
Abstract
Objective:
This study is designed to assess the pattern of nonadherence, and associated factors among ambulatory patients with epilepsy at Jimma Medical Center, Southwestern Ethiopia, from November 2020 to April 2021.
Methods:
A hospital-based prospective observational study was employed. A consecutive sampling method was used to recruit study participants. Nonadherence was assessed by the Hill–Bone compliance to the high blood pressure therapy scale. A threshold of 18 scores was used to classify adherence status. Epi-Data manager version 4.6 was used for data entry and all statistical analysis was performed by Statistical Package for Social Science 25.0. Multivariable logistic regression was performed to explore associated factors.
Results:
A survey included 334 patients with epilepsy. One hundred twenty-two (36.52%) of the study participants were found to be non-adherent. The factors associated with nonadherence were poor involvement of the patient in the therapeutic decision (adjusted odds ratio = 1.74; 95% confidence interval: 1.04–2.90; p = 0.034), per month income of lesser than1000 Ethiopian birr (adjusted odds ratio = 2.66; 95% confidence interval: 1.03–6.84; p = 0.042), recent seizure episodes (adjusted odds ratio = 1.97; 95% confidence interval: 1.20–3.23; p = 0.007), adverse drug reaction (AOR = 2.13; 95% confidence interval: 1.31–3.47; p = 0.002), and negative medication belief (adjusted odds ratio = 1.28; 95% confidence interval: 1.53–2.25; p = 0.043).
Conclusions:
In our setting, the magnitude of nonadherence was substantially high. Hence, providing regular health-related information about the disease and treatment, supplying free antiepileptic drugs, routine assessment of adverse drug reactions, and a multidisciplinary approach involving patients may improve adherence.
Introduction
Epilepsy is a neurologic condition that affects all people and has no social, racial, or geographic boundaries. 1 Epilepsy is known by repeated seizures involving the entire body or a part of the body accompanied by loss of consciousness and bowel control. 2 Worldwide there are seventy million patients with epilepsy (PWE), of which 90% are living in low- and middle-income countries. 3 Due to multifaceted and complex factors, 90% of PWE in developing regions are not receiving appropriate treatments.4,5
The prevalence of epilepsy in Ethiopia ranges from 0.064% to 2.95% with the highest incidence in ages 1–19 years.6,7 Studies suggested that epilepsy fails to come quickly under control with currently available antiepileptic medicines in about one-third of cases. 4 The probable reasons for uncontrolled seizures were wrong medication, wrong dose, inappropriate seizure classification, comorbidities, medically refractory epilepsy, and nonadherence to antiepileptic drugs.8,9
Nonadherence is a complex and multidimensional healthcare-related problem. It refers to the degree to which the patients failed to respect and follow recommendations from a healthcare provider about taking medication, the daily timing, dosage, frequency, duration of medication use, and executing lifestyle changes.10,11 The causes of nonadherence are multifactorial and can be classified as system-related, patient-related, medication-related, sociocultural, and financial-related. 12 Knowledge about the treatment or diseases, beliefs about medication, resources, and trust in healthcare professionals were critical factors in determining adherence from the patient’s perspective.12–14 Nonadherence to antiepileptic drugs (AEDs) aggravates the consequences of unmet therapeutic outcomes, increases the risk of seizures by 21%, and increases overall mortality by more than three-fold among epileptic patients.15,16
Nonadherence imposes different economic and health consequences like frequent hospitalization, increased morbidity, and mortality along with poor quality of life and poor seizure control.17–19 It is undeniable that many patients experience difficulty in following treatment recommendations. Studies in developed countries showed that 50% of the chronic medication users failed to adhere and in developing countries like Ethiopia the rates are even higher.11,20
The magnitude of nonadherence varied across different continents. It was 66.2% in Brazil, 21 49.3% in Malaysia, 22 68 % in Ethiopia, 23 and 71% in India. 24 Generally, nonadherence to long-term therapies severely compromises the effectiveness of treatment and it is a critical issue in epileptic patients from the perspective of health economics and quality of life. Irrespective of this, a limited study has been conducted on the Pattern of Anti-Epileptic Medications Non-Adherence and Associated Factors in Ethiopia. Accordingly, this study is designed to explore the pattern of nonadherence to antiepileptic drugs and associated factors among ambulatory PWE, in Southwestern Ethiopia.
Methods and materials
Setting, period, and design
A prospective observational study was conducted from November 2020 to April 2021 at the Jimma Medical Center (JMC). JMC is in Jimma town, 352 km from Addis Ababa, Ethiopia. Currently, 160,000 outpatient attendants are being served at this hospital of which 1127 were PWE.
Source population and study population
All people with confirmed diagnosis of epilepsy, and having had regular follow-up at the ambulatory clinic of JMC were our source population, and those patients who fulfilled eligibility criteria were our study population.
Inclusion and exclusion criteria
Inclusion criteria
We included patients with age of 18 years and above, with complete medical records, regular follow-up of six months or above, and willingness to participate in the study.
Exclusion criteria
We excluded patients with acute psychotic features, and those with incomplete medical information.
Study variables
Nonadherence was a dependent variable and our primary outcome of interest as well. Adherence was assessed by using nine items of medication-taking subsections (high blood pressure therapy scale (HBTS)). 25 Each of the nine items contains a four-point Likert-type scale. The score represented as 1 = all of the time, 2 = mostly, 3 = sometimes, and 4 = never. The total Item scores were added to give an overall score of 9–36. A score above a threshold of 18 indicates adherence, otherwise nonadherence.25,26 The involvement of the patients in their therapeutic decision was measured by a questionnaire containing two items. Each of the two items contains a five-point Likert-type scale, 1 = never, 2 = rarely, 3 = sometimes, 4 = most of the time, 5 = all times. The total score ranged from 2 to 10, and a score below the midpoint (<5) indicates poor involvement and the score above the midpoint showed active involvement. 27 Belief about medication questionnaire) 28 is 10-items Likert-type scale divided into two sections, medication necessity, and concern. Having the average score on the medication necessity scale exceeding the average score on the medication concerns scale is a positive belief, if not it is a negative belief. 27
Sample size and sampling techniques
A sample of 334 was calculated using a single population proportion formula by using the following assumptions: Z = 1.96, p = 68% proportion of nonadherence at Yirgalem general hospital, 23 95% confidence level, d = 5% margin of error, n = minimum sample size.

A consecutive sampling method was used to recruit study participants during the follow-up schedule for a medication refill.
Data collection process and quality assurance
The data was collected through interviews and chart review. A pretest was done on 17 PWE at a nearby hospital, and necessary amendments were undertaken. Three data collectors participated in the whole process of data collection. At all stages of the process, the patient’s confidentiality was preserved.
Statistical analysis
Epi-Data manager version 4.6 and Statistical Package for Social Science version 25.0 was used for data entry and statistical analysis. A descriptive statistic was used to explain frequency, percentage, and mean or standard deviation. The association between each independent variable and nonadherence was assessed by performing binary regression and associated factors were identified by multivariable regression. The p-value < 0.05 was used to declare statistical significance.
Operational definitions
Recent seizure episode: is experiencing at least one seizure attack in the last month.
Adherence: Respondents were deemed adherent if their score on nine HBTS questions was above a threshold of 18 points.25,26
Nonadherence: Respondents were deemed non-adherent if their score on nine HBTS questions was below the threshold of 18 points.25,26
Adverse drug reaction is the response to a drug that can be noxious or unintended and occurs at the normal doses used in humans for prophylaxis, diagnosis, or treatment. 29
Results
Demographic distribution of study participants
The survey included a total of 334 PWE. One hundred eighty-three (54.79%) of them were male and 151 (45.21%) of the participants were female. The mean age was 29.91 ± 11.26 years. Majorities, 244 (73.05%) had a formal education, whereas 90 (26.94%) had a nonformal education. With regards to the patient’s involvement in the therapeutic decision-making and medication belief, about one-third (34.13%), of study participants were actively involved, and two-third (65.5%) of participants had positive beliefs about the medications (Table 1).
Demographic distributions of study participants (n = 334).

Therapy and clinical related factors
In this finding, the commonest diagnosed type of seizure was generalized tonic-clonic seizures 221 (66.16%) followed by unclassified seizures 77 (23.05%), and focal seizures 36 (10.77%). About half (48.50%), and one-fourth (25.14%) of participants had a seizure duration of more than 10 years, and 6–10 years, respectively. One hundred thirty-eight (41.31%) of patients had been diagnosed at 11–20 years old, and 117 (35.02%) were reported to have recent seizure episodes. One hundred sixty patients (47.90%) were on a single antiepileptic drug, followed by dual (44.01%), and triple therapy (8.08%). Of the study participants about one-third of the patients had experienced antiepileptic drug-associated adverse drug reactions (ADR) (Table 2).
Therapy and clinical related distribution of study participants (n = 334).

Prevalence and reasons for nonadherence
Our study results showed that 212 (63.48%) respondents were fully adherent and 122 (36.52%) of them were non-adherent. According to the respondent, forgetfulness 46 (37.70%) and unavailability of antiepileptic drugs 35 (28.68%) were the top two reasons for their nonadherence. With regards to which AED the patients were non-adherent, phenobarbital monotherapy 43 (35.24%) and combination with phenytoin 33 (27.04%) were the top two medications to which the patients were non-adherent (Table 3).
Adherence status, reasons for nonadherence, and to which AEDs patients were non-adherent (n = 334).

Scores and distribution of responses to nine items of HBTS (n = 334)
In the adherence assessment scale, 36.52% of the study participant’s adherence score was below eighteen, 29.35% scored 18–26 and 34.13% scored 27–36 (Figure 1).

Distributions of patient score to HBTS (9–36).
Factors associated with nonadherence
The association between nonadherence and different independent variables was identified. From a binary logistic regression analysis all independent variables with a p-value of <0.25 % were transferred to the multivariable logistic regression model. In the multivariable model patient having a monthly income of lesser than 1000 ETB were 2.66 times (adjusted odds ratio (AOR): 2.66; 95% confidence interval (CI): 1.03, 6.84) less likely to be adherent as compared to their counterparts. Patients with recent seizure episodes were 1.97 times (AOR: 1.97; 95% CI: 1.20, 3.23) less likely adherent when compared with their counterparts. Additionally, a group of patients with ADR was 2.13 times (AOR: 2.13; 95% CI: 1.31, 3.47) less adherent than another group of patients. Furthermore, those patients with positive medication beliefs and active involvement in their therapeutic decision-making were 1.28 times (AOR: 1.28, 95% CI: 1.53, 2.25), and 1.74 times (AOR: 1.74, 95% CI: 1.04, 2.90) more likely to be adherent than their counterparts respectively (Table 4).
Association of dependent and independent variables among study participants (n = 334).
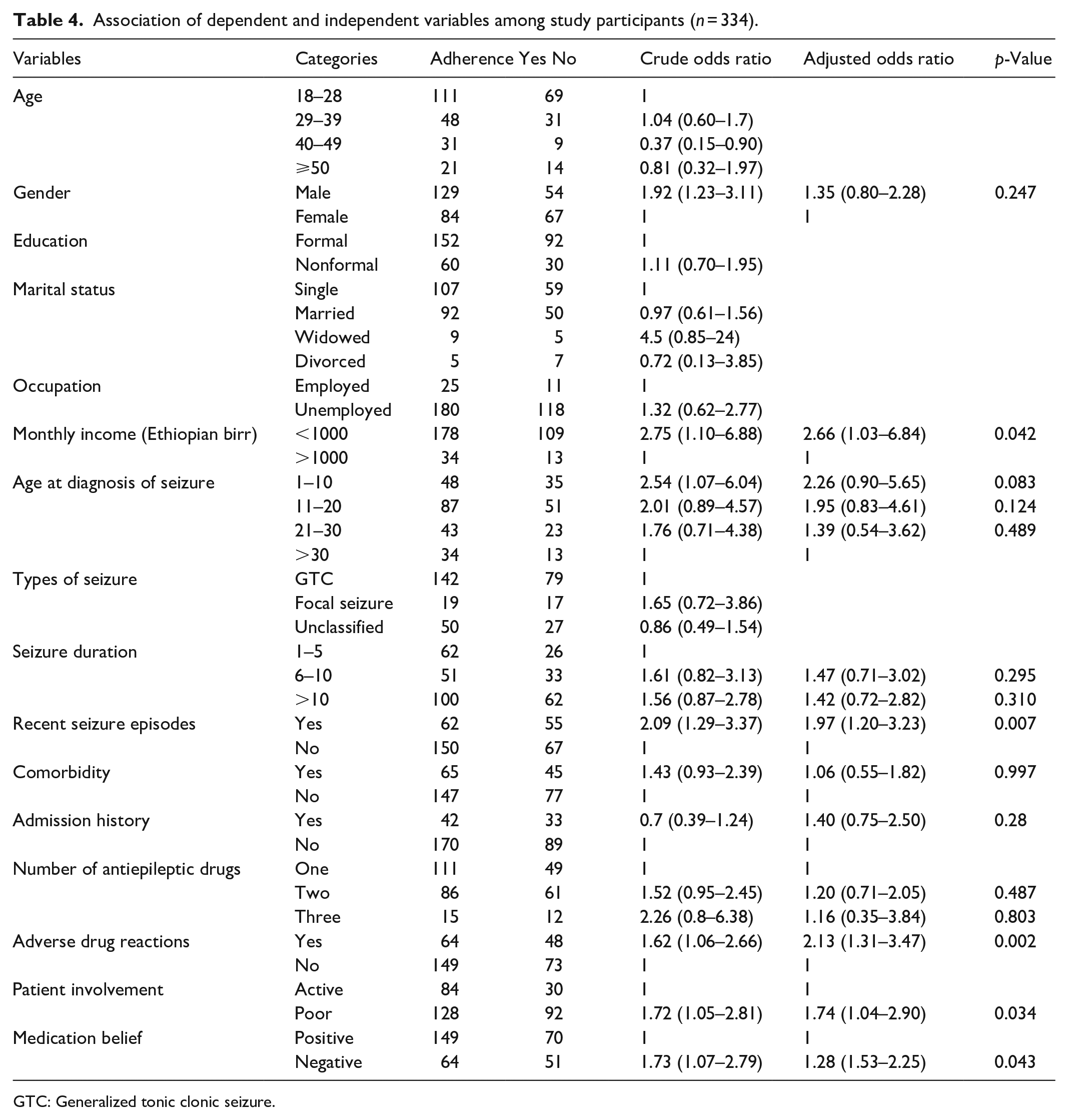
GTC: Generalized tonic clonic seizure.
Discussion
Prevalence of antiepileptic medication nonadherence
In chronic diseases like epilepsy, nonadherence is the critical factor that leads to failure of treatment and disease recurrence. In this study, 36.52% of the participants were found to be non-adherent. In line with the current finding, the study conducted in Debre Markos Referral Hospital, 30 Dilla University Referral Hospital, 31 United Kingdom, 16 Finland, 32 and Mettu Karl comprehensive specialized hospital (MKCSH) 26 identified that 37.8%, 38.1%, 36.4%, 34%, and 40% of participants were non-adherent.
Nevertheless, the reported study from the United Kingdom (20.5%), 21 India (27.7%), 33 and France (21%), 34 showed a much lower level of nonadherence. The justifications for this variation may be, due to differences in the educational status, availability of AED, types of AED used, and cultural differences. In Ethiopia, the most frequently used AEDs are old generations like Phenytoin and Phenobarbital which are associated with higher ADR that may lower the level of adherence. 35
Factors associated with nonadherence
Patient autonomy and active participation in shared decision-making with Healthcare professionals will significantly enhance adherence. 36 Evidence showed that poor involvement of patients in shared therapeutic decision-making increases healthcare-associated complications and treatment-related costs. 37 In the present study, the less likely part of shared decision-making lowered the level of adherence by 1.74 (AOR, 1.74; 95% CI: 1.04–2.90) when compared to actively involved patients. Therefore, healthcare professionals should encourage patients to be a part of shared therapeutic decision-making, as this may enhance patient adherence.
In a developing country like Ethiopia, where there is a shortage of medications, the monthly income of the patient is highly associated with nonadherence. In this study, a monthly income of lesser than 1000 ETB lowered the level of adherence by 2.66 times (AOR, 2.66; 95% CI: 1.03–6.84) as compared to the groups of patients earning more than 1000 ETB monthly. This is supported by the former studies from Ethiopia 38 and Kenya, 39 where the level of adherence was negatively affected by the low monthly income. This is probably due to the unavailability of some AED in public hospitals, patients with low monthly incomes became non-adherent as those medications are unaffordable from non-governmental institutions.
Additionally, in the current study experiencing recent seizure episodes increased the likelihood of nonadherence by a factor of 2.09 (AOR, 2.09; 95% CI: 1.29–3.37) as compared to the groups of patients without recent seizure episodes. A similar finding was reported from India 40 ; Hawassa University Comprehensive Specialized Hospital 41 ; Indonesia 42 ; and Bangladesh. 43 This is because experiencing frequent seizures negatively affects belief about the diagnosis and effectiveness of the current regimen which may lead to failure to take the drugs.
Epileptic patients are highly concerned about the harmful effects associated with their treatment and they may be questioned about the importance of their medicines. 44 The Necessity–Concerns Framework declared that adherence is the interaction between positive and negative beliefs about the medicine. 16 Similarly, in our study, 115 (34.4%) of the participants had negative medication beliefs, and nonadherence was increased by 1.28 factors among this group of patients when compared with positive beliefs patients (AOR, 1.28; 95% CI: 1.53–2.25).
Finally, adverse drug reactions affect adherence and may result in the discontinuation of medications.45,46 In line with this finding, our study revealed that nonadherence was higher by 2.13 among the group of epileptic patients with ADR as compared to the other group of patients without ADR (AOR, 2.13; 95% CI: 1.31–3.47). This finding is augmented by other studies reported from Khartoum and the University of Gondar Referral Hospital.47,48
Limitations
This study was conducted in a single setting which makes it difficult for generalizations. The adherence status, and other important variables including ADR, medication beliefs, and involvement of the patients in the therapeutic decisions were measured based on a self-reported questionnaire which is prone to recall and social desirability bias.
Recommendations
The hospital and ministry of health should work firmly with locally and nationally available suppliers to make AEDs available and affordable for all patients. Healthcare professionals should routinely assess and monitor PWE for signs of adverse drug effects and provide appropriate management with the safest possible alternative drug. Furthermore, health education targeting patients, families, and communities should be given as it may help adherence to their regular follow-up and medication as well. Finally, patients need to be motivated enough to be adherent.
Conclusions
In our study more than one-third of PWE were non-adherent. The primary reasons for nonadherence were forgetfulness and unavailability of antiepileptic drugs. Nearly half of the patients were taking a single antiepileptic drug. Lesser monthly income, negative medication belief, the experience of ADR, and a history of recent seizures were among identified factors associated with nonadherence. Whatever measures that can enhance patients’ belief or seizure control or accessibility to antiepileptic drugs and encourage the patients to be part of the decision-maker would help the patients to be adherent.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231160817 – Supplemental material for Pattern of anti-epileptic medications nonadherence and associated factors at ambulatory clinic of Jimma Medical Center, Southwestern Ethiopia: A prospective observational study
Supplemental material, sj-docx-1-smo-10.1177_20503121231160817 for Pattern of anti-epileptic medications nonadherence and associated factors at ambulatory clinic of Jimma Medical Center, Southwestern Ethiopia: A prospective observational study by Yadeta Babu Bayane and Birbirsa Sefera Senbeta in SAGE Open Medicine
Footnotes
Acknowledgements
Our special appreciation goes to the Jimma University Medical Center, study participants, data collectors, and supervisors for their considerable contributions to conducting this study.
Author contributions
YBB and BSS participated in the proposal development, designing of the study, and formal analysis. YBB and BSS participated in writing up the original version of the document. YBB has checked and modified the manuscript. Both authors agreed to submission and publication with this journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The protocol of this study has adhered to the Declaration of Helsinki’s guidelines and an ethical approval letter was obtained from the Jimma University Institutional Review Board (JUIRB 00025220/2020).
Informed consent
Written informed consent was obtained from the study subjects themselves. All study subjects had the decisional capacity to provide written informed consent. Participation was entirely voluntary, and participants were free to withdraw from the study at any time without any consequence. Confidentiality of all information has been maintained. The JUIRB approved the form of informed consent before the installation of the study.
Data availability
The corresponding author can provide an additional resource upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.