
Abstract
Introduction:
Wasting among refugee children continues to be a serious public health problem particularly in conflict and in situations when people are displaced. Evidence of risk factors in the refugee context is crucial to successfully prevent malnutrition and its consequences. However, little information is known about the determinants of wasting in a refugee setting. Hence, this study was aimed to identify determinants of wasting among South Sudanese 6- to 59-month-old children in Okugo refugee camp, South-Western Ethiopia.
Methods:
Institutional-based unmatched case–control study was conducted on 99 acute malnutrition children (cases) and 297 children who are not malnourished (control) from 6 April to 2 May 2019. The study participant was selected by systematic random sampling and data on exposure variables were collected by face-to-face interview using a structured questionnaire. Data were entered into Epi data version 3.1 and was exported to SPSS version 25 for further analysis. Descriptive, bivariable, and multivariable analyses were done to compute summary statistics and to identify determinants of wasting.
Result:
The mean age of the cases and controls with standard deviation (SD) was 13.8 (±6.9) and 19.2 (±8.7) months, respectively. Multi-variable analysis revealed that mothers who were unable to read and write (adjusted odds ratio = 3.26, 95% confidence interval (1.07–7.93)), fathers only decision-maker to use donations items in the household (adjusted odds ratio = 3.75, 95% confidence interval (1.28–10.85)), not used all donated refugee food and non-food items (adjusted odds ratio = 2.57; 95% confidence interval (1.17–5.66)), the incidence of diarrhea 2 weeks preceding the survey (adjusted odds ratio = 5.28, 95% confidence interval (2.31–12.04)), and mother’s smoking habit (adjusted odds ratio = 2.98, 95% confidence interval (1.19–7.44)) were significant determinants of wasting.
Conclusion:
The finding shows that mothers who are unable to read and write, father only decision-maker, parents’ smoking habit, not using all donated refugee food items, and diarrheal disease were found to be independent determinants of wasting. Hence, interventions on acute malnutrition which are focused on empowering women through training and strengthening their control over the household assets, proper utilization of donated food, and non-food items will play a paramount role.
Introduction
Wasting among refugee children remains a serious public health issue in conflict and post-conflict recovery conditions due to their increased susceptibility. 1 Globally, acute malnutrition rate in refugee camps is higher than 20% that has been reported. 2 According to 2018 World Health Organization (WHO), the United Nations Fund for Children (UNICEF), and the World Bank report, wasting affects 50.5 million or 7.3% of children under 5 years of age globally. Among these, 33 million have moderate acute malnutrition which affects roughly one in ten under-five children in the least developed countries. Most of these children live in South Asia and Sub-Saharan Africa. 3 Globally, wasting declined from an estimated 58 million in 1990 to 52 million in 2011 by the rate of 11%. 4
WHO 5 defined severe acute malnutrition among children aged 6–59 months whose weight-for-height on Z-score (WHZ) is below −2SD based on WHO multicenter growth reference study group 2006 or clinical signs of bilateral pitting edema, or a very low mid-upper arm circumference (MUAC). The instant reasons for acute malnutrition are lack of food and illness. In most cases, those elements integrate to cause a speedy and substantial weight loss or a failure to gain weight. 6
African region was home to 1.2 billion people, of which 22 million were international migrants, including 6.3 million refugees 7 with more than 80% of refugees being comprised of women and children. Between 2015 and 2017, the number of refugees in the region has increased significantly due to conflict and political instability in the regions. More than half of all refugees’ people were from the Democratic Republic of the Congo, Nigeria, and South Sudan. 8
Ethiopia remains the largest refugee-hosting country in Africa. Today, Ethiopia is home for more than 676,000 refugees mainly from South Sudan, Somalia, and Eritrean. More than 263,000 are from South Sudan. 9 Given the largest refugee-hosting countries in Africa, 9 the government of Ethiopia opens the door to refugees and implemented a new policy allowing refugees to have access to legal documents.10,11
Refugee children aged 6–59 months are more susceptible to malnutrition due to refugee populations are exposed to food deprivation and prolonged periods with a suboptimal diet due to food insecurity that can cause serious illness and death. 12 And also, they suffer from the problem of access to appropriate healthcare, nutrition, and social services. 13 Furthermore, this situation might be fueled by the children’s unintentional separation from their parents and being unaccompanied in the refugee. 14
Evidence from a nutritional survey conducted in 2014 among South Sudanese refugee camps revealed that the extent of acute malnutrition became nearly doubled in comparison to an emergency threshold level of 15%. 15 The risk of malnutrition in refugee children increased with decreasing parent socio-economic status. 16 Factors that are contributing to malnutrition in refugee children vary from country to country.17,18 However, there is no sufficient evidence regarding determinants of wasting among South Sudanese 6- to 59-month-old children in Okugo refugee camp, South-Western Ethiopia. Furthermore, given the heightened vulnerability, evidence on the nutritional status of these refugee children needs great public health attention. Hence, this study was aimed to identify the determinants of wasting among under-five children in Okugo refugee camp, South-Western Ethiopia.
Methods and materials
Study area and period
The study was conducted in Okugo refugee camp of Dimma woreda, Gambella Region, Southwest Ethiopia from 6 April to 2 May 2019. Dimma woreda is bordered between South Sudan on the South, Gureferda woreda on the North, Surma woreda on the East and Gog woreda on the West. It is located about 655 km from the capital city, Addis Ababa, and 456 km away from Gambella town to the southern border. The livelihood of the population is mainly dependent on traditional gold digging and agriculture particularly they used to harvest maize. The refugee camp hosts South Sudanese refugees of whom majority come from Jonglei state fleeing ethnic conflict. The main ethnic groups are Anuak (64%), Murle (32%), and others (4%). The refugees are mainly farmers and pastoralists. The camps have an estimated refugee population of 14,775 with a distribution of 6717 females and 6210 male and 1848 children from South Sudan according to a 2015 report. They live in the village camp constructed by UNICEF. The refugee camp has one health center that provides service for population by professionals in different care units. 19
As it was stated in Ethiopia’s national refugee proclamation in 2004, refugees are entitled with the right to work and reside out of camps, access social and financial services, and register life events, including births and marriages 20 (Figure 1).
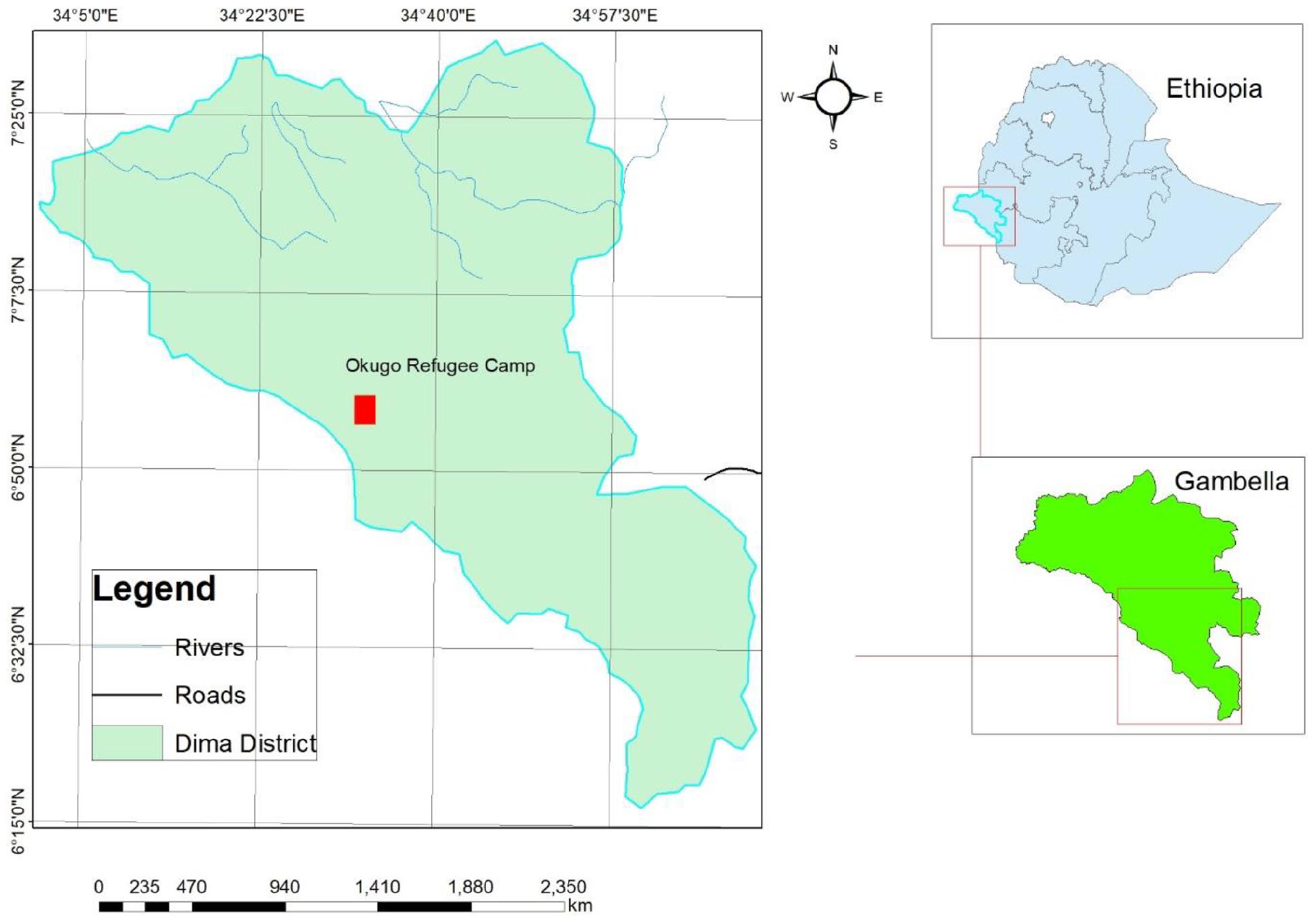
Map of Okugo refugee camp, Gambella Region, Southwest Ethiopia; map produced using Arc GIS version 10.3.
Study design
Institutional-based unmatched case–control study design was conducted.
Source population
The source population was all 6- to 59-month-old children whose parent/caregiver stayed for ⩾6 months in Okugo refugee camp, Dimma woreda.
Study population
For cases
Under-five children aged 6–59 months old whose WHZ is below −2SD based on WHO multicenter growth reference study group 2006 and fulfill inclusion criteria were included as a case. 21
For control
Under-five children aged 6–59 months whose WHZ ⩾−2SD based on WHO multicenter growth reference study group 2006 were included as controls. 21
Inclusion and exclusion criteria
Inclusion criteria
Under-five children who are 6–59 months old whose family/caregiver lived in the refugee camp for ⩾6 months and children whose WHZ is below −2SD based on WHO multicenter growth reference study group 2006 were included as a case.
Under-five children who are 6–59 months old whose families/caregivers lived in the refugee camp for ⩾6 months, and who measured WHZ ⩾−2SD based on WHO multicenter growth reference study group 2006 were included as controls. 21
Exclusion criteria
For both cases and controls, a child with known chronic illnesses like malignant, tuberculosis (TB), human immunodeficiency virus (HIV) infection and acquired immunodeficiency syndrome (AIDS), and congenital abnormality was excluded because these chronic illnesses have an association with malnutrition due to the pathophysiological process or interaction this may cause difficulty of comparison with the healthy control groups.
Sample size calculation
The sample size was calculated using Epi info version 3.3.2 statistical software. The following assumptions were considered: ways of preparing food for child (together with a family/adult) was the exposure variable which is 38.6% among those who are acutely malnourished (cases) and 21.8% among those who are not malnourished children (control) with the odds ratio (OR) of 2.18, 22 95% level of confidence, power of 80%, and 1:3 case–control ratio (we used 1:3 ratio of case to control to increase the power given the expected prevalence of exposure among the controls)

where n1 is the number of cases, n2 is the number of controls, Zα/2is the Z-score for two-tailed test based on α level, Z1 − β is the Z-score for one-tailed test based on β level, r is the ratio of cases to control, p1 is the proportion of exposure among cases, p2 is the proportion of exposure among controls, q1 = 1 − p1, and q2 = 1 − p2.
The sample size became 99 for cases and 270 for controls; overall required sample size was 360. By adding 10% non-response rates, the overall total sample size becomes 396 (case = 99 and control = 297).
Sampling technique
Initially, for anthropometric measurements, WHZ was done for all 6–59 months children who stayed for at least ⩾6 months in the refugee camp to select acutely malnourished children for cases and control. Furthermore, a unique consecutive number was re-assigned to create a sampling frame for identified eligible children with mother/caregiver. Systematic random sampling (SRS) techniques were used to select the study participants using sampling interval (K) calculated from total eligible children with mother/caregiver and total sample size.
After selecting the cases, constantly three controls were selected from the right and left neighbors of each case. If control was not found in the right and left of immediate neighbors, the next child with mother/caregiver were included.
In case more than one under-five acutely malnourished children are found in a family, the youngest child was included in the study because of different evidence-based studies indicate that being young age has a significant association with acute malnutrition.15,23,24 When a case was not found, non-duplicative consecutive children with mother/caregiver were selected to find the case.
Study variables
Under-five children aged 6–59 months old who measured WHZ below −2SD based on WHO 21 multicenter growth reference study group 2006 were considered as the dependent variable.
Socio-demographic variables of the parents (parents educational status, parents occupational status, head of household, family size, presence of livestock, income, ethnicity, religion), parent behavioral factors (parent smoking habit, parent’s practice of using all donated refuge food and other item, maternal autonomy in decision-making), child-related characteristics (sex, age, birth order of the index child, birth interval of the index child, immunization of the index child, and morbidity status of the index child), child caring practices(feeding practice such as exclusive breastfeeding, complementary feeding, and duration of breastfeeding, healthcare seeking and hygiene, child food preparation), maternal/obstetrics-related factors (maternal age at first birth, family planning status of the mother, antenatal care (ANC) attendance of at least one times, health status of mother during pregnancy, food supplementation during pregnancy, parity, and age of mother at index childbirth) were independent variables.
Data collection methods
Anthropometry of the children was measured based on the WHO 25 standardized procedures. For children aged less than 24 months, their length was measured in a recumbent position, while standing height was measured for those who are 24 months and older. For children less than 2 years old, unclothed or slightly dressed children were weighed to the nearest 10 g using 25 kg portable Salter spring scales. Beam balance was used to measure weight of greater than 2 years old children read to the nearest 0.1 kg. Standing height was measured to the nearest 0.1 cm for greater than 2 years and the recumbent length was measured nearest 1 mm for less than 2 years children using UNICEF’s recommended model wooden board, as per the WHO protocol.26,27 The structured interviewer administered questionnaires were adapted from Ethiopian demographic health survey 28 and a thorough review of different literatures. The adapted questionnaire was translated to Agnuwaha language for the sake of better understanding of the interview, and back translated into English by different experts to see the consistency. Pretest was conducted in 5% of the samples in Bandera town which is a local community camp to see the completeness, consistency, applicability of the instruments and ratify accordingly. Besides basic information on child characteristics, caring practices, socio-demographic characteristics, environmental conditions, obstetric-related factors, and parent behavior-related factors was collected from the immediate caregivers of the children by face-to-face interview using a pretested structured questionnaire. The data were collected by six data collectors (clinical and midwifery nurses) and supervised by two bachelors of sciences (BSc) in public health officer. The principal investigator made overall supervision daily.
Data quality assurance
Well-designed data collection instruments, properly coding, filling, and cleaning of missed data guaranteed quality of the data. Both the interviewers and supervisors were trained for 2 days on the objective, methodology of the research, data collection methods, interviewing approaches, anthropometric measurements, and data recording process. Moreover, the data collectors were blind for cases and controls to minimize the interviewer bias.
The data collector and supervisor were calibrated the scale ahead of measurement of children and validation was done by comparing scale reading with a known weight of 3 kg object. For the sake of standardization, anthropometric measurements of children were done two times by trained professionals using standard procedure of WHO during the daytime to minimize the measurement error. An anthropometric measurement was taken twice and a difference of 100 g in weight and 0.1 cm in length were accepted as normal. 29
Data processing and analysis
Epidata version 3.1 was used for data entry, and then the data were exported to SPSS version 25 for further analysis. Before analysis, data were cleaned, edited using simple frequencies and cross-tabulation; re-categorization of categorical variables and categorization of continuous variables were done accordingly to be suitable for analysis.
The descriptive statistics of numerical variables were expressed by mean value and standard deviation while categorical variables were presented in percentage (%) and frequency using table bar graph. The normality of continuous variables data was cheeked by histogram. The anthropometrics data were also analyzed by WHO Anthro software in order to identify the cases and controls.
Initially, bivariable analysis was performed between a dependent variable and each of the independent variables, one at a time. Their ORs at 95% confidence intervals (CIs) and p-values were obtained. Then, all variables found to be significant at bivariable level (p-value ⩽ 0.25) became fitted into a multivariable logistic regression model. The following variables educational status of mother, maternal control/decision-making, parental assault in the past 1 month, using all refugee donated food and non-food items/ration, mother smoking status, father smoking status, feeding practice of child during illness, still breastfeeding status, diarrhea in the past 2 weeks before survey, immunization dose received with appropriate age, morbidity status of upper respiratory tract infection (URTI)/cough in the past 2 weeks, health seeking status of mothers, and extra food consumption during pregnancy were a candidate for multivariable analysis. Then, multivariable logistic regression was applied by stepwise regression eliminations methods and adjusted odds ratios (AORs) together with their corresponding 95% CIs and a p-value < 0.05 were used as a difference of statistical significance. Model goodness-of-fit was tested by the Hosmer–Lemeshow model goodness-of-fit test. 30 The final model fitness test result was (χ2 = 9.76, p-value = 0.282).
Operational definitions
Acute malnutrition: anthropometric measurement of WHZ below −2SD based on WHO 21 multicenter growth reference study group 2006.
Cases: under-five children age 6–59 months old who measured, WHZ below −2SD based on WHO 21 multicenter growth reference study group 2006.
Control: under-five children age 6–59 months who are measured WHZ ⩾−2SD based on WHO 21 multicenter growth reference study group 2006.
Healthcare seeking behavior: healthcare seeking behavior of the caregiver of the child within 24 h of the onset of symptoms. 31
Immunization status: it is defined as on-time full vaccination in which all vaccine doses are administered within 4 days prior and within 4 weeks after the recommended age specified in the national immunization schedule. 32
Autonomy of mother in decision-making: independent decision-making on earned donations from the camp or money in the household. 33
Complementary foods: they are foods that are required by the child, after 6 months of age, in addition to sustained breastfeeding. 34 In this study, we categorized frequency of complementary feeding as =<two or >two per a day.
Ethical consideration
Ethical clearance was obtained from the ethical review committee of Wollega University, Institute of Health Science (reference no. IHSH/122/2011). Official permission was secured from the District Health Office and Administration Office of Refugee-Returnee Affairs (ARRA). The study subjects were informed about the objective of the study, and written assent was obtained from parents/caregivers. Confidentiality of the data was guaranteed and collected secretly. Feedback and advice were given to the respondents during data collection time as needed.
Result
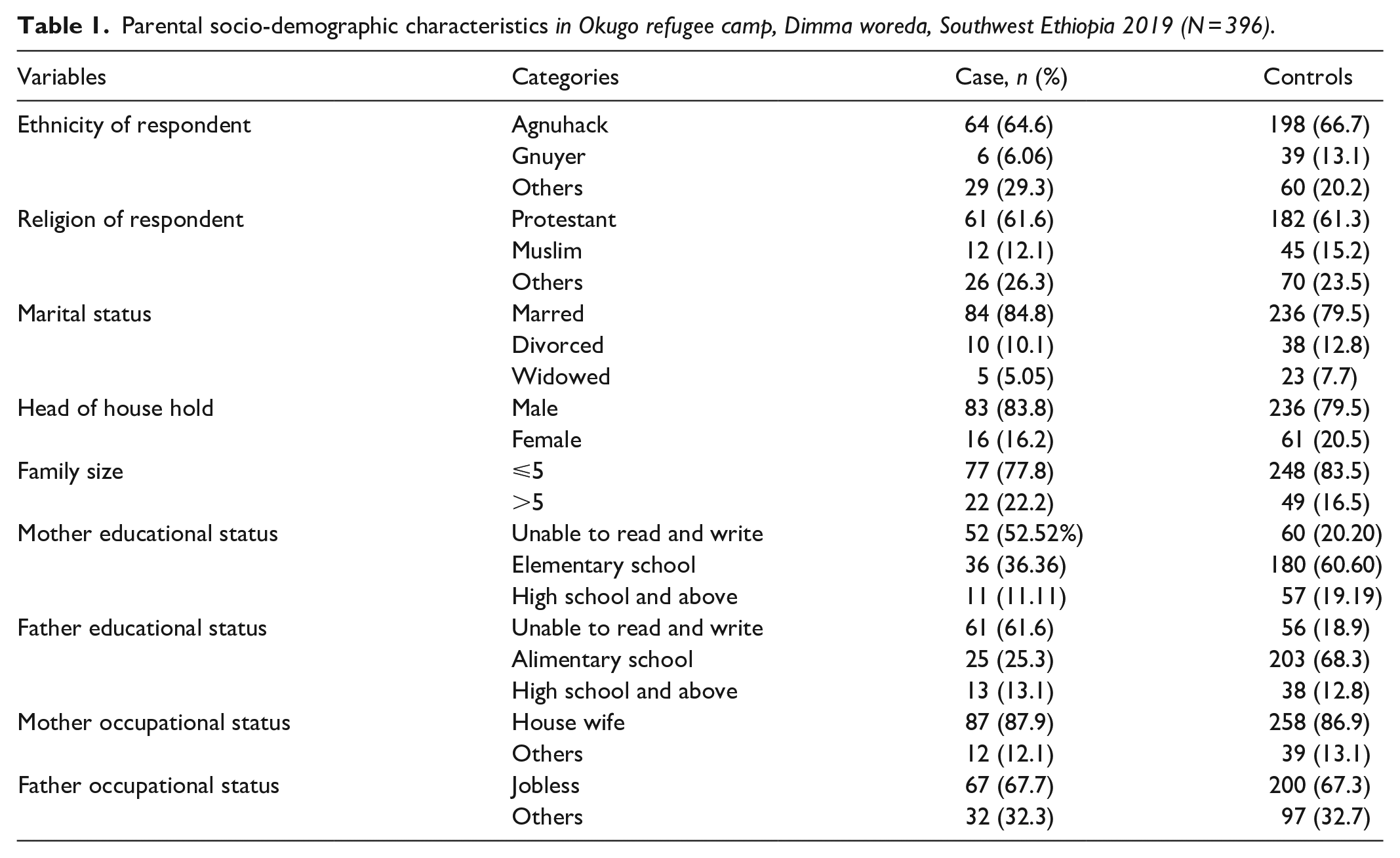
A total of 99 cases and 297 controls were included in the study. The mean age of the respondents was 25.6 ± 4.9 SD years among case and 25.2 ± 5.3 years among control. Female head of the household accounts for 16 (6.2%) among cases and 61 (20.5%) among the control group of the respondent. The majority of mothers were Agnuhack (66.2%) and Gnuyer (11.4%). Regarding the educational status of mothers, 52 (52.5%) cases and 60 (20.2%) controls were illiterate/unable to read and write, and also among the cases 13 (13.1%) and 38 (12.8%) attended high school and above. Out of total mothers surveyed, 87 (87.9%) of mothers of cases and 258 (86.9%) of controls were housewife, and 67 (67.7%) cases and 200 (67.3%) controls were jobless (Table 1).
Parental socio-demographic characteristics in Okugo refugee camp, Dimma woreda, Southwest Ethiopia 2019 (N = 396).
Child characteristics-related factors
Regarding the sex of under-five children, 67 (67.7%) of the cases and 171 (57.6%) control were males. The mean age of the cases and controls was 13.85 ± 6.9 and 19.2 ± 8.7 months, respectively. Nearly three-fifths of wasting were in the age interval between 6 and 11 months. The majority of both cases and controls were born in a narrow birth interval of <24 months. Majority 78 (78.8%) of the case group and about one-third 89 (30%) of the control group had diarrhea before 2 weeks of data collection (Table 2).
Child-related characteristics in Okugo refugee camp, Dimma woreda, Southwest Ethiopia, 2019 (N = 396).

Child care-related factors
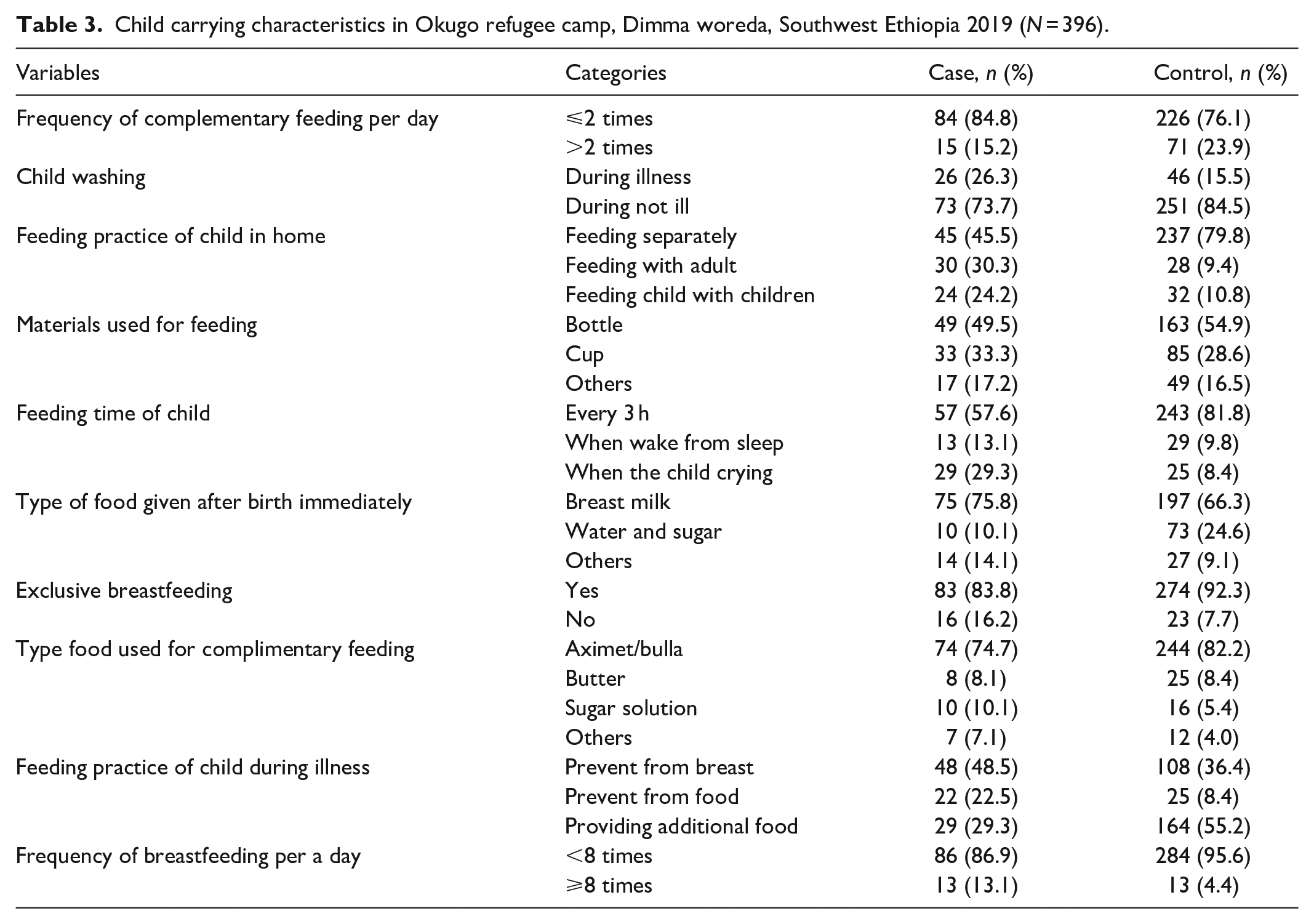
Concerning the child caring practice, the majority 83 (83.8%) of mothers of cases and 274 (92.3%) of mothers of controls were still breastfed their child. Among the breastfeeding mothers, 86 (86.9%) cases and 284 (95.6%) from control group feed their child less than eight times per a day. Besides to this, 97 (98%) cases and 281 (94.6%) control started complementary feeding in <6 months and also 15 (15.2%) among cases and 71 (23.9%) among control mothers/caregivers were feeding complimentary food greater than two times per a day, respectively.
Among the respondents, 52 (52.5%) cases and 237 (79.8%) control group fed their children separately during complementary feeding. The majority of the cases 73 (75.5%) and control group 246 (83.7%) feed aximet/bulla for complementary feeding. About three-fifths of respondents from the case and control group bath their child during illness (Table 3).
Child carrying characteristics in Okugo refugee camp, Dimma woreda, Southwest Ethiopia 2019 (N = 396).
Maternal characteristics-related factors
Regarding maternal/obstetrics-related factors, the mean age at the first birth of study participants was 20.9 ± 3.5 SD years among case and 20.8 ± 3.3 years among control. And also, the mean age at the index pregnancy was 23.4 ± 4.4 SD years among case and 22.8 ± 4.9 years among control.
Concerning ANC utilization by respondents, 42 (42.4%) of cases and 241 (81.1%) of controls had at least one ANC follow-up. Overall, 51.5 (51.5%) among cases and 257 (86.5%) among the control group consumed supplementary food during pregnancy. In addition to this, the majority of the respondents among the cases 92 (92.9%) and the controls 279 (93.9%) had parity of less than five (Table 4).
Maternal/obstetrics-related factors in Okugo refugee camp, Dimma woreda, Southwest Ethiopia 2019 (N = 396).

ANC: antenatal care.
Parental habit-related factors
Out of total respondents, 22 (22.2%) of mothers of cases and 148 (49.8%) of controls were practicing involvement in decision-making. Regarding the ration using status of respondents, 53 (53.3%) cases and 248 (83.5%) controls were using all donated refuge food and others items. A significant number of case groups 21 (45.7%) and control groups 28 (57.1%) were selling donated refugee items to buy non-food items. In addition to this, 66 (66.7%) mothers of cases and 60 (20.2%) of mothers of control group were smoking and among these 60 (90.9%) cases and 36 (60%) of controls were using traditional smoking materials. Regarding the source of money for smoking, majority of cases 45 (68.2%) and controls 38 (63.3%) were selling the refugee-donated items.
Regarding father smoking habit, 63 (63.6%) the cases and 50 (16.8%) the control practice smoking; among this, 55 (85.5%) the cases and 28 (60%) the controls were used traditional smoking substance. About 37.5% of the cases and 7 (31.8%) controls were smoking greater than three sticks of cigarettes per day. Among the cases, 22 (22.2%) and controls 29 (9.8%) were chewing khat in the last 6 months. About 46 (73%) cases and 34 (68%) controls were selling refugee food and non-food items (Table 5).
Parent habit-related factors in Okugo refugee camp, Dimma woreda, Southwest Ethiopia 2019 (N = 396).

Determinants of severe acute malnutrition
Maternal educational level was a significant determinant for wasting in which the odds of wasting are three times high unable to read and write than those children whose mother is literate/high school and above (AOR = 3.26, 95% CI = 1.07–7.93). Likewise, the odds of wasting were nearly four times higher among children whose fathers were the only decision-maker to use donations in the household compared with those children whose families have made decisions jointly on the issue (AOR = 3.75, 95% CI = 1.28–10.85). Similarly, not using all donated refugee food and non-food items was a significant determinant for wasting. The odd of wasting was 2.57 times among the children whose family not use all donated refugee food and non-food items compared to that of their counterparts (AOR = 2.57; 95% CI = 1.17–5.66). However, current marital status and father level of education were not statistically significant in the multivariable analysis of this study.
Furthermore, the incidence of diarrheal disease in the last 2 weeks preceding the survey was seen as one of the determinants of wasting. The odds of wasting were 5.28 times high in children who had diarrhea before 2 weeks than those children who had not diarrhea within 2 weeks preceding the survey (AOR = 5.28, 95% CI = 2.31–12.04). However, the morbidity status of the child by URTI in the last 2 weeks preceding the survey was not seen significantly associated with severe wasting in 6- to 59-month-old children in a multivariable analysis of this study. Likewise, the odd of wasting was nearly three times higher among children from parents who had smoking habit compared with those children whose parents have no smoking habit. In this study, the odds of wasting were seven times higher among children from families whose mothers were not taken the child to health institution within 24 h of the onset of symptoms of illness compared with those children’s whose mothers were taken within 24 h of the onset of the symptoms of illness (AOR = 6.58, 95% CI = 2.75–15.76) (Table 6).
Determinants of wasting among South Sudanese 6- to 59-month-old children in Okugo refugee camp, Dimma woreda, Southwest Ethiopia 2019 (N = 396).

COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
p-value ⩽ 0.05; **p-value ⩽ 0.001.
Discussion
This case–control study was conducted to identify determinants of wasting among children aged 6–59 months in Okugo refugee camp. In this study, wasting among the refugee children aged 6- to 59-month-old was significantly associated with husband only decision-making to use the donation in the households, incidence of diarrhea before 2 weeks of the survey, mother smoking habit, not using all donated food and non-food items in the household, father smoking habit, health seeking behavior of the mother after the onset of symptom, and maternal educational level.
Among socio-demographic factors, maternal illiteracy was found to be a significant determinant for wasting in which children whose mother is unable to read and write were more likely to be wasted than those children whose mother attended high school and above. This finding is consistent with different studies done in Kampala Uganda, Burkina Faso, Malawi, Tanzania, and Zimbabwe.35–37 The possible explanation is that malnutrition is directly and indirectly related to maternal education because having low educational status decreases the passion of self and child care as well as the ability to give a decision on household. 38 Furthermore, mothers with a lower level of education are less likely to seek healthcare as compared to their counterparts. This decreases healthcare seeking behavior for manageable diseases such as diarrhea in which it can lead to severe wasting. 39
However, in this study, paternal education is not significantly associated with acute malnutrition of the children, which is not consistent with a study conducted in the Al-Quds University in Gaza strip Jabalia Refugee camp. 40 The potential explanation might be the difference in culture, study designs, and tradition of the study area in which the fathers’ considerer caring of the children as the responsibility of the mothers.
In this study, there is a significant difference between children who have no exclusive breastfeeding and those children who have exclusive breastfeeding. The odd of wasting is 5.28 high among those children who have no exclusive breastfeeding. This is supported by other studies conducted in Nepal and Mai-Aini Eritrean refugee camps.17,24 This might be due to increased good awareness in breastfeeding currently in a camp set up. Exclusive breastfeeding is recommended because breast milk is containing necessary nutrients in the first few months of life. Besides, the mother’s antibodies in breast milk offer the infant immunity to disease. 41
Decision-making power on the utilization of donated food and non-food items is found to be significantly associated with severe acute malnutrition. The odd of wasting is about three times high among decisions made by fathers only on the use of donations provided by the organization. This finding is similar with the study done in Rohingya refugees in Bangladesh 42 in which the odd of wasting is lower by more than one-third among children whose mothers participated in making all household decisions. Similarly, the pocket study done in Ethiopia also supports this finding in which children whose mothers had no power to decide how income earned are more likely to be wasted than their counterparts. 43 This might be due to the direct or indirect effect of joint decision-making on household food security, women’s empowerment, and socio-economic status which can positively or negatively affects the nutritional status of children. Currently, the government policy also encourages empowering women through women education and increasing the influence of women in all spheres of life which has a significant impact on the health of the family and the community. 22
In this study, not using all donated refugee food and non-food items in the household was one of the independent predictors of wasting. The odds of wasting were more likely to occur among the children whose family not use all donated refugee food and non-food items compared to that of the counterpart. In this refugee set-up, all households do not have any source of income and they are heavily dependent on continuous international food aids, and other forms of assistance. Most households of cases and controls exchange donations provided for them to by complementary food items and non-food items. However, only fathers who made decision to exchange the donations might satisfy their individual needs which lead to food shortage in the household making children are more vulnerable.
A study conducted in Mai-Aini Eritrean refugee camp, Northern Ethiopia showed that children whose mothers did not consume extra food during pregnancy are associated with acute malnutrition of the children. 17 Nevertheless, there is no significant difference in children whose mothers not consumed extra food during pregnancy and those having consumed extra food during pregnancy in relation to acute malnutrition in this study. This inconsistency might be due to the availability of ANC service being provided in the primary healthcare units and increasing the access of the service and due to the nature of study population and study design difference.
Moreover, this study described the diarrheal disease in the last 2 weeks preceding the survey were also seen as one of the determinants of wasting in 6–59 children. Wasting was more likely to occur in children who had diarrhea before 2 weeks than those children who had not diarrhea within 2 weeks preceding the survey. This finding is consistent with the study done in South Sudan, Eritrean, and Uganda.17,23,44 The possible explanation might be due to loss of fluids and electrolytes, loss of appetite, and decrease in absorption of food in the intestine due to high motility of the intestine during diarrhea episodes.45,46
However, this study does not show a significant association between the morbidity status of the child with URTI and acute malnutrition. This is inconsistent with similar studies conducted in India. 23 This might be due to the high coverage of immunization and Vitamin A supplementation in the camp, and the difference in study design.
In this study, it was indicated that children who have been not taken to health institutions within 24 h of the onset of symptoms were more likely to be wasted than those who were taken within 24 h of the onset of the symptoms. This finding is consistent with the study done in South Sudan. 22 This finding supports that taking sick children within 24 h of the onset of the symptoms is advisable to prevent further disease progression and early detection of the problem.
Likewise, the odds of wasting were three times higher among children whose parents had smoking habits compared with those children whose parents have no smoking habit. The possible explanation might be due to exposure to cigarette smoke or being a passive smoker at the age of 6–59 months may itself affect child growth and weight gain and also smoking substances can alter the behavior of mother toward the child and self-care. 47 Furthermore, the counter effect of expenditure on smoking in poor households like refugee families can impede the child’s nutrition status.48,49
Limitation of the study
Having considered only weight/height as an anthropometric indicator of acute malnutrition also may have left out cases identified by MUAC. Furthermore, these anthropometric indicators identify different groups of children with different manifestations of acute malnutrition and different risk of death in which MUAC is better than WHZ to identify high-risk children in the community. 50 Since this study assesses the history of exposure retrospectively, it may be prone to recall bias. However, due attention was given to the study procedures, including the process of training, the research team, standardization of anthropometric measurements, and a close supervision throughout the field activities to minimize the expected bias. Since the refugees were displaced from their homeland inconveniently, some of them did not bring their birth certificates or immunization card, especially those children born outside of Ethiopia.
Conclusion and recommendation
According to the finding of this study, maternal education, not exclusively breastfeeding, diarrhea disease 2 weeks preceding the survey, not taking sick children timely to a health facility for treatment, not using all donated food and non-food items, husband only decision-making in household, and parental smoking habit are found to be independent predictors of acute malnutrition.
Recommendation
There is no engine that can immediately alleviate acute malnutrition in children rather it needs coordinated activity and inter-sectoral collaboration. Hence, ARRA is recommended to work with concerned non-governmental organizations (NGOs) which are working in Okugo refugee camp in combating acute malnutrition by giving education on health seeking practice of parents after the onset of symptom and proper utilization of donated food and non-food items. It is also necessary to work on women empowerment/decision-making through training and strengthening their control over the household assets and ability on the usage of donations provided for the households. Besides to this prevention and control of childhood diarrheal illness through improving access to safe and adequate water supply, sanitation and hygiene practices will play a paramount role. Therefore, health extension workers who are in the refugee community need to focus on educating the community to maintain hygiene and sanitation for themselves and their children.
Footnotes
Author contributions
T.T. conceived the study, developed the tool, coordinated the data collection activity, and carried out the statistical analysis, and interpretations of the results and manuscript write-up. D.W., H.B., and E.T. participated in developing the tools, data analysis, and involved in report write-up. E.T. made substantial contribution in result writing and reviewing manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The research questionnarie(s) used in this study was made available. Raw data will be available upon request from the corresponding authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the ethical review committee of Wollega University, Institute of Health Science (reverence no. IHSH/122/2011), and official permission was secured from the District Health Office and Administration Office of Refugee-Returnee Affairs (ARRA). Ethical clearance was obtained from the ethical review committee of Wollega University, Institute of Health Science.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.