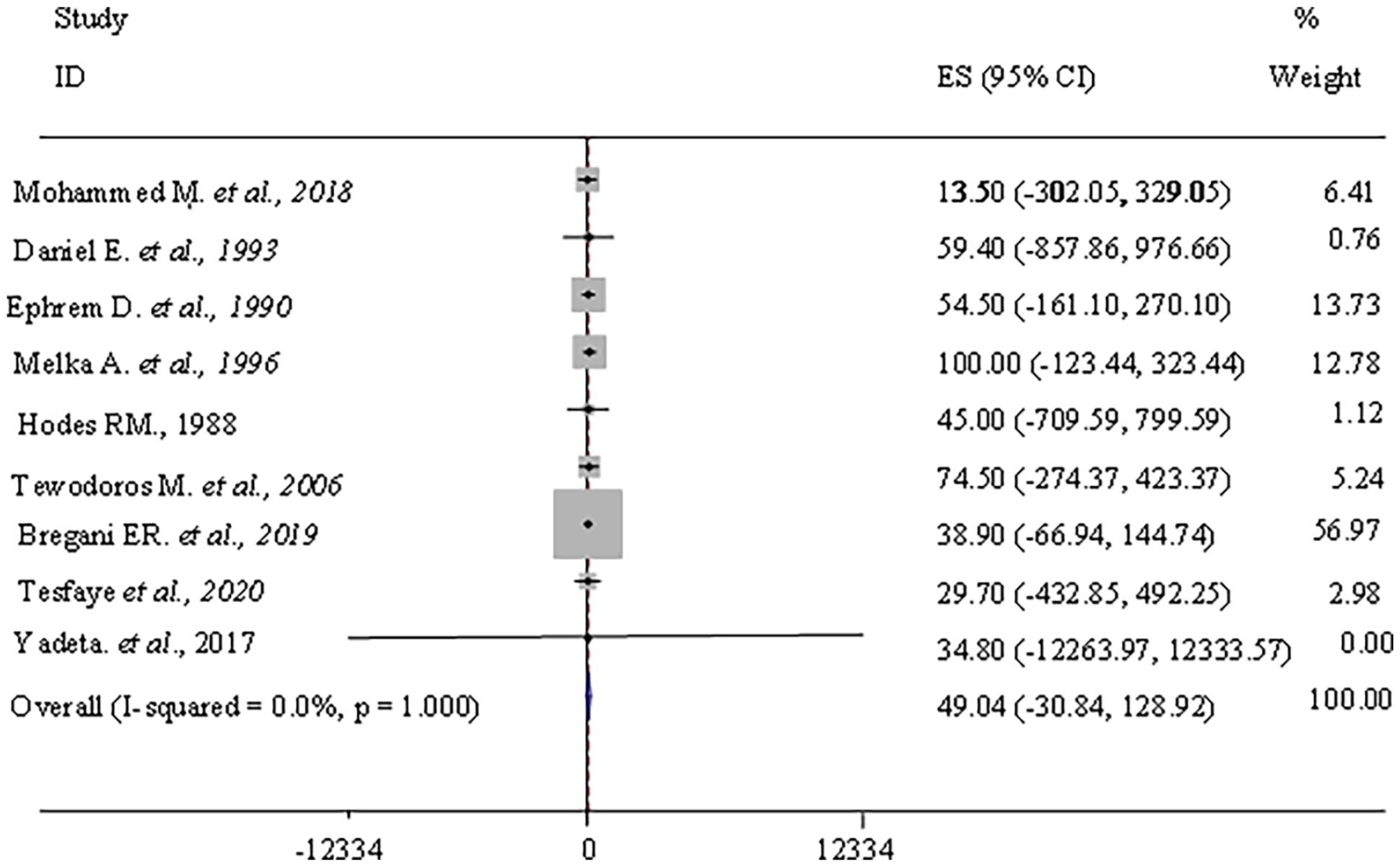
Shows the prevalence of rheumatic heart disease in cardiac patients in Ethiopia: A systematic review and meta-analysis.
Prevalence of RHD in children and asymptomatic participants
In the present systematic and meta-analysis, the pooled prevalence of RHD in children and asymptomatic participants from seven included studies was 2.70 (−1181.99, 1187.39). There was no heterogeneity observed across the included studies (I2 (variation in ES attributable to heterogeneity) = 0.0%), p = 1.000). However, random effect model with restricted maximum likelihood method was used to estimate the pooled prevalence (Figure 3).

Shows the prevalence of RHD in children and symptomatic population in Ethiopia: A systematic review and meta-analysis.
Discussions
RF and RHD primarily affects children and adolescents, especially in low- and middle-income countries where poverty is prevalent and access to health services is limited. People who live in overcrowded or poor conditions are most at risk of contracting the disease. 8 A systematic review of RHD also showed regional variation in the prevalence of RHD in children, with a high prevalence in children of low socioeconomic status, living in overcrowded areas, residing in urban areas, having malnutrition, and with poor access to health services. 35
RHD is a dreaded complication of RF. The term RHD refers to chronic heart valve damage that can occur after a person develops RF.3,9,36 RF begins with a pharyngeal infection, caused by group A (GAS), group C (GCS), or G (GGS) Streptococcus leading to RF, which manifests itself in various ways as an incubation period of 2–3 weeks after the initial episode of pharyngitis. The incidence of RHD is decreasing in developed countries, but remains a major challenge in developing countries. 36
In the present meta-analysis, the pooled prevalence of RHD in various cardiac patients from the nine included studies was 49.04 (−30.84, 128.92). Cardiovascular diseases continue to be a significant burden of disease worldwide, but vary greatly between resource-rich and resource-poor regions of the world. Coronary artery disease remains the major cause of cardiovascular disease burden in most Western countries, but RHD is the leading cause of valvular disease and early heart failure in developing countries. 1 The global prevalence of RHD is estimated at 15.6–19.6 million people (2.4 million children aged 5–14 years) with an annual mortality rate of 1.5%. In Ethiopia, hospital studies showed that 32.8 36 and 39.2% 37 were RHD patients among all cases of heart disease. Of the 457 cardiovascular deaths including cerebrovascular accidents between January 1995 and December 2001; 26.5% (121) of the deaths were due to RHD. 14 Günther also reported 125.3 per 1000 person-year mortality rate during about 7 years follow-up. 13
In the present meta-analysis, the pooled prevalence of RHD in children and asymptomatic participants from seven included studies was 2.70 (−1181.99, 1187.39) or 27/1000. Population and hospital-based studies have also shown that RHD is the number one heart problem in Ethiopian children.13,14 Twenty million people are affected in developing countries with the highest incidence in sub-Saharan Africa. Two million children are affected worldwide, including one million in sub-Saharan Africa. The determinants of the existence of RF and RHD in Africa are poverty; overcrowding; malnutrition; cultural aspect/awareness of the disease being low; lack of resources; inadequate medical expertise; genetic susceptibility to GAS leading to increased streptococcal infection; inadequate diagnosis/treatment; and poor adherence to secondary measures.9,38 –40 The highest rates of RHD are found in sub-Saharan Africa with prevalence of 5.7 per 1000, compared with 1.8 per 1000 in North Africa and 0.3 per 1000 in economically developed countries.41 –43 In Kenya, echocardiography revealed prevalence rates of 62 per 1000, 43 48 per 1000 in Nicaragua, 44 30.4 per 1000 in Mozambique among school-age children, 45 and in Egypt, a rate of 5.1 per 1000 students as previously estimated in the early 1990s. 46
In general, this study showed the true burden of disease is certainly much higher, and due to the lack of high-quality research on the prevalence of RHD, the true prevalence of RHD is underestimated. The overall quality of epidemiological data from developing countries is poor, especially with regard to lack of epidemiological studies and screening. Therefore, well-designed and validated studies involving investigation of the microbiological epidemiology of RHD and evaluation of environmental factors are needed. Studies should also be conducted to assess public perceptions of risk factors.
Strength and limitation of the study
This systematic review and meta-analysis included all published articles showing prevalence of RHD regardless of study parameters, study participants, and means of screening. However, to determine the representative RHD prevalence from these studies, the studies were classified as RHD prevalence studies in different cardiac patients and RHD prevalence studies in children and asymptomatic population. Therefore, the outcome (pooled prevalence) was not significantly affected. This systematic review and meta-analysis included the most popular article search databases, but has limitations in accommodating all search engines.
Conclusions
One of the main challenges in addressing issues related to RHD is the lack of accurate and reliable data to illustrate the true burden of this disease. The results of this study therefore suggest a very high prevalence of RHD in many cardiovascular patients, children, and the asymptomatic population. This result therefore suggests and may help policymakers develop new proven techniques for problem solving as well as for the prevention, control, and elimination of RHD.
Footnotes
Author contributions
TA was involved in designing and conceptualization of the study, collection of the data, performing and interpreting the statistical analysis, and preparing and approving the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.