
Abstract
Objectives:
We explored the perspectives of older veterans in Gerofit, a Department of Veteran Affairs (VA) supervised clinical exercise program, to understand the factors associated with participation and how the program supported personal health goals.
Methods:
Twenty semistructured interviews were conducted with active and inactive Gerofit participants. We used a hybrid inductive and deductive approach to thematic analysis of transcripts, with the latter informed by the Health Action Process Approach model of behavior change.
Results:
Active and inactive participants differed in their perspectives about how Gerofit impacted their progress toward meeting personal health goals. Active participants noted program features (e.g., schedule, staffing) as facilitators and suggested greater self-efficacy about program participation compared to inactive participants. Both groups perceived the camaraderie with other veterans as a facilitator.
Conclusions:
Exercise program features, including camaraderie, are important factors that affect the ability of older veterans to participate in exercise and achieve personal health goals.
Introduction
Exercise is important in the management of multiple chronic conditions and can improve physical function in older adults, yet the majority of individuals do not participate in exercise.1–3 Older Veterans receiving health care through the Veterans Health Administration (VHA) are more likely to be inactive, defined as participating for fewer than 10 min in moderate or vigorous physical activity daily, compared to those older Veterans who do not receive health care through the VHA. 4 Thus, the VHA is an important setting to provide physical activity interventions to reach those veterans most in need of these services.
Physical inactivity has been associated with loneliness and isolation.5,6 In the National Health and Resilience in Veterans Study, 44% of veterans aged ⩾ 60 reported feelings of loneliness at least some of the time, with the percentage increasing with age. 7 Participating in regular group exercise offers an opportunity for older adults to be engaged in routine physical activity in social settings that promotes social support and an enhanced sense of connectedness. 6
This article features a qualitative evaluation of Gerofit, a VHA group exercise program for older Veterans. The study explored how Veterans—both regular participants and those who discontinued their participation—experienced the Gerofit program, facilitators and barriers to participation (including perceived social support), and how well the program aligned with and supported personal health goals
The Gerofit program
Gerofit is available at 31 VA facilities nationally. Gerofit began in 1986 at the Durham Geriatric Research Education and Clinical Center (GRECC), which is affiliated with the Durham Department of Veterans Affairs in North Carolina. 8 Since 2015, with funding support provided by the VA Office of Geriatrics and Extended Care and the VA Office of Rural Health, the program has expanded to include new sites and modalities (e.g., telehealth). The VA Eastern Colorado Gerofit program was established in 2018 as part of the second wave of national expansion.
Gerofit has been described previously. 8 Briefly, the Gerofit program offers ongoing, continuous enrollment. Potential participants must be at least 65 years old, medically stable, functionally independent, and work well in group settings. Program referrals are typically from primary care providers. Participation in the program is voluntary, and enrolled Veterans may participate as long as they wish (i.e., no limit on number of sessions/no end date). Assessments are performed at multiple time-points (baseline, 3, 6 months, and annually) and involve the evaluation of physical function (e.g., arm curls, chair stands, eight-foot-up-and-go, gait speed, 6-min walk, balance) and health status outcomes. Results of these assessments are reviewed with the individual, in the context of progress over time and to identify future training goals/needs. This is also a behavioral strategy to improve self-efficacy and motivation.
The baseline assessment informs the development of individual exercise prescriptions that are tailored to improve physical function and meet personal health goals. Subsequently, Veterans independently perform their personalized self-paced exercise prescriptions in a group setting in the gym, which is open on specified days/times. All sessions are supervised by an exercise physiologist, and Veteran participation is documented in the electronic medical record. Regular assessments support monitoring progress toward achieving exercise goals. Personalized exercise prescriptions are continuously modified to meet the needs and goals of the Veteran. For example, if a Veteran would like to improve agility on stairs, the exercise program would include a focus on lower extremity strength and balance.
The Eastern Colorado GRECC Gerofit program
Facility and setting: The VA Eastern Colorado Gerofit program is held in a gym on campus. In-person sessions were initially held 3 days per week (Monday, Wednesday, and Friday) between 1 p.m. and 3 p.m. We subsequently expanded hours to 10 a.m. to 2 p.m. to accommodate increasing demand for the program and the morning hours preferred by some participants. On average, 14.8 Veterans use the facility per day. Exercise sessions were staffed by two exercise physiologists. Participants received one-on-one training at their initial exercise visit, but they were then expected to exercise independently with staff oversight.
Evaluation: Quantitative outcomes of Gerofit have been reported elsewhere and include improvements in 10-year mortality, improved physical function, 2 mobility, 9 and surgical outcomes. 10 Our local qualitative evaluation study of older Veteran participant experience aimed to complement well-established objective outcomes. The goal of this program evaluation is to explore the perspectives of the Veterans who have enrolled in the Eastern Colorado Gerofit program. Key findings help elucidate factors influencing exercise initiation and maintenance among Veterans with multiple chronic conditions and complex care needs that will inform the delivery and future adaptations of the Gerofit program. This article contributes a unique, Veteran-centered perspective to the established body of knowledge related to Gerofit.
Methods
Design and conceptual framework
In 2019, we undertook a qualitative evaluation of the VA Eastern Colorado Gerofit program. National VA IRB review determined that this project met the requirements for quality improvement and program evaluation. This project was deemed as quality improvement and not for research and did not require IRB review. Therefore, we do not have a formal approval/waiver number. These activities were not deemed to be human subjects research. For this reason, no written informed consent was required or obtained.
This project was guided by the Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) 11 and the Consolidated criteria for reporting qualitative research (COREQ). 12
We adopted the Health Action Process Approach (HAPA) model of behavior change to guide the study. 13 The HAPA describes behavior change in two phases, the motivational phase (intentions) and the volitional (action) phase.14–16 HAPA contributes a nuanced operationalization of self-efficacy into two phases, motivational and volitional, where the type of self-efficacy varies by phase. In the motivational phase, action self-efficacy (the belief that one can engage in a behavior) and task-self-efficacy (belief that one can complete specific tasks related to a behavior) are involved, whereas in the volitional phase, maintenance self-efficacy (belief that one can cope with challenges related to the behavior) and recovery self-efficacy (belief that one can overcome setbacks to continue the behavior) are involved. 16 Together, these self-efficacy constructs help explain individuals’ beliefs in their ability to initiate, engage in, and maintain behavior change and cope with challenges that emerge at different stages of the behavior change process. HAPA has been applied to study the response of individuals with chronic conditions to lifestyle interventions. 16
Sample for key informant interviews
We conducted key informant interviews with a purposeful sample 17 of active and inactive participants, enrolled between 1 July 2018 and 4 March 2020, and stratified by age, length of time in the program, and distance (in miles) between their residence and the facility. These factors were chosen because previous studies suggest that capability to participate in exercise due to age, habitual participation in physical activity, and physical barriers, such as accessibility of exercise facilities, are factors that influence exercise participation. 18 We defined active participants as Veterans who had not gone more than three consecutive months without attending an exercise session. We defined inactive participants as those who had not participated in the program in over three consecutive months. This evaluation was designed prior the transition to telehealth programming and includes individuals who participated in the in-person Gerofit programming only.
Data collection
Interviews with active participants were conducted during May–July 2019 in-person or by phone, depending on the key informant’s preference. Participants were offered telephone or in-person appointments, and participants scheduled a time with the interviewer for the format they preferred. Subsequently, inactive participants were interviewed between September and October 2020 by phone due to social distancing requirements associated with the COVID-19 pandemic. Two female researchers (KN and SJ), with relevant academic training (masters in medical/applied anthropologist and PhD in health and behavioral sciences; masters in sociology, respectively) and 30 years of combined professional experience doing qualitative research, conducted interviews. Neither of the researchers had professional or treatment relationships with the participants. We called participants explaining our relationship to the program, the purpose of interviews and invited Veterans to take part in an interview at a time of their choosing.
Together with the site lead/medical director (LA), we developed semistructured interview guides, tailored for active and inactive participants. Questions explored topics such as motivations for participating in Gerofit, personal health goals, program expectations, barriers and facilitators to participation, and solicited general feedback to help guide quality and process improvement (Appendix 1). The semistructured interview guides were specifically developed for our program by our project team with extensive knowledge of the program (LA) and qualitative research expertise (SJ and KN). Experienced qualitative researchers on the project team created initial drafts of the interview guides based on priority program evaluation questions and quality improvement information needs determined a priori. Interview guides were reviewed and refined multiple times prior to being used to conduct interviews, enhancing interview question clarity, and the flow and length of the interview guides were the foci of iterative refinement. No additional needed refinements were identified during the course of using the interview guides to conduct key informant interviews. Key questions included
Active Participants: “Tell me about your big, personal healthcare goals.” “What role does Gerofit have in your plan for achieving your goals?” “How do you think Gerofit has affected the role of exercise/physical activity in your life?” Inactive Participants: “What were some of the things that encouraged you to participate or made it easier to participate?” “Ultimately, what led you to stop coming?” “What changes could be made to Gerofit to make it easier for those facing similar barriers/challenges to participate?”
All interviews were approximately 30–60 min in duration, audio-recorded with permission, de-identified, and professionally transcribed. Throughout data collection, the study team (LA, KN, and SJ) met on a weekly basis to process key insights emerging from interviews. Interviews were conducted until theoretical saturation was achieved, at which point no significantly new information was emerging as determined by structured debriefs completed after each interview and ongoing team discussion.19,20
Data analysis
A mixed deductive and inductive approach was used to create a comprehensive codebook. 21 We used the HAPA constructs to explore how active and inactive Gerofit-eligible older Veterans experienced program elements as facilitators or barriers to engaging in regular physical activity and achieving personal health goals. Together, the HAPA, program features, and salient aspects of Veterans’ experience informed the development of an initial codebook. Subsequently, the codebook was expanded and refined as new codes emerged from the thematic analysis of data. Operational definitions of codes were derived a priori, for example, from literature on behavior change theories. To establish interrater reliability, two coders (KN and SJ) first independently coded a single transcript in its entirety, and then met to compare coding, discuss any discrepancies in the application of codes, and any areas where either coder felt ambiguity regarding how to apply codes to specific sections of text. This process was repeated for three consecutive cycles using different transcripts, iteratively refining the codebook, most often by making operational definitions more precise (Appendix 2). Once consistency in applying the codebook was achieved, the remaining transcripts were individually coded. NVivo qualitative data analysis software (QSR International Pty Ltd., Burlington, MA, Version 12, 2018) was used to code data.
Results
Of the 29 active and 15 inactive participants identified and contacted, 20 agreed to participate in interviews (11 active and 9 inactive). Reasons given for declining to participate in an interview included lack of time/interest. Participants included 3 women and 17 men. Mean age was 75.0 (5.9) years, and participants were predominately white (80.6%). The demographics of those who participated in key informant interviews reflected program demographics. Demographics of program participants and interviewees are displayed in Table 1.
Demographic characteristics of participants at enrollment in the Eastern Colorado Health Care System Gerofit Program from 1 July 2018 to 4 March 2020.
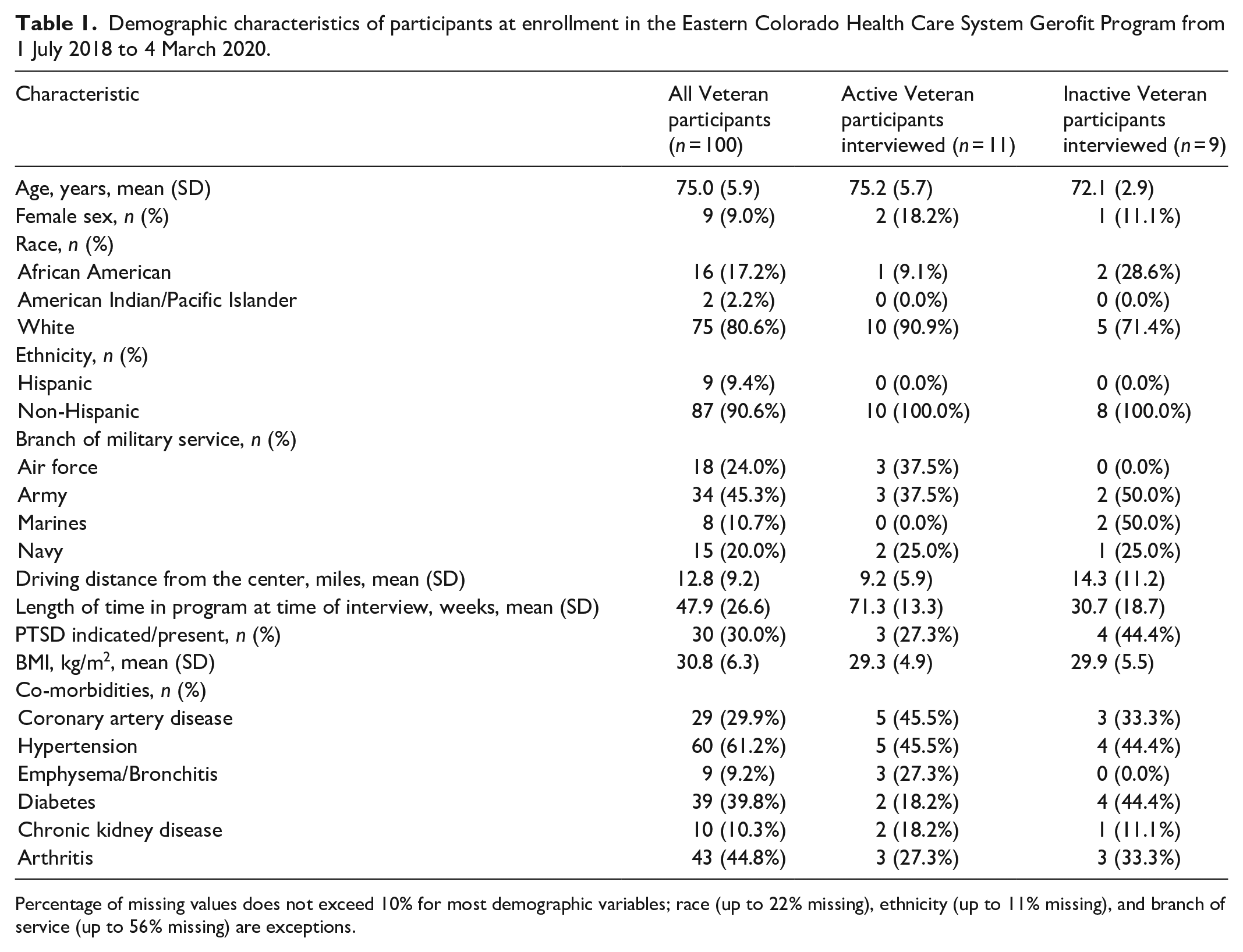
Percentage of missing values does not exceed 10% for most demographic variables; race (up to 22% missing), ethnicity (up to 11% missing), and branch of service (up to 56% missing) are exceptions.
We present the results by three key themes: Gerofit program features facilitating participation in regular exercise, the influence of self-efficacy on initiation and maintenance of regular exercise, and Gerofit as a means to achieve personal health goals. In presenting each theme, we compare and contrast the experiences of active and inactive participants and present selected exemplary quotations below. Appendix 3 includes additional illustrative quotations by theme.
Theme 1. Gerofit program features influence participation in regular exercise
Active and inactive Gerofit participants described how program features such as gym days/times, equipment, staffing, and participation with other Veterans influenced their level of engagement (Table 2). With the exception of opportunities to exercise with other Veterans in a group setting, active and inactive participants who took part in interviews experienced the program features differently. However, even with respect to the camaraderie with fellow Veterans, the degree to which this influenced participation differed between active and inactive participants.
Gerofit program features enabling participation in regular exercise.

Program schedule (days and hours the gym was available): Gym hours, which were limited to certain times and days each week, facilitated participation for active participants, but reportedly limited opportunities to participate for inactive participants. For some active participants, this structure forced them to protect or prioritize this time for exercise by scheduling other obligations around these days/times. For those without this same level of flexibility and/or motivation, the limited hours and days that the gym was open created a structural barrier contributing to inconsistent participation and program attrition, specifically for the inactive participants.
To highlight the contrast in perspectives, one active participant explained that the schedule “. . .made me more accountable. I know the hours are limited, so I can’t just put it off. . . Having the limited hours pushes me.” Another shared that they scheduled other appointments around Gerofit: “I won’t let anything interfere with coming here.” In contrast, an inactive participant shared:
It was just too hard to get there . . . You have to be totally health motivated, have your schedules sync up, and it just wasn’t working for me. If there was some kind of variation [in days and times], [it] might work better.
Program staffing: The Gerofit program includes on-site staff (e.g., exercise physiologists) who provide exercise instruction and supervision for enhanced safety. These specialists also support progress monitoring to help participants achieve personal health goals by tailoring prescription exercise plans based on assessment results and participant goals. Older Veterans who participated in interviews noted that having exercise physiologists available in the gym helped them feel more comfortable pushing themselves. They felt reassured knowing that qualified experts were watching to make sure they were performing exercises correctly to avoid injury. One active participant described that access to Gerofit staff and the quality of the support created a value or benefit that made the extra distance they traveled to get to the Gerofit gym worth it. This participant stated:
I’ve had a long-term membership with a gym that’s closer to my house than [Gerofit], but I like coming here. One of the main reasons [is] the staff. It’s like having trainers. The people here are very knowledgeable and can steer me. They know a lot more, and they’re at a much higher level than what you find in an ordinary gym.
While access to this expertise was noted as a program benefit that was not available in other community-based exercise facilities, some inactive participants described that they sought more personalized or one-on-one support, which was not a component of Gerofit. Such comments highlighted that the program had not met inactive participants’ expectations. One inactive participant shared, for example, “I’m looking for something more like a personal [trainer] . . . [Gerofit] did not meet my expectation of what I, personally, was looking for.”
Camaraderie with other Veterans: The opportunity to exercise exclusively with other Veterans was another unique program feature that distinguished the Gerofit gym from community-based exercise facilities. The ability to exercise alongside other Veterans was viewed positively by both active and inactive participants as it provided an easy point of connection among those with shared backgrounds. For active participants, camaraderie with other Veterans often led to fun and banter, and even friendly competition at times. A feeling that others were “expecting me to show up” heightened a sense of accountability to the gym community that sustained motivation and participation. An active participant described the atmosphere:
We come and socialize. You know, we’re laughing, jok[ing] . . . We respect why each of us [is] there. . . You can go to a place where you’re comfortable, you get along with people, and everybody is on the same page. . . everybody is so good about each other. Everybody tries to mingle with each other and socialize [and] in the same breath, we accomplish our goals of coming there and working out, and that’s what it’s all about, you know, mentally and physically uplift[ing] each other.
Active participants also described the effect of witnessing the commitment to exercise of fellow Veterans, including both those who were in better physical condition and those who had disabilities or injuries to overcome. In either case, other Gerofit participants were sources of inspiration that made active participants expect more of themselves. Witnessing the persistence of fellow Veterans made them less tolerant of their own propensity to make excuses for getting to the gym: “You’ve got other people that are in better health than you are. You’ve got people in worse health than you are. If they can do it, I better get at it and do it. Yeah, that helps.”
Theme 2. Influence of self-efficacy on initiation and maintenance of regular exercise
Distinct types of self-efficacy (e.g., action, task, maintenance, recovery) operationalized in the HAPA framework are defined in Table 3, with illustrative quotes contrasting the experience of active and inactive participants. This section presents related subthemes.
Different types of self-efficacy and their salience to initiation and maintenance of regular exercise among older Veterans.

Action self-efficacy: Action self-efficacy is the belief in one’s ability to engage in exercise. 16 Both active and inactive participants expressed having concerns initially about their ability to participate in an exercise program due to preexisting health conditions. Active participants enrolled despite this concern, acknowledging that while they may be constrained to some degree, it was important to do what they could. One active participant described that their diabetes did not affect exercise participation as much as anticipated, and their Hemoglobin A1C dramatically improved as a result of exercise. Inactive participants, by contrast, had a harder time getting started and/or were not able to participate regularly for a sufficient period to experience the benefits of regular exercise. One inactive participant described, “I’m not that well-disciplined to do exercise, so I just thought it might be a good thing to monitor my exercise. But what happened is I waited a while, and then when I did decide that I wanted to go back, then COVID-19 started.”
Task self-efficacy: Task self-efficacy is confidence in one’s ability to perform particular tasks necessary to initiate and sustain a given health behavior.
22
In the case of exercise, task self-efficacy can pertain to a sense of mastery in the use of exercise equipment and/or performance of specific exercises/physical activities. Stark differences emerged between active and inactive participants in relation to each type of self-efficacy highlighted above. As illustrated in Table 3, task self-efficacy was the exception, with both groups reportedly gaining increased confidence in relation to the proper use of equipment, exercises to perform to pursue health/fitness goals, and how to progress safely to the next level of intensity. While task self-efficacy supported active participants’ engagement in Gerofit, some inactive participants described applying the new knowledge, skills, and task self-efficacy they gained in Gerofit while exercising in community-based programs/facilities or at home. One inactive participant shared:
I know how to exercise. But it’s helpful to learn new ways of exercising for my particular problems, and I thought . . . I would get some instruction on what works well for my neck and shoulders. I learned a lot about the best exercises, and that was very helpful. . .
Maintenance self-efficacy: Maintenance self-efficacy is the belief in one’s ability to cope with or overcome challenges to engaging in regular exercise.
16
Active participants maintained strong beliefs in their ability to engage in exercise, even when encountering obstacles to doing so (such as caregiving responsibilities or medical appointments that disrupted routines). Active participants responded by planning around these challenges—something that was essential given limited gym hours. As one active participant explained, “I’ve missed the last couple of months because we were up here in the mountains. But I plan to get back into it as soon as we get back sometime in September. I try to go three times a week.” Inactive participants, by contrast, tended to acknowledge intrinsic factors such as a lack of discipline or motivation to maintain physical activity. Others may not have had an intention to maintain their participation over the long term; they learned what they could from the program and then continued to use it in other locations. As one inactive participant explained:
In the short term, . . .I used Gerofit for education, motivation, confidence . . . to use the equipment here at [assistive living community]. I went to Gerofit, and then I kind of transferred that information. . . I kind of had the feeling that I probably wouldn’t be there long term, because when I went in, I thought this is an opportunity to learn the weights.
Recovery self-efficacy: Recovery self-efficacy is the belief in one’s ability to overcome new and unexpected setbacks, such as illness or physical injury.
16
Overall, active participants described confidence and determination to resume exercise despite challenges, with the goal to return to a particular level of physical function or conditioning. Recovery self-efficacy is evident in this quote from an active participant: “As soon as my hand is better, I’ll be going back to the weights.” Another active participant described difficulties in regaining strength following a recent injury; they acknowledged that they “couldn’t expect a miracle.” This participant planned to continue exercising to keep working toward their goal: “You can get frustrated and say, ‘Well, the heck with it. Nothing is happening.’ and quit. Or, like I just said, it’s a situation where it takes time to heal. I have to look at it like that. . .” Conversely, an inactive participant with chronic back pain described “no miracle” from Gerofit:
[I was hoping], with doing these exercises, [the] pain would go away, this pinched nerve would snap back into place. . . It didn’t seem to help one bit . . .It was work. And I was still in pain. I kept at it with the hope that something would happen, but [it] didn’t happen. No miracle.
Theme 3. Gerofit as a means to achieve personal health goals
Active and inactive participants identified similar goals and motivations for participating in Gerofit, which included the desire to maintain or improve physical functioning to perform activities of daily living and engage in activities that enhanced their quality of life (Table 4). Participants—active and inactive, alike—noted that prevention served as an impetus for joining Gerofit. Associated goals most often focused on fall risk reduction and a desire to remain independent and avoid long-term care. Other participants saw Gerofit as a tool supporting their recovery, for example, from a surgery, a broken bone, or a fall. Participants listed rehabilitation goals ranging from building cardiovascular and lung capacity after recent procedures to increasing strength, flexibility, and balance in order to decrease reliance on walking aids. One active participant shared, “Hopefully, going to the gym will help me get off this crutch and resume the life that I had. . . I just want to re-establish the life that I had before I broke my hip.”
Personal health goals and reasons for participation.

Still others utilized Gerofit as they sought support for maintaining weight or managing a chronic condition, such as diabetes or chronic pain. One active participant recalled, “My primary goals were to get in shape and to lose weight. I thought that adding the exercise component would only speed things along and would be a perfect complement to it, and it was.” One Veteran, who was no longer attending Gerofit on a regular basis, described how they received guidance on exercises to use for pain management. This inactive participant indicated ongoing use of those exercises.
Discussion
This qualitative evaluation study adds to the body of knowledge of Gerofit, a national exercise program for older Veterans available through the VA. This study of active and inactive participants’ experiences helps inform quantitative measures reported previously regarding program satisfaction, retention, and health outcomes. Specifically, we found that (1) older Veterans valued a personalized (tailored) approach to a prescription exercise program; (2) self-efficacy is important for exercise initiation and maintenance; and (3) group exercise programs help older Veterans meet social-emotional needs while promoting regular participation in physical exercise to improve physical function, engagement in valued activities, and independence. Unique features of Gerofit fostered participant self-efficacy, which enhanced the ability of older Veterans with multiple chronic conditions and complex care needs to achieve personal health goals.
Inactive participants differed from active participants in three primary ways. First, inactive participants’ expectations were not sufficiently met. For example, inactive participants were not always satisfied with the equipment available or with the level of individualized attention provided by exercise physiologists, with some expressing that they expected a personal trainer. Second, inactive participants tended to experience the Gerofit schedule as too restrictive/limiting. Active participants, in contrast, perceived the program days/hours of operation as providing the structure they needed and described how they planned other activities and obligations around Gerofit. Third, some inactive participants did not intend to participate in Gerofit indefinitely. These inactive participants described the value of short-term engagement with Gerofit, such as access to the expertise of exercise physiologists, a baseline performance assessment, a tailored prescription exercise plan, and instruction on the proper use of equipment. Subsequently, they applied this new knowledge at exercise facilities closer to home, such as those available in an assistive living community. Active participants, on the other hand, sometimes traveled greater distances to participate in Gerofit, some relying on public transportation to do so. These active participants were motivated by the camaraderie, enhanced accountability, and inspiration they felt with other Veteran participants.
Findings have implications for the Gerofit program, older Veteran participants, referring providers, and the VA as an integrated health care system.
Implications for Gerofit Programs:
A key value of Gerofit to program participants is access to the knowledge and guidance of exercise physiologists, who provide supervised exercise programs that are responsive to older Veterans’ goals. The continuous presence of exercise physiologists reassures participants that they can safely engage in rigorous exercise as they work to meet health goals. Gerofit exercise physiologists support progress monitoring and increased self-efficacy for exercise in a medically complex patient population. While this support is a key ingredient to Gerofit’s success, exercise physiologists do not function as personal trainers—a distinction that may need to be made in communications about the program.
Some older Veterans may need more scheduling flexibility. To be responsive to this recognized need and the need for social distancing in response to the COVID-19 pandemic, Gerofit is now offered in a telehealth format with synchronous participation via video and has a video library to make on-demand classes available. Telehealth makes it possible to connect Veterans with exercise classes offered through other locations and at different days/times, thus providing more flexibility and a mechanism to maintain reliable access. Telehealth programming requires special attention to technological concerns as many individuals have varying levels of confidence and experience with accessing telehealth programming. However, these may be addressed during the initial one-on-one visit as education improves the ability for older adults to successfully use these technologies.23,24 The Gerofit program currently provides devices when indicated and assistance with this connection upon program enrollment. These options provide various ways for participants to access the Gerofit program and benefit from the support of the exercise staff as well as the camaraderie of other Veterans. In addition, exercise staff can assist individuals with accessing community programs and facilities that may offer additional opportunities to increase flexibility of exercise options.
Gerofit programs should consider adding coaching to address specific initiation and maintenance barriers that surface. Associated evaluation should assess initiation and maintenance self-efficacy as salient participant-level outcomes predicted to support routine engagement in physical activity. 13 These ongoing evaluations will identify participant-specific areas of decreased self-efficacy and allow the exercise physiologist and participant to jointly design a strategy to improve self-efficacy. As HAPA suggests, different strategies will be required during the intention phase and volitional phase. 14 For example, some individuals had more difficulty getting started with the program. In these cases, identification of individual barriers and personal strategies, such as committing to meet another enrolled Veteran at the same time, may be helpful. Likewise, for those Veterans who have been in the program for a long time and suffer a setback in health such as an injury, strategies may include reverting to less challenging exercises until the injury has improved.
Implications for Older Veterans with Multiple Chronic Conditions:
Mobility, longevity, functional independence, and quality of life matter most to older Veterans. Engaging in regular exercise is essential to meet these goals. In addition, the alignment of the exercise program with health goals was important for success. When expectations were met, participants tended to continue in the program, whereas when they fell short, participants discontinued participation. One strategy to address expectations for exercise program might include shifting the expectations or changing the value of the expectations over the course of the program. Larson et al. 25 illustrated that when individuals started an exercise program, the hope was to lose weight or improve physical appearance, but as other health benefits such as increased energy or improved sleep were realized, weight loss and appearance seemed less important compared to these other benefits.
Older Veterans can be some of the most important champions and role models for other older Veterans to initiate and maintain regular exercise. As noted above, Gerofit program staff are important partners in this work, as they support the establishment of realistic goals, tailored exercise plans, and ongoing progress monitoring.
Different experiences with some program features and different levels of self-efficacy reported between active and inactive participants suggest that an even more tailored approach to exercise may be needed to engage some older Veterans. Attitudes about aging impact initiation and maintenance of health-promoting behaviors and the outcomes associated with these behaviors may underlie some of the differences found between active and inactive participants. 26 For example, positive self-perceptions of aging (SPA) have been associated with improved functional health and participation in healthy behaviors, including physical activity. 27 Increasing SPA may be one strategy for improving initiation and maintenance of exercise, but exercise programs may need to add specific interventions focused on changing SPA. Beyer et al. 28 showed that coupling a group exercise program with an intervention to improve SPA significantly improved SPA compared to the control group exercise program that did not receive an SPA intervention.
Implications for referring primary care providers:
Medically complex, older Veterans can participate safely and achieve improvements in physical and mental health. Veterans feel safe exercising in this program and value the education and supervision provided. Further, older Veterans enjoy the social connections of group exercise programs. These qualitative findings may reassure providers who are contemplating referring older Veterans with multiple chronic conditions and complex care needs.
Veteran reported health benefits, such as the enhanced ability to manage chronic conditions and experiencing greater than expected improvements in associated indicators such as Hemoglobin A1C levels. When patients endorse the benefits of exercise and have access to support for regularly engaging in physical activities, providers may not have to spend as much time educating patients about lifestyle interventions and working to manage chronic conditions in the clinic. At least some of this counseling can occur within the program.
Implications for the VA integrated health care system:
Gerofit is a VA program that enhances the patient’s experience. Gerofit supports what matters most to older Veterans with multiple chronic conditions/complex care needs, such as symptom management (sleep, mood, pain), reliance on medications; enhanced ability to engage in activities participants value; enhanced social engagement/connection; physical function, including activities of daily living; quality of life; and clinical outcomes (Emergency Department use, need for follow-up appointments, surgery).
Gerofit can support self-management of chronic conditions and improve health outcomes, thus potentially reducing costs for the VA (e.g., reducing medications, reducing falls, delaying institutionalization)
Limitations
While the results reported here are specific to an exercise program delivered within the VA for older Veterans, findings may offer important insights regarding exercise engagement and onsite/in-person exercise programming for other populations with multiple chronic conditions and lower physical functioning at baseline. There are important limitations to acknowledge, however. For example, this study was limited to a single Gerofit site and, thus, may not be generalizable to other Gerofit programs that may be configured differently or offer different program elements. Although our semistructured interview guides underwent iterative development and refinement, a process that reflected rigorous qualitative research methods, we did not pilot-test these interview guides with Veterans who would have been eligible for the Eastern Colorado Gerofit program as these individuals were unlikely to provide thoughtful feedback due to the limited context of the program. However, our iterative development of the interview guides through weekly planning meetings involving the study team with appropriate knowledge of the program and methodological expertise helped ensure that the questions were clearly written, easy to understand, and adequately captured the information sought related to our project aims (i.e., how Veterans experienced the Gerofit program, facilitators and barriers to participation, and how well the program aligned with and supported personal health goals). This article describes an in-person Gerofit exercise program as it was delivered prior to COVID. Since that time, we have implemented a virtual Gerofit program (Gerofit-to-home). The findings reported here may not be generalizable to this or other Gerofit programs adapted to be delivered virtually. Replicating this qualitative program evaluation with virtual program participants (both active and inactive, including those who transitioned from in-person to virtual participation) is an important future direction. We interviewed active and inactive participants sequentially. Only the active participants were interviewed prior to the COVID-19 pandemic, while the inactive group was interviewed during the COVID-19 pandemic. It is possible that the pandemic may have influenced the perspectives of the inactive group. However, the inactive participants became inactive prior to the pandemic (all participants enrolled in Gerofit during the same time frame, 1 July 2018–4 March 2020), so our investigators made efforts to focus the questions on recalling factors influencing their decision not to continue to participate in Gerofit. While we engaged in a rigorous, team-based iterative data analysis process that involved debriefing each key informant interview and establishing interrater reliability, we did not return transcripts to key informants for comment/correction, nor did we engage them in member checking our theoretically informed interpretations of interview data. Finally, only three women participated in the study reported here. Future studies should examine similarities and differences in participant experience by gender within active and inactive participant groups.
Conclusions
While exercise is important for older adults, participation in and adherence to exercise can be challenging. Flexibility of exercise program schedules and customization of content, such as coaching and working toward specific health goals, are important factors to promote participation. Exercise programs are not frequently accompanied by psychosocial approaches/supports such as self-perceptions of aging or ongoing assessment of expectations, which, if combined, could more effectively support healthy aging. This article contributes a unique, Veteran-centered perspective to the established body of knowledge related to Gerofit. It underscores the value of group-based exercise for older Veterans as well as the need for a more tailored approach to exercise programming in this population.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241271759 – Supplemental material for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program
Supplemental material, sj-docx-1-smo-10.1177_20503121241271759 for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program by Lauren M Abbate, Sarah R Jordan, P Michael Ho, Daniel D Matlock, Kelli D Allen, Sarah Wherry, Toby Wellington, Zach J Buxo, Vanessa Richardson, Courtney McGuire, Megan Pearson, Katherine S Hall and Kathryn A Nearing in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241271759 – Supplemental material for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program
Supplemental material, sj-docx-2-smo-10.1177_20503121241271759 for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program by Lauren M Abbate, Sarah R Jordan, P Michael Ho, Daniel D Matlock, Kelli D Allen, Sarah Wherry, Toby Wellington, Zach J Buxo, Vanessa Richardson, Courtney McGuire, Megan Pearson, Katherine S Hall and Kathryn A Nearing in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241271759 – Supplemental material for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program
Supplemental material, sj-docx-3-smo-10.1177_20503121241271759 for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program by Lauren M Abbate, Sarah R Jordan, P Michael Ho, Daniel D Matlock, Kelli D Allen, Sarah Wherry, Toby Wellington, Zach J Buxo, Vanessa Richardson, Courtney McGuire, Megan Pearson, Katherine S Hall and Kathryn A Nearing in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121241271759 – Supplemental material for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program
Supplemental material, sj-docx-4-smo-10.1177_20503121241271759 for Older Veterans’ perspectives on participation in a clinical exercise program: A qualitative study of the VA Gerofit exercise program by Lauren M Abbate, Sarah R Jordan, P Michael Ho, Daniel D Matlock, Kelli D Allen, Sarah Wherry, Toby Wellington, Zach J Buxo, Vanessa Richardson, Courtney McGuire, Megan Pearson, Katherine S Hall and Kathryn A Nearing in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the Veterans who shared their perspectives to make this work possible.
Author contributions
Lauren M Abbate, Sarah R Jordan, and Kathryn A Nearing were involved in all aspects of the study including concept and design, data collection and analysis, interpretation of the data, drafting, and critical revision of the manuscript for important intellectual content. Sarah Wherry, Toby Wellington, Zach J Buxo, and Courtney McGuire contributed to data collection and critical revision of the manuscript for important intellectual content. Vanessa Richardson was involved with data management and analysis, contributing statistical expertise, and critical revision of the manuscript. P Michael Ho, Daniel D Matlock, Kelli D Allen, Megan Pearson, and Katherine S Hall contributed to interpretation of the data and critical revision of the manuscript for important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the United States Department of Veteran Affairs Rehabilitation Research and Development Service (Merit RX003120); United States Department of Veteran Affairs Health Services Research and Development Service (Career Development Award 1IK2HX003053); the Veterans Health Administration Office of Rural Health, Enterprise-wide Initiative; and the Department of Veteran Affairs Office of Geriatrics and Extended Care, Mentoring Partnership Program.
Ethics approval
National VA IRB review determined that this project met the requirements for quality improvement and program evaluation. This project was deemed as quality improvement and not for research and did not require IRB review. Therefore, we do not have a formal approval/waiver number.
Informed consent
These activities were not deemed to be human subjects research by National VA IRB. For this reason, no written informed consent was required or obtained.
Trial registration
Not applicable.
Disclaimer
The content of this manuscript does not represent the views of the VA or the United States Government.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.