
Abstract
Objective:
The aim of this study was to assess patient reported adverse events and associated factors among epileptic patients taking antiepileptic drugs on follow-up at University of Gondar Referral Hospital.
Methods:
Cross-sectional study was done on 354 adult epileptic patients. Patients who were on antiepileptic drugs for epilepsy treatment for less than a year, those who were below 18 years old, patients with incomplete information on the chart and those who were involuntary or uncooperative were excluded from the study. Data were entered in to SPSS version 20.0 for analysis. Bivariate and multivariate binary logistic regression analysis was done to see factors associated with antiepileptic drugs adverse effect. Level of statistical significance was declared at p ≤ 0.05.
Result:
Generalized tonic clonic seizure was the most common (86.2%) type of epilepsy. A total of 79 adverse events were reported. The most frequently encountered adverse events were fatigue (5.08%), gastrointestinal disturbance (4.24%) and sedation/depression (4.24%). Adverse drug effect of antiepileptic drugs was significantly associated with illiterate educational status, increased number of antiepileptic drugs, no seizure during last follow-up and last year, and 1–5 seizures for the last year.
Conclusion:
About one-sixth of epileptic patients reported adverse drug effects. Adverse drug effects were more commonly seen in patients with low educational status, increased number of antiepileptic drugs, absence of seizure during last follow-up and last year, and 1–5 seizures for the last year. So clinicians should give emphasis for patients with these characteristics to counsel on how to minimize or prevent adverse drug events from antiepileptic drugs or giving reassurance about it if it is minor.
Introduction
Epilepsy is a common neurological disorder which demands immediate medical attention. It is the second leading neurological cause of reduced disability adjusted life years. 1 About 1 of every 10 individuals living a normal life span is expected to have at least one epileptic seizure. More than 50 million people in the world will have recurrent seizures.2,3 The lifetime prevalence of active epilepsy was 7.60 per 1000 persons. 4 In a large community-based epidemiological study, the prevalence of epilepsy in Ethiopia was reported as 5.2 per 1000 population. 5
The main stay of treatment in epilepsy is the use of antiepileptic medications. More than 20 Food and Drug Administration (FDA)-approved antiepileptic drugs (AEDs) are available in the current market. The use of drugs in the management of epilepsy is accompanied by adverse effects such as idiosyncratic reactions, dose-related neurocognitive effects and complications of long-term use.6,7 Comparative studies that assessed the efficacies of AEDs have found equivalency between the different AEDs; therefore, selection of AEDs is mainly dependent on adverse effect profile.8–10 According to HP Bootsma et al., 11 adverse events are more important than efficacy in patients who had taken AEDs for longer periods, and patient reported adverse events determine the long-term retention time. The overall cost of treating epilepsy is impacted by AED adverse events. 12 The health care costs due to adverse effects of antiepileptic drugs was estimated to be as high as US$26.675 per patient per year. 13
The FDA has defined reportable adverse drug experience as “any adverse event associated with the use of a drug in humans, whether or not considered drug related.” 14 Frequency of reported adverse events due to AEDs in a community-based setting was found to be about 60%. 15 Moderate to severe subjective complaints (reported adverse events) due to AEDs were found to be 67% among epileptic patients whose disease was assumed to be controlled. 16 Patients taking two or more antiepileptic medications also reported more side effects than patients on monotherapy.15–17 As compared to the older AEDs, the newer compounds like Gabapentin, Lamotrigine, Oxcarbazepine, Lacosamide, Pregabalin and Levetiracetam seemed to have better tolerability. 18
The goal of epilepsy treatment is to achieve adequate seizure control and improve quality of life without adverse events from the medication. However, adverse events due to AEDs occur frequently and are the main reasons that limit doses to be used for achieving adequate seizure control. 19 Adverse events may also cause impaired treatment adherence. P Perucca et al. 20 reported that significant proportion of epileptic patients discontinue their treatment due to adverse effects. Different studies also confirmed that AED-related adverse events significantly affect quality of life of epileptic patients.21–23
Adverse events due to AEDs finally may lead to hospitalization, switch to more expensive alternatives and failure to achieve treatment goals. Recognition of commonly occurring adverse effects due to AEDs helps to adequately monitor patients and optimize treatment outcome. Early identification of patients who have high risk of adverse event is essential to counter potential treatment failures and to plan interventions accordingly. Therefore, the aim of this study was to identify patient reported adverse events due to AEDs and to determine factors associated with adverse event among epileptic patients at University of Gondar Referral Hospital (UoGRH).
Methods
Study area and period
The study was done at the neurology clinic of UoGRH, North-West Ethiopia. The hospital is located 737 km away from Addis Ababa, the capital city of Ethiopia. It is one of the biggest tertiary-level teaching and referral hospitals in the region. The hospital serves as a referral center for 7 million populations in North Gondar administrative zone and the residents around. It has 400 beds in five different inpatient departments and 14 wards. There are around 2200 epileptic patients on follow-up at the neurology clinic of the hospital. Data were collected from 15 January to 15 April 2017.
Study design and subjects
The study was a hospital-based cross-sectional study. All adult epileptic patients who were taking AED therapy, having follow-up at UoGRH and available at the time of data collection were taken as a study population. Patients who were on AEDs for epilepsy treatment for less than 1 year, those who were below 18 years old, patients with incomplete information on the chart and those who were involuntary or uncooperative were excluded from the study.
Sample size and sampling methods
The sample size was calculated using single population proportion formula, by taking 5% margin of error, 95% confidence level and proportion of reported adverse event as 0.5% (in order to get maximum sample size). In the 3 months of the study period, 1800 patients were expected to come. Since the source population was less than 10,000, the sample was recalculated by using correction formula and it was found to be 324. Finally, we have taken 354 patients as a sample. Systematic random sampling method was used to recruit participants for the study in each day of the data collection process. Every fifth patient was interviewed following physician’s visit.
Data collection procedures
Data were taken from patients’ medical chart and patient interview. Data collection tool was prepared after reviewing different literatures done on the topic.15,17,24–26 The tool was translated in to Amharic and pretested on 18 (5%) of sample population on a different setting (Felegehiwot hospital). Data collection was done by two BSc nurses starting from 15 January to 15 April 2017. Adverse effect–related information was collected by using Amharic version of the questionnaire. Patients were asked to report for the presence of any perceived adverse drug event (ADE) due to their AED in the past 3 months. Patient demographics, diagnosis, co-morbid conditions and type of drugs were collected on the patient charts by using well-designed data extraction format. In order to assure the quality of data, data collectors were trained for 1 day on the documentation and techniques of data collection. Medical chart number was documented to avoid reputation of participants. The principal investigator reviewed all filled data abstraction formats.
Data processing and analysis
Data were entered in to SPSS version 20.0 for analysis. Double entry was applied for accuracy. Descriptive statistics were used for demographic and clinical details. Each drug was counted as 1 whether it was given alone or in combination with others. Both bivariate and multivariate binary logistic regression analyses were done to see factors associated with reported ADEs. All variables with p ≤ 0.3 in bivariate analysis were taken to multivariable model to control for all possible confounders. Level of statistical significance was declared at p ≤ 0.05 levels.
Ethical consideration
Letter of ethical clearance was obtained from ethical review board of school of pharmacy. Letter of cooperation was obtained from UoGRH before going to neurology clinic. Each patient was informed about the objective of the study and oral consent was taken from patients before starting the interview. Privacy and confidentiality were ensured during patient interview and review of patients’ chart. Thus, name and address of the patient were not recorded in the data extraction formats.
Result
Socio-demographic characteristics of study subjects
Three hundred fifty-four epileptic patients were included in the study. Participants’ mean age was 29.1 ± 11.7 years. Majority (61%) of the study subjects were male, a quarter of the participants (25%) were married and 209(59%) of the respondents live in urban areas. Educational status of most (61.6%) of the participants were primary education or below. Majority of the participants (89.7%) were orthodox Christians. More than two-thirds (70.6%) earn a monthly income of below 1500 Ethiopian birr. Table 1 shows socio-demographic characteristics of study participants.
Socio-demographic Characteristics of Study Participants, UoGRH, 2017.

UoGRH: University of Gondar Referral Hospital; AED: antiepileptic drug.
Jehovah.
Clinical characteristics of study subjects
Generalized tonic clonic seizure (GTCS) was the commonest (86.2%) type of seizure. Majority (82.2%) of the patients were on monotherapy. Nearly 90% of the participants have no co-morbid diseases. The mean age of onset of epilepsy was 22 (± 12.1 SD) years. More than two-thirds (70.6%) were seizure free during last follow-up. Table 2 shows clinical characteristics of study participants.
Clinical Characteristics of Study Participants, UoGRH, Northwest Ethiopia, 2017.

UoGRH: University of Gondar Referral Hospital; GTCS: Generalized tonic clonic seizure; AED: antiepileptic drug.
Commonly prescribed drugs for epilepsy
The average AED prescription per patient was 1.18. Most of the patients (69.8%) received Phenobarbital as a monotherapy followed by Phenobarbital with Carbamazepine dual therapy (8.2%). Drugs prescribed for epileptic patients with its frequency are presented in Table 3.
AEDs Used by Epileptic Patients Who Were on Follow-up at UoGRH, Northwest Ethiopia, 2017.
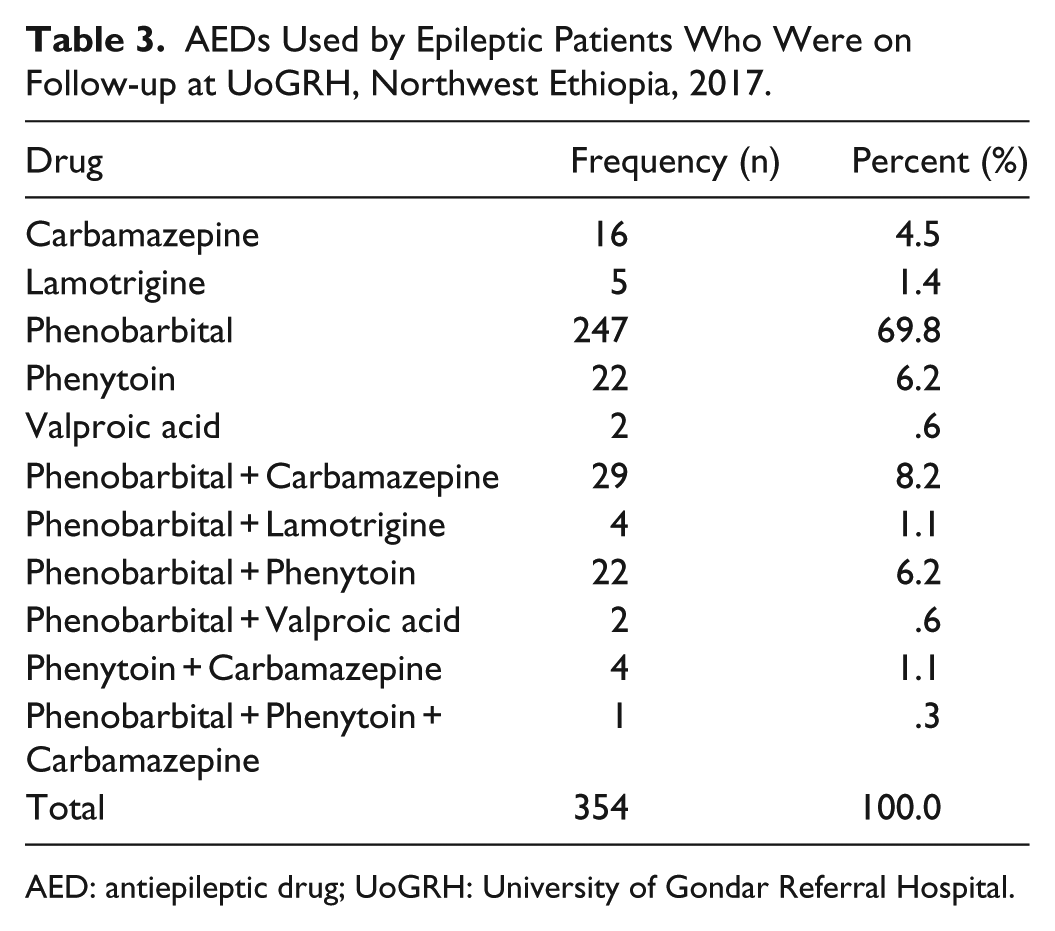
AED: antiepileptic drug; UoGRH: University of Gondar Referral Hospital.
Patient reported adverse drug effects
Fifty-three (15%) of the study participants reported that they experienced adverse effects related to their AED therapy during the last 3 months before the interview. A total of 79 adverse events were reported. The most frequently encountered adverse events were fatigue (5.08%), gastrointestinal (GI) disturbance (4.24%) and sedation/depression (4.24%). Each type of ADEs in relation to the specific drugs is presented in Table 4.
Adverse Effect of Antiepileptic Medications Among Epileptic Patients on Follow-up at UoGRH, Northwest Ethiopia, 2017.
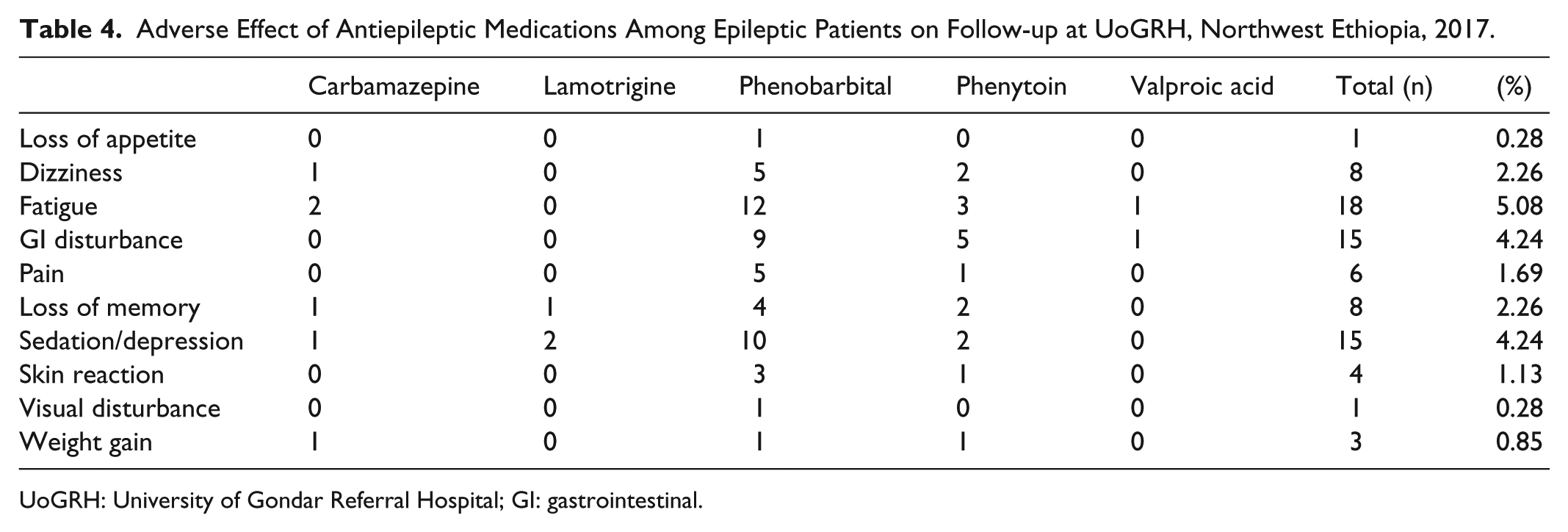
UoGRH: University of Gondar Referral Hospital; GI: gastrointestinal.
Out of the 313 patients who were given Phenobarbital as a mono- or combination therapy, 51 (16.29%) developed ADE. About one-third (32.69%) of patients who were taking phenytoin reported ADE. The rate of adverse events in relation to each type of drugs is indicated in Table 5.
Rate of Adverse Events in Relation to Each Type of Drugs Given for Epilepsy Treatment.
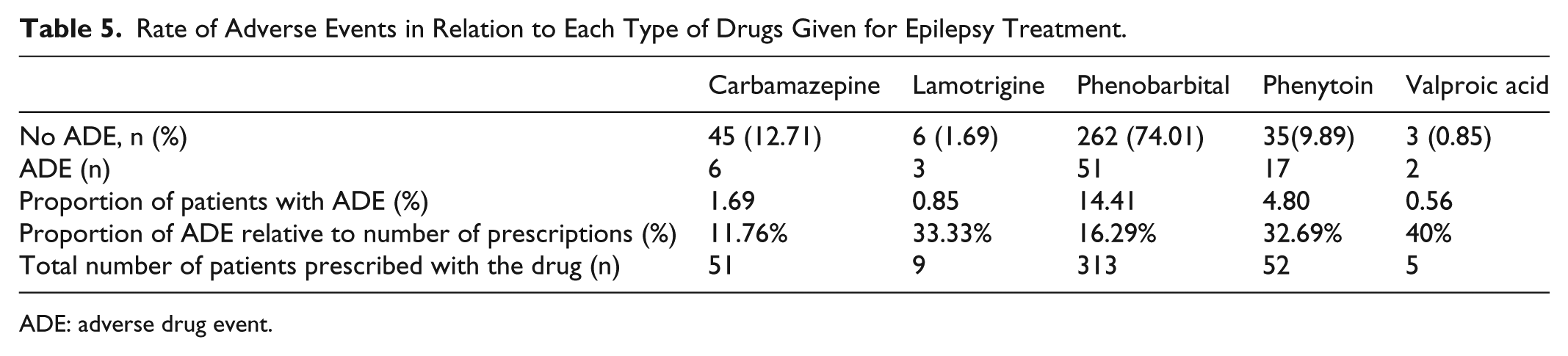
ADE: adverse drug event.
Factors associated with reported adverse medication effect of AEDs
The results of multivariate analysis showed that adverse drug effect of AEDs was significantly associated with illiterate educational status, increased number of AEDs, no seizure during last follow-up and last year, and 1–5 seizures for the last year. Being unable to read and write (illiterate) were 4.9 times (adjusted odds ratio (AOR) = 4.9, 95% confidence interval (CI) = (1.372–17.507)) more likely to experience adverse drug effect than diploma and above educational status. Patients who had no seizure during last follow-up were 6.9 times (AOR = 6.932, 95% CI = (1.152–41.700)) more likely to develop adverse drug effect than those who had greater than five seizure for the last follow-up. Patients who had no seizure and those who experience 1 up to 5 seizures during last year were 13.56 times and 10.9 times more likely to have ADE than those patients who experienced greater than 10 seizures during the last year, respectively. Participants who took monotherapy for their epilepsy were 62.5% more unlikely to experience adverse drug effect than who took more than one AEDs (AOR = 0.375 95% CI = (0.171–0.824)). Table 6 shows association between socio-demographic and clinical characteristics with adverse drug effect of AEDs.
Logistic Regression Analysis Result of Variables Which Have Association with adverse drug effect of AEDs in UoGRH, Northwest Ethiopia; 2017 (N = 354).

AED: antiepileptic drug; UoGRH: University of Gondar Referral Hospital; COR: crude odds ratio; AOR: adjusted odds ratio.
Statistically significant association.
Discussion
Besides seizure control and optimization of quality of life, one of the ultimate goals of epilepsy treatment is reducing adverse effects from antiepileptic medications. The purpose of this study was to identify patient reported adverse events and to find out factors associated with patient reported adverse events among epileptic patients who were taking AEDs at UoGRH.
In the current study, adverse effect of AEDs was reported by 53 (15%) respondents. This finding was in line with the result of the study done by Birru et al. 24 in 2014 which was 17.6%. Similarly, no more than 15% of the patients who visited the outpatient clinic of a tertiary epilepsy center in Kempenhaeghe (Netherland) reported to have side effects. 27 But it was lower than the result of the study conducted in Jimma university specialized hospital which reported 33.4% of patients had experienced adverse events. 25 The study done in Bishoftu General Hospital also reported that 25.8% of epileptic patients experienced an ADE due to AEDs. 26 As compared to our study, lower incidence of adverse drug reactions (ADR) (4.67%) was reported in the study done in Hyderabad. 28 The most common adverse effects reported were fatigue, GI disturbance and sedation/depression. In contrast to our study, headache was the commonest adverse effect recorded in Jimma and Bishoftu.25,26 Birru et al. 24 also reported hypersomnia as the most common adverse effect from AEDs.
It is generally agreed that monotherapy is the primary option in the treatment of epilepsy. But if seizures persist after titration to the highest tolerated dose of a single AED, the patient is given a trial of combination therapy. 29 Most of the respondents (82.2%) in this study took monotherapy for epilepsy. This finding is in line with previous studies done in Ethiopia. Birru et al. 24 reported that 80.35% of epileptic patients at Gondar university hospital received monotherapy. The study done at Bishoftu general hospital and the study conducted on two hospitals in Northwest Ethiopia reported monotherapy was given for 78.6% and 76.7% of epileptic patients, respectively.26,30 But Gurshaw et al. 25 reported that in Jimma university hospital, monotherapy for epilepsy accounts only 54.5%.
The most commonly used monotherapy was Phenobarbital, followed by phenytoin, and the most prescribed dual therapy was Phenobarbital with carbamazepine followed by phenytoin with Phenobarbital. Many other studies in Ethiopia also reported similar results,24,26,30 but in a study done at a tertiary health care facility in northern Nigeria, carbamazepine was the most commonly prescribed medication (91.2%). 31 This difference may be due to the higher prevalence of focal seizure in Nigeria population, which was reported as 58.8% 32 while it is only 1.4% in our setting. In contrast to our study, Alexander B Kowski et al. 33 reported that levetiracetam, lamotrigine and valproic acid were the most commonly used AEDs. The broad spectrum activity of Phenobarbital against many types of seizure and its lower cost makes it to be used more frequently in our setting. 34
Adverse drug effects of AED were 4.9 times more likely to occur in illiterate patients than those who have diploma and above educational status. This may be because illiterate patients’ understanding and communication with health care providers are lesser than educated people which may lead to inappropriate use of medication and then adverse drug effects.
As compared to monotherapy, use of two or more AEDs was significantly associated with adverse drug effects. A similar finding was reported by SG Uijl et al., 16 J George et al., 35 PA Mei et al., 36 A Javed et al. 37 and J George et al. 35 This may be because, as the number of drugs taken by the patient increases, the probability of occurrence of ADE will increase due to additive effects or interactions. Because of this, monotherapy is generally recommended for treatment of epilepsy unless it becomes non-responsive for single agent. Since toxicity depends more on total drug load than on the number of compounds taken, we have to use lower doses of each single drug even when we use poly-therapy then adjust doses based on patient response. 38
Patients who had no seizure during last follow-up were 6.9 times more likely to experience adverse drug effect than those who had more than 5 seizures for the last follow-up (AOR = 6.93), those who experienced no seizure during last year were 13.5 times and those who experienced 1–5 seizures for the last year were 10.9 times more likely to report adverse drug effect of AEDs than those who experienced more than 10 seizures for the last year. This may be justified in the way that patients who had more frequent seizures may worry more about the disease than anticipating adverse effects and they may also consider the adverse drug effects as symptoms of the disease (epilepsy), but patients who were free of seizure may more probably attribute symptoms that they feel to the drugs that they were taking and consider as adverse effect.
The presence of adverse effect from AEDs is additional challenge for epileptic patients besides the burden from the disease itself. As reported by previous studies, ADR significantly affects the quality of life of epileptic patients.19,33 In addition, E Viteva 39 discovered an association between AED adverse events and the severity of perceived stigma. So clinicians involved in the care of epileptic patients should give emphasis for assessing possible adverse effects that the patient may experience and taking essential measures in order to relieve or prevent them.
The result of this study should be interpreted by considering the following limitations. The primary limitation of our study stem from self-reporting. The side effects were subjectively reported so that it may not include adverse effects that were not felt by the patient and which only can be identified by objective parameters like laboratory tests and other diagnostic tools. The cross-sectional nature of the study also limits the establishment of cause-and-effect relation between the AEDs and reported adverse effects. The participants were recruited from one medical center in Northwest Ethiopia. Therefore, the findings may not be generalized to all people living with epilepsy in Ethiopia.
Conclusion
About one-sixth of epileptic patients reported adverse drug effects. The commonest adverse drug effects reported were fatigue, GI disturbance and sedation/depression. Adverse drug effects were more commonly seen in patients with low educational status, increased number of AEDs, absence of seizure during last follow-up and last year, and 1–5 seizures for the last year. So clinicians should give emphasis for patients with these characteristics to counsel on how to minimize or prevent ADEs from AEDs or giving reassurance about it if it is minor.
Footnotes
Acknowledgements
We would like to thank University of Gondar for funding this research project. We are also very grateful to the nursing staffs of chronic outpatient department of UoGRH for their cooperation in the data collection process. MBA had participated in concept development, questionnaire design, write up of the final research and manuscript preparation and finalization. EAM had contributed in concept development, questionnaire design, data analysis and interpretation.
Availability of data and materials
The datasets during and/or analyzed during the current study is available from the corresponding author on reasonable request in preparing this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical clearance was obtained from the Ethical Review Committee of School of Pharmacy, University of Gondar. Ethics approval number was SoP/205/2017. The respondents were informed about the purpose of the study and their consent to participate was obtained orally.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was done with the financial support of University of Gondar.
Informed consent
Verbal informed consent was obtained from all subjects before the study and this was approved by Ethical Review Committee of School of Pharmacy.