
Abstract
Objectives:
This study aimed to assess achievement of adequate weight gain and identify its associated factors among infants and children with complicated severe acute malnutrition admitted in Kule and Tierkidi refugee camps in Gambella, Southwest Ethiopia.
Methods:
Records of 332 infants and children with complicated severe acute malnutrition were selected by systematic random sampling. Weight gain was calculated for all participants. Patients who achieved weight gain of >5 g/kg/day were regarded as achieving adequate weight gain. Sociodemographic characteristics, season of admission, patients’ anthropometry at admission, source of admission, clinical conditions at admission, types of medications used, length of stay at the centers, and the centers of the treatment were considered as covariates. The adjusted odds ratio and its 95% confidence interval were used to identify factors associated with adequate average weight gain in the multivariable logistic regression.
Results:
In total, 72% of the treated patients achieved adequate weight gain. Treatment at Tierkidi center Adjusted Odds Ratio = 5.9, 95% Confidence Interval: (2.0,16.9), treatment with amoxicillin–clavulanate Adjusted Odds Ratio = 4.1, 95% Confidence Interval: (1.7, 10.0), WFH z-score < −3 Adjusted Odds Ratio = 4.1, 95% Confidence Interval: (1.9, 9.0) and length of stay of ⩽7 days Adjusted Odds Ratio = 2.5, 95% Confidence Interval: (1.4, 4.4) were significantly associated with achievement of adequate weight gain.
Conclusion:
Seven in ten of treated patients achieved adequate weight gain. However, significant proportion of patients still failed to achieve recommended weight gain in refugee camps. Anthropometric indices, type of antibiotics used for treatment, short length of stay, and the treatment center were associated with achievement of adequate weight gain. We recommend that the local antibiotic sensitivity pattern be studied in order to recommend an appropriate treatment regimen for infants and children. Children requiring longer duration have to be given due focus. Inter-center variations have to be narrowed by strengthening follow-up and supervisory supports.
Introduction
Undernutrition continues to be a global public health problem. According to the joint report of the World Health Organization (WHO), United Nations Children’s Fund (UNICEF) and World Bank in 2021, over 45 million children under the age of five are wasted and 149 million are stunted. Two in five of stunted and a quarter of wasted children live in Africa. In 2020, there were 700,000 wasted under-five years children in the East African region. Ethiopia is a country with a very high and a medium prevalence of stunting and wasting with 35% and 7.2% respectively. 1 Malnutrition underlies 45% of deaths in children under 5 years of age, leading to an estimated 3.1 million deaths per year. 2 Stunting and wasting are associated with a five times increase in mortality in children. Further, children with severe acute malnutrition (SAM) are nearly 12 times more likely to die than healthy children if left untreated. 3
Undernutrition can be moderate or severe. 4 SAM is defined by Weight-for-Length or Weight-for-Height (WFH)-z score less than −3 standard deviation (SD) of the median WHO growth standards, and/or a mid-upper-arm-circumference (MUAC) less than 11.5 cm and/or presence of bilateral pitting edema. 5 It is unacceptably high across the Horn of Africa. In 2019, an estimated 9.5 million children were suffering from acute malnutrition in the region, including approximately two million with life threatening SAM. Ethiopia and Sudan had the highest numbers. 6
SAM is classified as uncomplicated and complicated to guide treatment. Malnourished children with severe bilateral pitting edema, or severe wasting (MUAC < 11.5 cm and/or WFH-z score < −3) with medical complications including poor appetite, intractable vomiting, convulsions, lethargy, unconsciousness, high fever (axillary temperature ⩾ 38.5 °C), pneumonia (chest indrawing, fast breathing), dehydration, persistent diarrhea, severe anemia, hypoglycemia, hypothermia (axillary temperature < 35 °C), severe skin lesions and eye signs of vitamin A deficiency are regarded as a complicated SAM and has to be admitted to the inpatient therapeutic feeding program.7,8
SAM is a major public health problem among refugee children. 9 In these settings, in addition to mortality and morbidity, undernutrition reduces people’s ability to recover after a crisis. It impairs cognitive functions, reduces immunity to disease, increases susceptibility to chronic illness, limits livelihoods opportunities, and reduces the ability to engage within the community. 10 It undermines resilience and may increase dependence on on-going support. 10 In 2018, UNICEF and its partners treated more than 3.4 million children with SAM in humanitarian settings. 11
Ethiopia hosts hundreds of thousands of South Sudanese refugees and SAM is one of the most urgent problems refugee children face in Ethiopia. According to the Standardized Expanded Nutrition Survey final report of 2017, the prevalence of Global Acute Malnutrition in the seven refugee camps of the Gambela operation area is 19.1%. Kule and Tierkidi refugee camps have the highest prevalence of SAM from the seven refugee camps. 12 This prevalence is well above the United Nations High Commissioner for Refugees’s acceptable standard of 10% in stable camps. 13
Ethiopia prepared a national guideline to manage SAM. 8 All health facilities in Ethiopia use this guideline to manage undernourished patients. Weight gain is one of the important clinical and program indicators of the success of treatment of SAM patients admitted to stabilization centers. According to the Ethiopian national malnutrition management guideline, infants and children admitted to the stabilization centers should achieve weight gain of 5 g/kg/day during treatment. 8
Studies on the adequacy of weight gain and associated factors among admitted children with complicated SAM were mainly conducted in non-refugee settings and outside of Africa, primarily in Asian countries.14–16 According to a study in Bangladesh, admitted children with complicated SAM achieved a mean weight gain of 10.6 g/kg per day. 15 In India, 57.4% of the total 300 children did not gain final target weight despite giving adequate diet. 16 Potential differences in sociodemographics and population characteristics make it difficult to generalize these results to refugee populations. This shows a scarcity of studies on achievement of adequate weight gain among children treated for complicated SAM at therapeutic feeding units (TFUs) of refugee camps. The purpose of this study was to assess the achievement of recommended average daily weight gain and identify associated factors among South Sudanese refugee children admitted with complicated SAM to the TFUs of refugee camps in Gambella.
Methods and materials
Study area, design, and period
The study was carried out in the TFUs of Kule and Tierkidi refugee camps in Gambela, Ethiopia, using records of infants and children admitted with complicated SAM from January 2019 to May 30, 2021. Kule and Tierkidi camps are two of the seven refugee camps established in Gambela region following the outbreak of conflicts in South Sudan at different times. There are a total of 108,513 refugees in the two camps, with 9341 (8.6%) being children under the age of five. All children aged 6 to 59 months in both camps receive Corn Soya Blend plus (CSB++) complementary food to supplement breast milk and the general food ration with high-energy and nutrient-dense foods appropriate for optimal growth and development. These camps have two health centers, six health posts, four nutrition centers, and two TFUs. Retrospective record review was conducted through review of patient records.
Admission and treatment of complicated SAM in the TFUs
SAM is classified as uncomplicated and complicated to guide treatment. Malnourished children with severe bilateral pitting edema, or severe wasting (MUAC < 11.5 cm and/or WFH z-score < −3) with medical complications including poor appetite, intractable vomiting, convulsions, lethargy, unconsciousness, high fever (axillary temperature ⩾ 38.5 °C), pneumonia (chest indrawing, fast breathing), dehydration, persistent diarrhea, severe anemia, hypoglycemia, hypothermia (axillary temperature < 35 °C), severe skin lesions and eye signs of vitamin A deficiency are regarded as a complicated SAM and have to be admitted to the inpatient therapeutic feeding program.7,8
Treatment and care of patients with complicated SAM is divided into three phases. The first phase is a stabilization phase in which life-threatening problems are identified and treated, specific deficiencies are corrected, metabolic abnormalities are reversed, and feeding is established using F-75. The F-75 has 75 kcal and 0.9 g of protein per 100 ml. This low calorie, low protein diet is preferred at this stage because of the patient’s fragile physiological state and reduced homeostatic capacity. The amount of F-75 per feed is calculated based on the patient’s admission weight. In this phase, all admitted patients are provided with parenteral gentamycin and ampicillin. The ampicillin is replaced by oral amoxicillin after 2 days. If resistance is suspected, patients can be given intravenous ceftriaxone or oral amoxicillin–clavulanate for an appropriate duration. Other medications are provided as required to treat medical complications. 8
The next phase is a transition stage which prepares the patient for the rehabilitation phase. Patients are transferred to this stage if their appetite returns, edema subsides, and all medical complication are resolved. Ready-to-Use Therapeutic Food (RUTF) or F-100 is gradually introduced and the patient’s condition will be carefully monitored. Rehabilitation phase is the time when intensive feeding is given to recover most of the lost weight, and emotional and physical stimulation are increased. RUTF or F-100 are used during the rehabilitation phase. Patients progressing to the rehabilitation phase who consume RUTF should be transferred from TFU to outpatient treatment and monitored weekly at a facility close to his/her home. 8
There are two scenarios of discharging complicated SAM patients. Patients will be discharged to the outpatient treatment if they regain their appetite by consuming 75% of the recommended RUTF, edema subsides, medical complications are resolved, and patient becomes clinically alert and starts gaining weight. Patients can also be discharged after full recovery from inpatient treatment. In this case, the same anthropometric indicator that is used to identify and confirm SAM on admission will be used to determine recovery and discharge from treatment. 8
Population
Source and study population
All infants and children aged 6–59 months admitted to Kule and Terkidi refugee camp TFUs during the period from January 1, 2019 up to May 31, 2021 with the diagnosis of complicated SAM were source populations. All infants and children, fulfilling the eligibility criteria and selected by systematic random sampling from the two refugee camp TFUs were study populations.
Inclusion and exclusion criteria
Inclusion criteria
Records of all children aged 6 to 59 months admitted with diagnosis of complicated SAM to the TFU of the two centers.
Exclusion criteria
Records of children whose register and/or admission charts were incomplete were excluded from the study. In addition, patients who were referred to other facilities after starting treatment, defaulted from treatment, or for whom final outcome is unknown were excluded from the study.
Sample size determination
The sample size was calculated for both objectives (prevalence of achieving adequate weight gain and factors associated with it); the larger sample size was found by using a single population proportion formula for calculation of prevalence, taking the proportion of treated children with SAM who achieved adequate average weight gain as 71.3%, 17 a significance level of 0.05, a 95% confidence interval (CI), a margin of error of 5% and a 10% incompleteness rate. The final calculated sample size was 332.
Sampling technique
A systematic random sampling technique was used to select the study participants. All medical records of infants and children aged 6–59 months, admitted to the two TFUs from January 1, 2019 to May 30, 2021 were listed using the Medical Record Numbers. The study units were proportionally allocated to the two TFUs according to the number of admitted patients. A total of 698 infants and children were admitted for treatment in the two TFUs. From these, 443 were admitted at the Kule TFU, while 255 were admitted at the Tierkidi center. The sampling interval became two by dividing the total population to the sample size (698/332). The first number to start with was selected randomly, and every other record in the list were included in the study thereafter.
Data collection tool and procedure
The data collection tool was developed using the TFUs registration books and individual follow-up charts. The patient cards contained demographic, clinical, medication, and other follow-up information from admission to discharge. The tool was pretested on 50 similar patient records in Ngunyiel refugee camp TFU with Cronbach’s alpha of 0.74. Four clinical nurses and two public health professionals were employed as data collectors. Senior public health professionals supervised the data collection procedures in the two centers.
Operational definitions


Statistical analysis
Data were checked for completeness, coded, entered into Epi-data version 3.1, and exported to Statistical Software for Social Sciences version 25 for cleaning and analysis. Weight and date were exported to Microsoft excel software to calculate individual weight gain, average weight gain, and length of stay from admission to discharge. Age, weight, height, and sex were exported to WHO Anthro 3.2.2 software to calculate weight-for-height z-score (WFH z-score) and height-for-age z-score (HFA z-score).
Before performing the statistical analysis, missing values, the presence of extreme values, and multicollinearity among independent variables were checked. The percentages and frequencies of sociodemographic characteristics and other relevant variables in the study were described using descriptive methods. The factors associated with the achievement of adequate weight gain were identified using bivariable and multivariable logistic regression analysis. Sociodemographic characteristics, season of admission, patients’ anthropometry at admission, source of admission, clinical conditions at admission, types of medications used, length of stay at the centers, and the centers of the treatment were considered as covariates. All independent variables that were associated with the achievement of adequate weight gain in the bivariable logistic regression analysis with a p-value of 0.25 were taken into the multivariable logistic regression. The adjusted odds ratio (AOR) and its 95% CI were used to identify factors associated with adequate weight gain in the multivariable logistic regression. The Hosmer–Lemeshow test was used to assess model fitness, and a p-value greater than 0.05 was considered a good fit. The Kilmogorov-Simirnov test was used to assess the normality of continuous variables and p-value of >0.05 was considered normally distributed.
Results
Demographic characteristics of the study participants
A total of 332 records of children were selected for this study, and 322 of them were included in the final analysis, yielding a 97.0% response rate. The remaining 10 records were found incomplete and were excluded. Almost half of enrolled patients were male. Infants aged 6–11 months constituted the largest age group, accounting for 167 (51.9%), followed by those aged 12–23 months. In total, 211 (65.5%) and 111 (34.5%) children were admitted to Kule and Tierkidi TFU centers, respectively. Three quarters of the children were admitted during the dry season (December to March). A total of 186 (57.8%) patients were referred from nutrition centers to an inpatient treatment (Table 1).
Sociodemographic and anthropometric characteristics of infants and children aged 6–59 months treated for complicated SAM in the TFUs of Tierkedi and Kule Refugee camps.

MUAC = Mid Upper Arm Circumference; WFH z-score = weight-for-height z-score.
Stunting: Stunting, or chronic undernutrition, is a form of undernutrition and presents as low height-for-age (HFA). It is defined by an HFA-z scores below two SDs of the median (WHO standards). Severe stunting is defined by an HFA z-scores below three SDs of the median (WHO standards) Stunting is a result of prolonged or repeated episodes of undernutrition which can start before birth.
Anthropometric characteristics at admission
On admission, the mean and SD of MUAC of patients was 11.50 (0.75) cm. The mean and SD of height or length for admitted children was 70.68 (6.77) cm. Nearly all children (312, 97%) had a non-edematous SAM at admission. Furthermore, 60 (18.1%) of the children admitted to TFUs were severely stunted (Table 1).
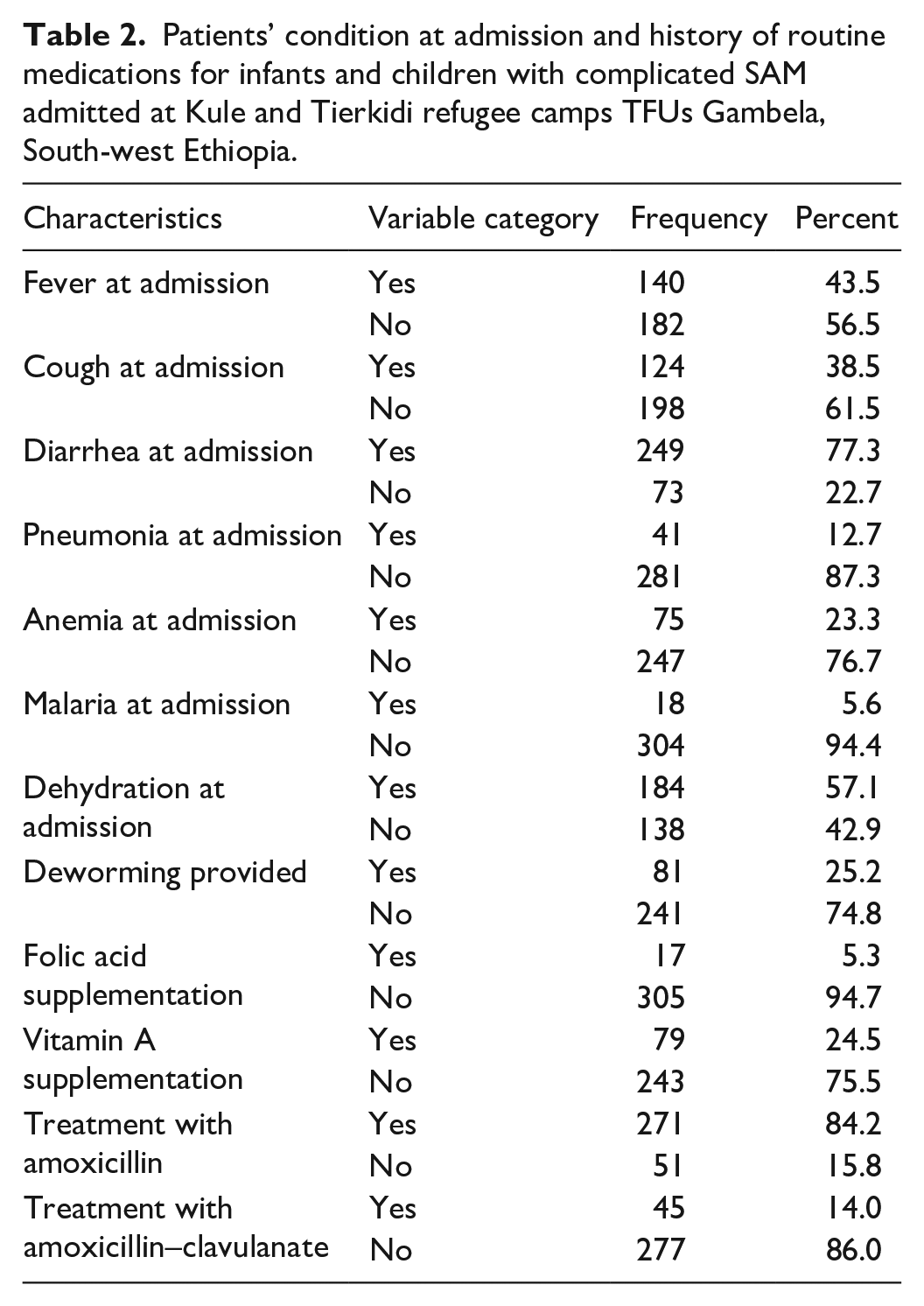
Patients’ condition at admission and history of routine medication
Most of the admitted patients were exclusively breastfed (86%) and vaccinated for their age (60.6%). More than three-quarters of treated patients had diarrhea on admission (77.3%), followed by fever (43.5%) and cough (38.5%). A fifth of patients had anemia, while around 5% of the admitted patients had malaria on admission. Concerning the routine medications provided to the admitted children, a quarter of patients received both vitamin-A supplementation and deworming on admission, while only 5% received folic acid supplementation (Table 2).
Patients’ condition at admission and history of routine medications for infants and children with complicated SAM admitted at Kule and Tierkidi refugee camps TFUs Gambela, South-west Ethiopia.
Achievement of adequate weight gain at therapeutic feeding centers
In total, 232 (72%) of children at the TFUs achieved adequate weight gain (>5 g/kg/day). On discharge, 64% of children admitted to Kule TFU achieved adequate weight gain, while 87.4% of children admitted to Tierkidi TFU achieved adequate weight gain. Three-quarters of children who were admitted with a WFH z-score < −3 achieved adequate weight gain, while only 43.2% of those admitted with a WFH z-score ⩾ −3 achieved adequate weight gain.
The average weight gain (SD) among the study population was 10.70 (6.9 SD) g/kg/day. The average (SD) weight gain for Kule and Tierkidi TFU was 9.47 (6.89) and 13.16 (6.37) g/kg/day respectively. The average length of stay at TFUs was 7.1 days.
Factors associated with achieving adequate weight gain at therapeutic feeding centers
In the bivariable logistic regression analysis, the TFU, referral source, presence of fever at admission, presence of cough at admission, presence of vomiting at admission, treatment with amoxicillin–clavulanate, Vitamin A supplementation status, folic acid supplementation status, WFH z-score on admission, MUAC on admission, and length of stay at the TFUs showed an association with achievement of adequate weight gain (p-value less than 0.25) and hence were taken to the multivariable analysis.
In the multivariable analysis TFUs where the children were admitted for treatment were significantly associated with achievement of adequate weight gain. Children who were treated at Tierkidi TFU were nearly six times more likely to achieve an adequate weight gain than children treated at Kule TFU; AOR = 5.92, 95% CI: (2.08, 16.85). Length of stay at TFU is also found to be significantly associated with achievement of adequate weight gain. Children who stayed at TFUs for less than 7 days were 2.48 times more likely to achieve an adequate weight gain than those who stayed longer; AOR = 2.48, 95% (CI: 1.39, 4.44). In addition, children who received amoxicillin–clavulanate during inpatient treatment were four times more likely to achieve recommended weight gain than those who did not receive such antibiotics for treatment; AOR = 4.13, 95% CI: (1.69, 10.08).
The WFH z-score of the acutely malnourished children at admission was also significantly associated with the achievement of adequate weight gain at TFUs. In this study, children who were admitted with a WFH z-score < −3 were four times more likely to achieve adequate weight gain when compared to those children who were admitted with a WFH z-score > −3; AOR = 4.10, 95% CI: (1.87, 8.97) (Table 3).
Factors associated with achievement of adequate weight gain among infants and children with complicated SAM admitted at Kule and Tierkidi refugee camps TFUs Gambela, South-west Ethiopia.

MUAC = Mid Upper Arm Circumference; TFU = Therapeutic Feeding Unit; WFH z-score = Weight-for-height z-score; COR = Crude Odds Ratio; AOR = Adjusted odds ratio.
Significant association (p-value < 0.05),
Discussion
This study aimed to determine the achievement of adequate weight gain and identify its associated factors among infants and children aged 6–59 months with complicated SAM admitted to TFUs of Kule and Tierkidi refugee camps in Gambela, Ethiopia.
In total, 232 (72%) of children at the TFUs achieved adequate weight gain of >5 g/kg/day. In this study, factors associated with achieving adequate weight gain were the TFU itself, WFH z-score on admission, length of stay at TFUs, and type of antibiotics used for treatment.
The observed level of achievement of weight gain among children with complicated SAM is in line with reports from studies conducted in Ethiopian towns of Aksum, 18 Mekelle, 19 Woldia 20 and Gedeo. 21 Studies in India, 22 Bangladesh 15 , and Democratic Republic of Congo 14 also reported comparable levels of achievement of weight gain among children with complicated SAM. In contrast, higher proportion of treated patients achieved adequate weight gain in this study when compared with other studies conducted in the Dadaab refugee camp of Kenya 23 and Jimma university referral hospital of Ethiopia. 24 The proportion of treated children who achieved adequate weight gain was also higher than the level reported from India.25,26 This difference may be due to the discrepancies in the population, level of facility, health-seeking behavior, availability as well as accessibility of therapeutic foods and medications. Use of different SAM treatment guidelines may have also played a role.
In the current study, patients who were admitted to the TFUs with a WFH z-score < −3 were more likely to achieve an adequate weight gain on discharge. The WFH z-score is found to be inversely related to weight gain. 27 A study done in a nutritional rehabilitation center in India is also in line with this finding as it showed average weight gain to be higher among children with poorer anthropometry (WFH z-score < −3 and MUAC < 11.5 cm) at admission. 28 A study conducted in Niger also supported this finding as it showed the rate of weight gain to be greater among children with WFH z-score < −3 at admission. 29
Treatment with amoxicillin–clavulanate was positively associated with achievement of adequate weight gain among admitted infants and children. This could be due to the resistance of bacterial pathogens to the commonly used antibiotics in the TFUs of developing countries. A study conducted in Niger discovered most enterobacteriacea isolated from children with complicated SAM to be resistant to amoxicillin and cotrimoxazole. 30 A study conducted in Kenya also indicated the existence of widespread resistance to the routinely used antibiotics among patients with SAM and recommended the use of amoxicillin–clavulanate combination to curb the mortality that may come due to resistance to antibiotics. 31 Similarly a systemic review study done on current WHO essential drug for SAM showed there is generally high resistance to first-line antibiotics in a population of mixed, moderate, and severely malnourished children in sub-Saharan Africa and Turkey. 32 However, no published trials or pharmacokinetic studies of amoxicillin–clavulanate in children with SAM have been conducted. 33
Patients who stayed for less than a week at TFUs were more likely to achieve an adequate weight gain than those who stayed longer. This finding is consistent with a study done in Uganda, in which patients achieved significant weight gain during early days of admission and showed a rapid decrease in weight gain after the initial weeks of treatment. 27 This shows that there is an inverse relationship between length of stay and average weight gain. Other studies done in Northern Ethiopia 34 and Dire Dawa 35 also showed similar findings.
In this study, children who were treated in Tierkidi TFU were more likely to achieve adequate weight gain when compared with children who were treated at Kule TFU. This was consistent with other findings where weight gain varied between TFUs, as explained by a study conducted in Dadaab refugee camp in Kenya. 23 In addition, other studies conducted on non-refugee populations in Ethiopia also reported existence of differences between compared TFUs in Debre Birhan, 36 East Amhara, 17 and Mekele. 19 This could be due to differences in the level of care provided in the facilities, staffing, and the condition of patients admitted to the centers. Differences in study settings, case load, and adherence to treatment guidelines may also explain the difference between the treatment centers.
Limitations of the study
Due to the nature of secondary data, important variables such as sociodemographic characteristics of caregivers, and child feeding practices that may influence treatment outcomes were not addressed in this study. The data collection tool was record driven. The absence of a standardized and validated tool is also another limitation.
Conclusions and recommendations
More than 70% of treated children in this study achieved adequate weight gain of >5 g/kg/day. The length of stay of ⩽7 days at TFU, WFH z-score < −3 on admission and treatment with amoxicillin–clavulanate and place of treatment were associated with achievement of adequate weight gain. Based on these findings, we recommend that the local antibiotic sensitivity pattern be studied in order to recommend an appropriate treatment regimen for infants and children. To reduce inconsistencies between treatment centers, standard guidelines must be enforced across the TFU of refugee camps. Close follow-up and supervisor support may help in narrowing the gap in treatment outcomes. Treatment in the TFUs must be given with due care and attention to reduce the unnecessary length of stay that may increase the risk of acquired infections and deteriorate nutritional outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221148602 – Supplemental material for Achievement of adequate weight gain among infants and children with complicated severe acute malnutrition receiving treatment in therapeutic feeding centers of South Sudanese refugee camps in Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221148602 for Achievement of adequate weight gain among infants and children with complicated severe acute malnutrition receiving treatment in therapeutic feeding centers of South Sudanese refugee camps in Ethiopia by Dagim Biratu, Ebissa Negera and Soresa Alemu in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221148602 – Supplemental material for Achievement of adequate weight gain among infants and children with complicated severe acute malnutrition receiving treatment in therapeutic feeding centers of South Sudanese refugee camps in Ethiopia
Supplemental material, sj-docx-2-smo-10.1177_20503121221148602 for Achievement of adequate weight gain among infants and children with complicated severe acute malnutrition receiving treatment in therapeutic feeding centers of South Sudanese refugee camps in Ethiopia by Dagim Biratu, Ebissa Negera and Soresa Alemu in SAGE Open Medicine
Footnotes
Acknowledgements
We thank Mettu University’s college of health sciences for helping in the arrangement of this research work. We also thank data collectors, supervisors, and administrators for their valuable supports.
Authors contributions
DB conceived the research idea and prepared the proposal, handled the data collection process, analyze the data, and draft the article. EN and SZ approved the proposal with some revisions, participated in the write-up process, and reviewed the article. All authors have reviewed and approved the last version of the article.
Availability of data and materials
Data will be available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was conducted according to the principles in the Declaration of Helsinki. Ethical clearance was obtained from the Ethics Review Committee of college of health sciences in Mettu University with reference number: RPG-73-2013. Administrative permission was obtained from the Refugees and Returnees Affairs(RRS) Gambela branch office. Written informed consent was obtained from the heads of both facilities for accessing data of malnourished children for participation in the study which was approved by Ethics Review Committee of Mettu University College of Health Sciences. Confidentiality was maintained while handling the participant’s information.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the heads of both facilities for accessing data of malnourished children for participation in the study which was approved by Ethics Review Committee of college of health sciences. Confidentiality was maintained while handling the participant’s information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.