
Abstract
Objective:
As in many other countries, the Netherlands is facing challenges in the provision of healthcare to its population. To ensure the population remains in good health in coming decades, an integrative approach to the many factors that influence health and health outcomes is needed. Population health management is gaining interest as a strategic framework for systems change in healthcare organisations. Based on population health management, the Dutch HealthKIC has developed the ‘Plot model’, which takes a regional perspective. The aim of this study was to detail the extent to which six prospective regions in the Netherlands were ready and willing to implement population health management using the Plot model, guided by the Five Lenses Model.
Methods:
Using an exploratory focus group reporting study, we involved stakeholders from six regions in the Netherlands. Thematic analysis followed the five predesigned dimensions of a validated cooperation model.
Results:
The study uncovered the potential for realisation of model aims, as assessed by an expert team, regarding shared ambition, mutual gains, relationship dynamics, organisational dynamics and process management. The exploratory questionnaire suggested that organisational dynamics is the least integrated topic in all areas, followed by process management, a finding confirmed in focus groups.
Conclusion:
The building themes of the Five Lenses Model all represent preconditions for the success of integration in the prospective regions. The present study showed that while some themes were reasonably represented in prospective regions, no region was satisfactory for all themes.
Introduction
Like many other countries, the Netherlands faces challenges in healthcare provision to its population. According to the National Institute for Public Health and the Environment (Dutch abbreviation RIVM), increases in healthcare expenditure are expected to continue until at least 2060, despite the population reaching its age peak around 2040. If current policies continue, healthcare expenditures will grow by an average of around 2.8% per year and one in three employees will be working in healthcare by 2060.1,2 The bulk of the costs are related to hospital care (96 billion), while mental healthcare costs are predicted to increase by a factor of five. 1 Population age structure has been changing since the 1960s and as the population continues to age, the burden on a shrinking working force increases, a group which plays a significant role in supporting the well-being of an aging population.3,4 The complexity of these challenges is further increased by the need to offer high-quality care to a demanding population while keeping healthcare systems accessible and affordable.5,6 To ensure people remain in good health in the decades to come, new vision is needed regarding how the current healthcare system is organised and incentivised, and how people are directed through the system. To improve outcomes across the entire healthcare system, a transformation is needed from a reactive, curative ‘Disease and Cure’ approach to a more proactive, preventive societal ‘Health and Wellbeing’ perspective. This will require an integrative approach that weaves together the many factors that influence health and health outcomes.5–8
A comprehensive international population health-value perspective has previously been summarised in the Triple Aim. Triple Aim defines the improvement of a healthcare system as the simultaneous pursuit of three linked aims: improving the individual experience of care, improving the health of populations and reducing growth in healthcare costs.9,10 The experience of care professionals also plays an important role and addressing the needs of this group adds a fourth policy aspect, which increasingly results in the formulation of ‘Quadruple Aim’ healthcare reform initiatives. 7 To help achieve the Triple Aim, population health management (PHM) is one strategy that providers–financiers of healthcare can use to guide systems change. PHM interventions do not focus on the single patient but rather on an entire population or subpopulation, usually defined by a geographic area or population segment and based on complex risk assessment strategies across the complete care continuum. 11 PHM thus refers to the large-scale transformation required for the reorganisation and integration of different services at all levels of integration. These efforts cover public health, healthcare, social care and wider public services with the aim of improving outcomes, and are summarised in what is now referred to as the Triple Aim. 12 This population health-value perspective differs from other perspectives such as value-based healthcare (VBHC) in that the sustainability of healthcare has an additional societal aspect. VBHC strives for the optimisation of service delivery for a specific group of patients in a limited network of providers or focuses on a specific function of the system such as funding.13,14 These alternative perspectives have provided important lessons, including (1) a high risk of ‘waterbed effects’ (i.e. improvement to one part of the system has a detrimental effect on another part) and ‘wrong pocket’ problems (efficiency gains are collected by unintended parties), both of which are associated with interventions that fail to address the full complexity of a system; (2) the monitoring and reimbursement systems elicit a strong focus on repair instead of prevention; (3) a lack of organisational command and investment for system change; and (4) vested interest ‘within silos’ that block innovation across an entire system. 15 While important in themselves, initiatives other than the Triple Aim do not recognise the mutual dependencies between the financing, governance and partitioning of preventive, curative, chronic care and related services regarding health and health spending.
The concept of PHM is still developing and improved definitions emerge regularly. Studies that describe various elements of PHM implementation also appear regularly.16–18 Nevertheless, the most important elements in the implementation process are still ill-defined. Benefitting from national and international experience, including that of examples such as Gesundes Kinzigtal, Kaiser Permanente, Basque Country, Maryland and Massachusetts,19,20 the Dutch NGO ‘HealthKIC’ has now taken on the task of understanding the PHM framework in action. This NGO has developed the ‘Plot model’ (Dutch: ‘Kavel model’) that takes a regional perspective and is founded on three pillars: a new approach to organising differently around one accountable regional body, a different payment and finance model that stimulates health instead of healing and a different approach to monitoring that includes health as well as costs and resources. Since these changes are complex, the context in which they take place is of the utmost relevance. The success or failure of implementation of a PHM strategy will be determined by the specific circumstances within which it is carried out. 20 Imperative for successful change is willingness, propelled by trust in PHM, concerning the transition process and between organisations in the specific region that plans to implement PHM.
When evaluating the integrative processes needed to successfully launch PHM implementation in a specific region, normative integration to achieve connectivity and to add overall value is crucial. The dimension of normative integration can be further explored by using the ‘Five lenses on cooperation model’, a conceptual framework based on the premise that optimal integration requires an integral approach, based on five balanced themes as visualised in Figure 1. 21 The five closely connected themes are (1) Shared ambition (shared commitment of the organisations), (2) Mutual gains (a dialogue about underlying interests of partners that provides an ideal win-win solution), (3) Relationship dynamics (good personal relationships among the partners that contribute to successful integration), (4) Organisational dynamics (appropriate organisation and adequate arrangements) and (5) Process management (process steering among the partners).21,22

Five lenses on cooperation by Bell and colleagues.
The aim of our current exploratory mixed-methods study is to provide a description of the willingness and readiness of six prospective regions in the Netherlands to implement PHM using the Plot model and guided by the Five Lenses Model.
Methods
Procedure
This exploratory focus group reporting study was performed between June and August 2020 and involved six prospective regions within the Netherlands interested in implementing PHM. Based on knowledge acquired during a preceding selection process, a key stakeholder was identified per region. This key stakeholder was often the coordinator or chairperson of existing collaborations at the executive level between the main regional healthcare organisations. This key stakeholder was asked to provide a list of the other main executive level stakeholders involved in regional initiatives. These could be, for example, stakeholders at a hospital, an insurance company, a municipality, social care, education, a general practitioner (GP) practice or a mental healthcare service. The key stakeholders were then asked to complete an online questionnaire, followed by a semi-structured focus group discussion. To describe willingness and readiness to implement PHM, we used the building themes from the five lenses on cooperation model. 21 The study was designed to continue to a saturation point, represented by the moment during data analysis when the same themes continually recur. At this point, additional focus groups provide no new insights.
Questionnaire
Approximately 1 week prior to the date of focus group meetings, the key stakeholders from the six prospective regions received an online questionnaire designed to provide an exploratory baseline insight into the level of integration of organisations in their region with regard to the five building blocks of the Five Lenses Model (Figure 1). The questions were further developed with the support of the Plot model team (Supplemental Appendix I). The Plot model team made the questionnaire based on the validated RMIC Measurement Tool 23 and based on their many years of practical experience. The questionnaire consisted of 23 questions, including at least two questions per topic. The answer scores (four categories) corresponded to four different stages of integration: segregated (score 1), aligned (score 2), coordinated (score 3) and integrated (score 4).
Focus group
Six focus group meetings, including the Plot model expert team (MAB, LV and/or CV) together with stakeholders from the six regions, addressed a topic list between June and August 2020. Five focus group meetings were live and one online. Prior to each focus group meeting, the baseline questionnaire results were discussed by the expert team to gain an impression of the region. After involved parties provided verbal and written informed consent and after a short introduction, all focus group sessions were audio recorded. During the sessions the trained expert team led the focus groups and was careful to ensure discussion of all topics. They also explained the origin and aims of the Plot model and discussed this with stakeholders. The duration of focus group meetings varied between 81 and 97 min.
Statistical analyses
The questionnaire data were reported as means per component of the different stages of integration (scores 1 to 4) and analysed using SPSS version 21.0 (IBM Corp., 2012, Armonk, NY, USA). The audio-recorded focus group sessions were transcribed verbatim by RNM and a copy of the transcript was sent to the key stakeholder of each candidate region for approval. The focus group transcripts were coded and labelled by RNM and AFTME based on the focus group topic list, discussed with MAB and then analysed using Microsoft Excel (2016).
The results were ordered with regard to the Five Lenses Model into two parts: (1) The explanation of Plot model aims by the expert team (MAB, LV and CV) and (2) The willingness and readiness of prospective regions to implement PHM based on questionnaire results and stakeholder discussions of progress and limitations within each region. RNM and AFTME then discussed the analysis results with MAB. The results of the questionnaires and focus group meetings were pseudonymised. The study was registered and approved by the medical research ethics committee of Leiden University Medical Centre, N20.197.
Results
The designated key stakeholder per region completed the questionnaire and recruited a number of other regional stakeholders for a focus group meeting (Table 1).
Stakeholders in the focus groups per potential plot.
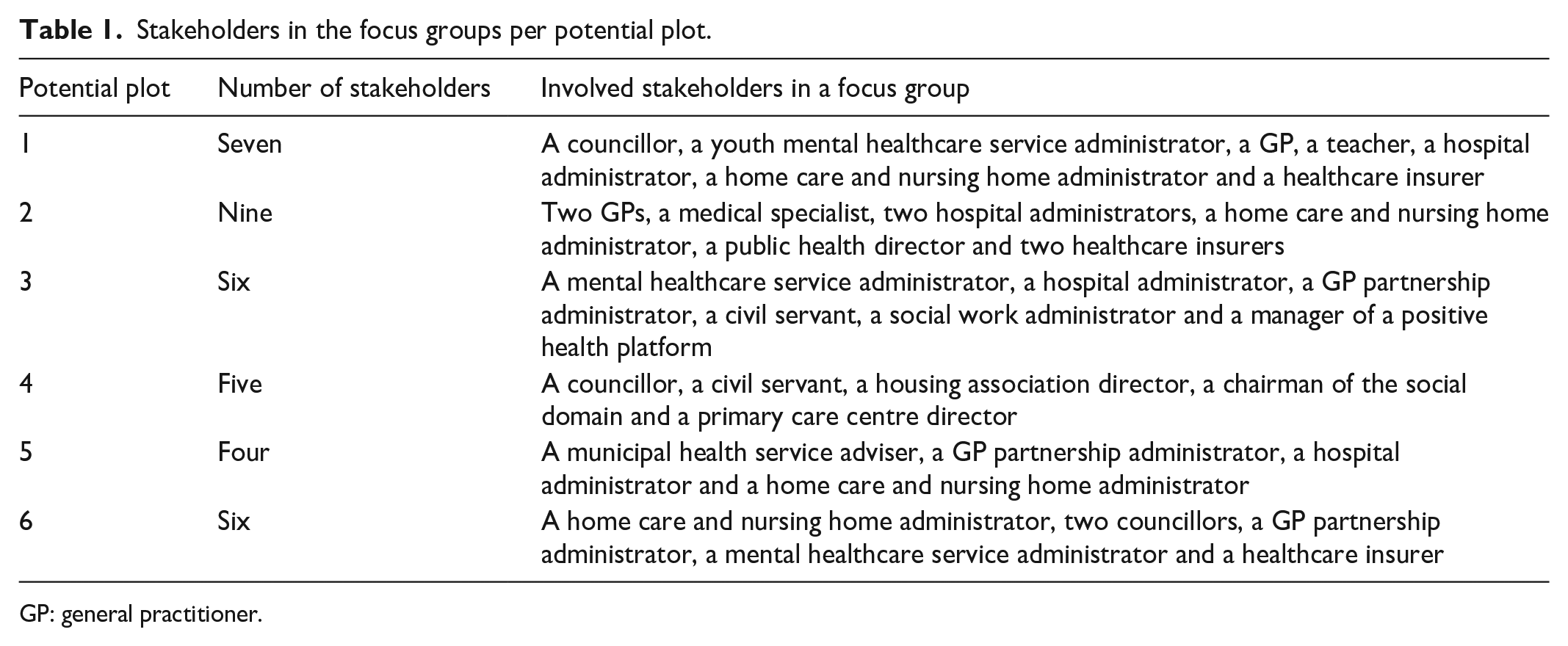
GP: general practitioner.
Questionnaire
The results of the exploratory questionnaire give some insight into the level of integration of organisations across the various regions of the Netherlands with regard to shared ambition, mutual gains, relationship dynamics, organisational dynamics and process management. However, the questionnaire was only completed by one key stakeholder per prospective region. Organisational dynamics (such as sufficient financial resources) seems to be the least integrated topic across all regions, followed by process management (structural monitoring, shared data infrastructure and plans to build shared data infrastructure) (Table 2).
Questionnaire results.

The mean scores correspond with different stages of integration with 1 meaning completely segregated, 2 aligned, 3 coordinated, and 4 completely integrated. x: missing data.
Focus groups
Topic 1: Shared ambition
Explanation of Plot model aims
To launch the large-scale transformational process required for the reorganisation and integration of different services it is necessary to have a shared ambition to shift the main focus from illness to health. The current Dutch healthcare system is structured around curing illness and the efficient delivery of care rather than the premises of health promotion and disease prevention. In contrast, the Plot model builds on the premise that health is more than just the absence of illness and a shared ambition to implement this vision acts as a compass for all cooperative stakeholders. The ambition of the Plot model creators is that organisations from sectors such as healthcare, social care, housing and other partners in a geographically demarcated prospective region embrace a single vision of transformation to a more Health and Wellbeing-focused perspective. Commitment is needed from all involved organisations within the prospective region to confront challenges such as mounting healthcare expenditure, an ageing population and a shrinking workforce. A primary goal is a greater focus on the health process after someone has been treated and discharged from hospital.
Willingness and readiness of prospective regions
During focus group meetings all stakeholders agreed with the ambition of the Plot model for a greater focus on health. They underlined the importance of involving all the various organisations in their region to tackle this challenge together (quote 1). Four of the six prospective regions had already drawn up a regional vision focusing on health in which this specific ambition had been documented by many organisations concerned. In one prospective region, around 30 involved organisations had begun by mapping out the challenges they would face when continuing to provide good healthcare in 2030. At the core of this regional vision is a desire to organise care across organisational and systemic boundaries, focusing more on Health and Wellbeing and less on Disease and Cure, the primary focus at this moment. Two prospective regions had not yet drawn up a regional vision, one of which found the transition to a greater focus on healthcare attractive but had not taken further concrete steps, while the other indicated that various regional organisations were interested in working together and are setting up projects, but still lack an overall regional vision. Even when a vision had been formulated, how action should follow ambition often remained unclear (quote 2). Resolving this issue requires many ingredients from other components of the Five Lenses on Cooperation Model, among which commitment is an important example. Everyone agreed that for the transformation to succeed, greater commitment would be needed (quote 3). Indeed, all prospective regions concurred that the time for transformation is now, as staff shortages, an aging population and increasing chronic disease all underline an urgency that is greater than ever (quote 4).
Quote 1: ‘I believe that we are socially obliged to do this together. Time is an important factor, time and commitment. It is very important to provide long-term, mutual support regardless of management changes, etc. If we can achieve this together it will be very exciting and very economically advantageous. But also very challenging’.
Quote 2, Manager primary care: ‘I notice that there is still insufficient substance to the stated vision. We have all made statements but to really achieve something . . .; it is still difficult to get everyone on board and take action. There seems to be a lack of mutual responsibility’.
Quote 3, Board of directors elderly care organisation: ‘And I find that a little nerve-racking; you trade a degree of autonomy and you take a business-economic risk, because if things go well, you might have less income; it’s important to ensure that it doesn’t become a huge bureaucracy, so governance discussions are key. An incredible amount of commitment is needed’.
Quote 4: ‘The urgency is now greater than ever, the labour market, an aging society, chronic conditions’.
Topic 2: Mutual gains
Explanation of Plot model aims
According to the expert team the aim of the Plot model is to create a system in which courage, leadership and regional willingness are matched with system infrastructure. Building on shared ambition, one common reason for failure is that the interests of the individual organisations are not well served, so it is imperative that stakeholder’s interests are served to an acceptable level. This requires the stakeholders to interact intensively. Different organisations within the prospective regions must think about and agree on how to organise health and care differently or how professionals can provide health and care differently. The organisations also need to consider how turnover and costs can be reduced. Another important element in PHM implementation is therefore an integrated cross-domain business model for health and social care. This means that, for the population in a given region, the costs and revenues resulting from different financial streams are aligned and the consequences for all regional stakeholders are transparent. This also means that certain organisations are critical to the overall success of the model: (1) the healthcare insurer which manages mutual cost savings and contracts, (2) the municipality, and (3) the population of the prospective region which decides whether they support the changes, whether there is a genuine shared interest and whether they find it interesting. The expert team also believes the public or local community should participate. Collaboration creates an idea of ‘stronger together’, but a degree of autonomy is also surrendered. Loss of autonomy and expansion of cooperation must thus be acceptable within a region.
Willingness and readiness of prospective regions
All six prospective regions agreed with the statement that mutual gains are a prerequisite to achieving a successful transition. This perspective creates a joint mission in which organisations relinquish a degree of autonomy in order to work together. They also all agreed that organisations should commit to working together long-term in order to reduce the production incentives together (quotes 5 and 6). Getting colleagues on board and taking action has proven difficult, as stakeholders from the various organisations often failed to recognise their common responsibility (quote 7). Three prospective regions mentioned that there is still some uncertainty regarding how the healthcare insurer in their region views the Plot model (quote 8). They would like the healthcare insurance company to join the discussion in order to ensure that all organisations affected by the transformation experience a soft landing financially; they thus need to have confidence in their future financial position in advance. An example of the tensions elicited by mutual gains in previous projects with a focus on positive health is that changes sometimes resulted in fewer patients being referred to hospital (a success), but as no strategy was in place to address the loss of hospital revenue, this success was often labelled a failure (quote 9). Something that is repeatedly emphasised is that the various parties wish to share common goals but have difficulty developing sufficient mutual trust (quotes 9, 10 and 11). Tension is common due to the fear that little action will be undertaken, resulting in a vision that is not practically purposeful. Investing in building mutual gain is therefore vital to any successful transition.
Quote 5: ‘Production targets and invoicing are such a part of our system, you have to take the necessary time and arrive at long-term agreements together in order to give this a chance of success, a chance for behavioural change to be successful’.
Quote 6, hospital board of directors: ‘If the vision actually involves a fall in hospital income, which I don’t necessarily believe, but I’m not in denial about it either. If you’re talking about a 10-year period and activities that are actually going to decline; well yes, if you see it coming well in advance and can use natural wastage to avoid replacing a surgeon, for example, then it could work because we also have labour market problems. Given sufficient time it’s certainly possible’.
Quote 7, healthcare professional: ‘That’s difficult, isn’t it, because our primary goal in hospital is our task as hospital; that is what we do. And we do it well, but our task is not to do things that are not our task, and then the question is whether these things will be done by someone else. I hear that this is not always the case’.
Quote 8: ‘We are dependent on healthcare insurers and whether they are willing to support the things we have in mind. If they don’t wish to participate, we have to explore other financial options’.
Quote 9, director of public health: ‘I have a question about, for example, a previous project called “more time with the doctor”, which means less hospital referral with potential financial difficulties for the hospital; these are examples that you should also talk about because if you’re really talking about a paradigm, it will affect the entire chain’.
Quote 10, hospital board of directors: ‘You can’t have too many leading organisations; those organisations all have their own demands’.
Quote 11: ‘We really have to avoid a situation in which we all commit but circumstances result in general disappointment. That others say “nice that you have shown that you can manage with less, but we’ll take over now, thank you and good luck”. That is of course fatal for a movement like this’.
Topic 3: Relationship dynamics
Explanation of Plot model aims
According to the expert team, an absolute precondition is that all involved organisations in a potential region are ready and willing to work together in a new way. Stakeholders should be able to find a satisfactory balance between their commitment to cooperation and their own organisational needs. For example, the working culture within a collaboration may be different to that of their organisation. An important factor here is leveraging existing positive energy amongst those who can effectively span existing boundaries, the so-called boundary spanners. Boundary spanners work at and manage the boundary between the various groups and organisations, while helping to cultivate individuals or organisations. Attention to individual, personal and relational aspects of cooperation are important, and programmes aimed at cultural change are essential to the successful transformation and collaborative reorganisation of healthcare. At the outset, organisations tend to agree that positive health is important, but it is critical that organisations also discuss their approach to future complexities in advance. It is important that organisations are able to communicate with each other, that they can count on each other’s support and take the next steps together. This applies even after personnel changes following municipal elections, when a completely new council is elected or when changes occur among hospital directors.
Willingness and readiness of prospective regions
All prospective regions already had good connections with other organisations within their region. However, a mutual connection to focus on positive health was not yet established, regardless of whether a vision had been formulated (quote 12). Trust is an incredibly important building theme within the Five Lenses on Cooperation Model, and it was apparent that greater trust was needed in all cases. While good connections were in place, there were also doubts as to whether the right organisations were involved and concerns regarding the lack of long-term relationships. For instance, there was little or no relationship with the insurer in some cases, and three prospective regions commented that the healthcare insurer did not play an active role in their region, while one region described the relationship with the health insurer as very complex (quote 13). Furthermore, all prospective regions indicated that the will to cooperate was often present, but that there was still a need to focus on cultural change.
Quote 12: ‘Positive health as a prevention model is wonderful; the only thing missing is an overarching organisation or the so called boundary spanners’.
Quote 13: ‘The relationship with the healthcare insurance company is extremely difficult. Whenever we meet we are literally and figuratively sitting opposite each other rather than next to each other’.
Topic 4: Organisational dynamics
Explanation of Plot model aims
According to the expert team, many health-focused projects are initiated in the Netherlands but frequently receive only temporary subsidies. Especially in cases where a domain is overarching, it is rarely a good fit with current funding structures. As a result, many projects and programmes end when the funding stops. Another problem is that organisations are currently judged primarily on short-term cost-related gains and not enough on prevention and stimulating health. The Plot model is designed to remove these obstacles via alternative forms of organisation, finance and monitoring. Another goal of the Plot model is to create an external fund with which prospective regions can finance health interventions aimed at curbing rising healthcare costs. Via shared cost savings, the prospective region can repay the investor and create a revolving fund, which frees up structural funding for organisational consolidation. Effective monitoring of interventions is therefore important in order to properly visualise shared cost savings. Another important element of PHM implementation is the ongoing use of data-driven insights to drive PHM interventions. PHM strives towards trusted and increasingly sophisticated performance measurement as a guide for targeted interventions in regional healthcare systems. The expert team would like to see room for meaning and participation, as well as for conscious choices among specific target groups or for specific challenges within a prospective region. They consider the Plot model a growth model that can initiate one or two area-specific themes per prospective region. To this end, the organisations involved in the prospective region are making a business case that covers plans for the next decade. Together these organisations form the integrator and take joint responsibility.
Willingness and readiness of prospective regions
Three prospective regions wished to improve organisational strength in order to help realise goals (quotes 14 and 15), as well as stating that they seek cohesion in order to kick start collaboration (quote 16). Issues of lack of competence regarding taking action and a need to link capacity across integration levels indicated a need for boundary spanners (quote 17). Several prospective regions underlined their need for greater organisational strength through illustrative examples of interventions or themes they wish to address. One prospective region mentioned that they would like to focus on better follow-up treatment for their patients, such as treatment at home following a hospital-based oncological treatment. Another prospective region indicated that many dedicated workers in their region may need further education. They will begin thematic education during the next academic year and hope to launch prevention by introducing a cultural change aimed at promoting health amongst young adults (quote 18). All prospective regions face a challenge at the organisational level concerning surrender of autonomy, a change that requires a great deal of genuine commitment (quote 19). It also remains unclear which and how many organisations need to be involved to ensure a successful transition (quote 20).
Quote 14: ‘I also want to increase organisational strength to really do things differently or to approach things differently. This is a very important component. Knowledge is not the problem, but organisation and everything that goes with it is not the strongest aspects of care in my experience’.
Quote 15: ‘We have to try something new, otherwise we will keep going in the same circles as we have been doing for years. We worked on this 10 years ago, made some progress but something more has to be done. A real revision is needed. We need to maintain momentum, otherwise we will be only be looking for problems and will lose the initiative. Something somewhere needs to happen now’.
Quote 16: ‘In the end it is just a collection of random projects if I were to be unkind; I am not seeing coherence, especially mutual coherence, spanning organisations’.
Quote 17, director GP organisation: ‘The GP organisation really doesn’t take a negative view. When it comes to the practices, there is still very limited action as regards adopting the philosophy’.
Quote 18: ‘Education is very important. My older colleagues still say that the greatest health gain among fishermen was achieved by educating fishermen’s wives about healthy food. This was not down to us as doctors’.
Quote 19, director GP organisation: ‘And I think that’s exciting, you give away a bit of autonomy. Incredible commitment required’.
Quote 20: ‘I think it depends on which organisations you bring together. Some organisations are further along than others and the chance of success depends on the organisations you choose’.
Topic 5: Process management
Explanation of Plot model aims
According to the expert team, it is important to discuss practical details of stakeholder collaboration and to clearly establish who will lead the implementation process. Plot model experts can support the process but process management must also be based within the region, so a lack of clear agreement can frustrate the cooperation process. For example, it is very important to determine who participates in the collaboration. One challenge facing the Plot model is determining how large a geographically demarcated area should be in which citizens still relate to each other, while ensuring that the population is large enough to make it financially sustainable. In general, upscaling is difficult. In the current system, finance is based on production but in order to make transformation possible and to allow the former model to be phased out, a prospective region needs a considerable portion of the investment fund. Some organisations will generate less turnover at lower cost, meaning current budget flows will be diverted. The hypothesis of the Plot model team is that longer-term investment enables the system to slowly adapt to the financing of health rather than illness. Collaboration requires momentum and process, and promising, concrete results will inspire stakeholders to proceed to the next phase of collaboration.
Willingness and readiness of prospective regions
However, not all prospective regions feel ready at the process management level. One prospective region suggested that first deploying specific interventions within their geographically defined region and only then applying them to the rest of the area may be the most promising approach. To date, they have been unable to properly demonstrate connections between different interventions, and many ongoing projects have no evidentiary value. Two other prospective regions commented that they have many ongoing projects they would like to accelerate but are tied down because of financial limitations. Nevertheless, there is some doubt as to whether an external fund is the answer (quotes 21 and 22).
Quote 21, a GP: ‘When it comes to organising things differently, we are already doing okay but there is room for improvement. But I really believe that care finance is the bottleneck here’.
Quote 22: ‘a number of projects have already proven themselves and we really want to continue them, but we sometimes see resistance from the municipality, health insurer or other organisations. I think that’s where the fund could be of enormous benefit in really getting things going. So that projects can become structurally sustainable. In my opinion there is a very great need for a fund of this type’.
Discussion
This exploratory mixed-methods study provides a description of the readiness and the willingness of six prospective regions in the Netherlands concerning implementation of PHM via the Plot model and based on the Five Lenses Model.
The Five Lenses Model highlights important themes to consider during the selection phase of a complex integration process. Integration requires a coherent set of methods to create connectivity, alignment and collaboration within and between different organisations. Efforts to promote integration for the benefit of patients with complex long-term problems, cutting across multiple services, providers and settings, is referred to as integrated care. 24 All building themes of the Five Lenses Model are preconditions to the success of integration in the prospective regions. Our exploratory questionnaire and focus group results showed that while some themes were more or less present in all potential regions, no region had implemented all themes. Initially, all potential regions need a shared ambition (e.g. vision and mission of the collaboration) 22 and many regions had indeed already drawn up a regional vision. The topic of mutual gain revealed that it is still difficult to coalesce the entire group of stakeholders, as stakeholders from the various organisations did not feel a common responsibility. In terms of relational dynamics, many connections were very good, but with an ongoing need to focus on cultural change, boundary spanners and mutual trust. It was felt that competence to undertake action right away was lacking, and better organisational strength and knowledge concerning process management would be needed to really do things differently. Previous studies nevertheless show that there is a drive to roll out innovative models of healthcare globally, and the importance of being ready and willing to develop and progress new integrated models of care is reinforced by experience. Some of the key learning points from previous examples of innovative integrated care models include (1) relationship building, including a capacity to build bridges, is key to intraorganisational and interorganisational working; (2) relationship dynamics appear to have a significant effect on the final success of a partnership; (3) a mutual gains approach at baseline (e.g. explicitly voicing the interests of the various partners) is a precondition for a successful partnership; (4) the importance of investment to support transformation efforts; and (5) previous transformation initiatives offer valuable lessons for new initiatives.22,25–33 If prospective regions take these lessons to heart, success is not guaranteed but the chances of successful transformation are likely to increase.
Limitations
One potential limitation was that the questionnaire was only completed by one key stakeholder per prospective region, possibly suggesting that results may not be representative. However, as the questionnaire was intended as a baseline overview of the integration level in the prospective regions it is therefore secondary to the qualitative results. Another limitation was the fact that researchers could only interview a group of stakeholders selected by a key stakeholder depending on the burning platform (a specific population segment with a high risk of adverse outcomes),9,34 which included only one or two stakeholders per organisation. The research team therefore recommends further studies, for example due-diligence research.
Conclusions
This study provided a description of the degree to which six prospective regions in the Netherlands are ready and willing to implement PHM using the Plot model and based on the Five Lenses Model. All of the Five Lenses Model building themes qualify as preconditions to the success of integration in the prospective regions. We found that while many themes were more or less present in prospective regions, no region had implemented all themes. We now recommend that, during the initial phases of a transition, greater focus should be placed on mutual interests, establishing relationships (via boundary spanners) and procuring resources for adequate process management.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231160830 – Supplemental material for Reforming healthcare in the Netherlands: practical population health management and the Plot model: A questionnaire survey and focus group study to assess the willingness and readiness of six regions in the Netherlands
Supplemental material, sj-docx-1-smo-10.1177_20503121231160830 for Reforming healthcare in the Netherlands: practical population health management and the Plot model: A questionnaire survey and focus group study to assess the willingness and readiness of six regions in the Netherlands by Rosa Naomi Minderhout, Annefrans FTM van Ede, Leonie Voragen, Carl Verheijen, Hedwig MM Vos, Mattijs E Numans, K Viktoria Stein and Marc A Bruijnzeels in SAGE Open Medicine
Footnotes
Authors’ note
Rosa Naomi Minderhout, MD, is a general practitioner in training and a PhD candidate at the LUMC Campus in The Hague, The Netherlands.
Author contributions
RNM, AFTME, KVS and MAB contributed to the conception and design of the study. MAB, LV and CV conducted the focus groups. RNM and AFTME did the analyses. RNM, AFTME, KVS and MAB contributed to the interpretation of the results. RNM drafted the first version of the manuscript. All the authors critically revised the manuscript for important intellectual content. All the authors made a significant contribution to the research and the development of the manuscript and approved the final version for publication.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the NGO All about Health. All about Health did not play any part in the design, analysis or in the decision to publish the results of this study.
Ethics approval and consent to participate
The study was registered and approved by the medical research ethics committee of LUMC N20.197.
Informed consent
Verbal and written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.