
Abstract
Objective:
There is an increasing recognition of the burden of cardiovascular disease in Africa. However, little is known about the pooled prevalence of acute coronary syndrome (ACS)-associated in-hospital mortality and contributing factors.
Methods:
PubMed, Medline, Embase, Web of Science (Core Collection), and supplementary sources including Google Scholar, World Cat, Research Gate, and Cochrane Library were searched. Chi-square test and I2-statistic were used to assess heterogeneity. Egger’s and Begg’s tests and funnel plots were used to assess publication bias. Data were analyzed using Stata software (version 15.0).
Result:
Twenty nine studies with a total sample of 11,788 were included. The pooled estimate of all-cause in-hospital mortality was 22% (pooled proportion (PP) = 0.22; 95% confidence interval (CI): 0.17–0.27. The In-hospital mortality rate was lower at the cardiac centers (PP = 0.14; CI: 0.05–0.23) compared to referral hospitals (PP = 0.24; CI: 0.17–0.31]) The mortality rate was comparable in Eastern (PP = 0.23; CI: 0.19–0.27) and Northern Africa (PP = 0.22; CI: 0.16–0.28). The incidence of in-hospital heart failure, cardiogenic shock, arrhythmia, bleeding, acute stroke, and reinfarction were 42, 17.0, 20.0, 16.0, 4.0, and 5.0%, respectively.
Conclusion:
All-cause in-hospital mortality rate associated with ACS is high in Africa. The mortality rate at cardiac centers was 10% lower when compared with referral hospitals. Establishing coronary units, strengthening existing cardiac services, and improving availability and access to cardiovascular medicines could help in reducing the burden of ACS in the continent.
Keywords
Introduction
Ischemic heart disease (IHD) is the leading cause of morbidity and mortality worldwide with 126.5 million affected people in 2017. 1 Forecasts of prevalence based on predictive models indicated that by 2030, the prevalence of IHD could increase to more than 1845 per 100,000. 2 Acute coronary syndrome (ACS), comprising ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), and unstable angina (UA), continues to be the most common cause of cardiovascular death in developed countries. 3 Although ACS-related mortality has gradually declined over the last decades in developed countries, the trend is completely different for developing countries. 4
ACS incidence and mortality in Africa have shown a significant increase due to a sharp rise in cardiovascular risk factors such as diabetes, dyslipidemia, uncontrolled hypertension, 5 expansion of the aging population, and change in lifestyle. Additionally, limited resources including the lack of emergency cardiac services, healthcare infrastructure, availability of cardiovascular medicines, and inadequate staffing further contribute to the increase in in-hospital mortality from ACS. 6 This is particularly the case for patients living in rural areas where there is limited access to medical expertise and diagnostic testing centers, coupled with challenges of transportation, holding back patients from seeking early medical care and timely treatment. 7
Mortality data play a vital role in framing healthcare plans and policies to prevent or reduce premature deaths and improve patients’ quality of life. 8 In Africa, ACS-related in-hospital mortality considerably varies from country to country. However, these data have not been comprehensively evaluated to provide a pooled estimate of the incidence of in-hospital mortality among patients with ACS in the continent. Therefore, this review aimed to examine the in-hospital mortality from ACS in Africa and identify factors contributing to mortality. This would generate new data on the magnitude of the problem in the continent that could inform policymakers regarding strategies to reduce the burden of ACS. Additionally, such data have the potential to provide insights into the quality of emergency care provided for patients with ACS in the continent.
Methods
Study protocol and reporting
The protocol for this systematic review was registered and available in Prospero (R.NO CRD42020165789). The study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.
Literature search strategy
We searched PubMed/Medline, EMBASE, Web of Science (Core Collection), and supplementary sources including Google Scholar, World Cat, Research Gate, and Cochrane Library for published studies that evaluated the in-hospital mortality and or nonfatal major adverse cardiovascular events (MACE) from ACS. The search terms were related to “ischemic heart disease” and “mortality.” IHD-related terms were: myocardial infarction, MI; Acute Coronary Syndrome, ACS; ST-Segment Elevation Myocardial Infarction, STEMI; Non-ST-Segment Elevation Myocardial Infarction, NSTEMI; Unstable Angina, UA; coronary thrombosis and Ischemic Chest Pain. Mortality-related terms were: death, collapse, and terms related to nonfatal MACEs such as in-hospital heart failure, in-hospital acute stroke, bleeding, arrhythmia, reinfarction, and cardiogenic shock. In addition, we manually examined the reference list of included studies to identify any additional eligible studies. The search was performed for studies conducted between 2005 and 2018 and was limited to the English language.
Eligibility criteria
Inclusion criteria
Studies that reported in-hospital death and/or MACE among patients hospitalized with ACS of any disease duration, and medical co-morbidities and conducted in any healthcare settings in Africa, and published in the English language were eligible for inclusion.
Exclusion criteria
Review articles, case reports, conference abstracts, qualitative studies, letters, and eight articles without raw data available/accessible for retrieval were excluded.
Study selection and screening
Retrieved studies were considered eligible after title and abstract screening and passed into full-text review by two reviewers (FA and SA) and disagreement was resolved in discussion with a third reviewer (MAM) when existed. A detailed PRISMA flowchart outlining the screening process is presented in Figure 1.

PRISMA diagram depicting screening of articles for systematic review and meta-analysis on in-hospital outcomes of the acute coronary syndrome in Africa.
Data extraction and quality assessment
The Joanna Brigg’s Institute critical appraisal checklist was used to assess the quality of included studies. 9 The quality assessment was conducted independently by two reviewers (FAM and SA) and studies were categorized as low (0–4), moderate (5–6), and high (7–9) quality. The two reviewers (FA and SA) independently extracted relevant information into the data extraction format. Relevant data such as author and year of publication, the country and region of the study, the setting, types of ACS, sample size, number of in-hospital death, and MACE (in-hospital heart failure, in-hospital acute stroke, cardiogenic shock, reinfarction, bleeding, and Arrhythmia) were extracted.
Outcome variables
The pooled incidence of in-hospital mortality from any cause was the primary outcome and the pooled incidence of MACE was the secondary outcome.
Statistical analysis
The pooled incidence of primary and secondary outcomes was computed using Stata software, version 15.0 (Stata Corp. 2015. Stata Statistical Software, Release 15, College Station, TX, USA) by using random effect (Der Simonian and Laird) models and reported as a proportion. Heterogeneity was assessed using I2-statistics based on the Cochrane handbook for systematic review and meta-analysis and classified as: 0–40%—might not be important, 30–60%—moderate heterogeneity; 50–90%—substantial heterogeneity; and 75–100%—considerable heterogeneity. 10 Begg’s and egger’s test and funnel plot symmetry were used to assess publication bias. Subgroup analysis was conducted by regions of the continent (Eastern Africa, Western Africa, Northern Africa, and Southern Africa), types of the healthcare facility (General hospitals, Referral hospitals, and Cardiac centers), and the phenotypes of ACS (STEMI, NSTEMI, and UA) to explore possible causes of heterogeneity in the included studies. Besides, sensitivity analysis was performed to see the influence of specific studies on the occurrence of outcomes of interest. This helped to identify a specific study with results that conflicts with the rest of the studies, and thus, explore the possible source of heterogeneity. A p-value of ⩽0.05 was considered significant in all cases.
Definition of terms
ACS: ACS is a spectrum of conditions of acute myocardial ischemia or infarction caused by an abrupt reduction in coronary blood flow. 11 It can be divided into ST-segment elevation ACS (STEMI) and non-ST-segment elevation ACS (NSTEMI/UA).
STEMI: Characteristic symptoms of myocardial ischemia in association with persistent ST-segment elevation on electrocardiogram (ECG) with positive troponins.
NSTEMI: characteristic symptoms of myocardial ischemia in association with ST-segment depression, T-wave inversion, or transient or nonspecific ECG changes with positive biomarkers.
UA: Characteristic symptoms of myocardial ischemia in association with ST-segment depression, T-wave inversion, or transient or nonspecific ECG changes and no positive biomarkers for cardiac necrosis.
Nonfatal MACE: The composite endpoint of in-hospital acute stroke, re-infraction, cardiogenic shock, in-hospital heart failure, major bleeding, and arrhythmia in patients hospitalized with ACS.
Fatal MACE: In-hospital death as confirmed by a physician.
Results
A total of 1499 studies were retrieved from an electronic database search. After 187 duplicates were removed, 1312 studies were screened by titles and abstracts. After excluding 1200 studies, the full text of 112 studies were reviewed. From these, 83 studies were further excluded based on the eligibility criteria, and 29 studies (24 cross-sectional studies, 3 prospective and retrospective cohort studies, and 2 prospective surveys) with a total sample of 11,788 (7151 STEMI, 3147 NSTEMI, and 1490 UA) were included in the final analysis (Figure 1).
Characteristics of included studies
Among the total studies included, 8 were conducted in eastern Africa,12–18,19 4 in West Africa,20,21,22–24 15 in northern Africa,25–38,39, and 1 in Southern Africa. 40 Twenty-four studies were conducted in referral hospitals,12–18,19,22–24,26,27,29–33,35–40 two in general hospitals,22,23 and five in cardiac centers20,21,25,28,34 (Table 1).
Characteristics of the included studies.

STEMI: ST-segment elevation myocardial infarction; NSTEMI: non-ST-segment elevation myocardial infarction; UA: unstable angina; NA: not applicable.
The incidence of in-hospital outcomes
The estimated pooled incidence of in-hospital death rate was 22% (pooled proportion (PP) = 0.22; 95% confidence interval (CI): 0.17–0.27; I2 = 97.1; p = 0.000) (Figure 2). In addition, we estimated the magnitude of MACE and thus, the incidence of in-hospital heart failure, cardiogenic shock, and arrhythmia were 42% (PP = 0.42; 95% CI: 0.30–0.54; I2 = 98.8; p = 0.000) (Figure 3), 17% (PP = 0.17; 95% CI: 0.12–0.22; I2 = 91.4; p = 0.000) (Figure 4), and 20% (PP = 0.20; 95% CI: 0.15–0.24; I2 = 94.3%; p = 0.000) (Figure 5), respectively. The incidence of reinfarction, in-hospital acute stroke, and bleeding were 5% (PP = 0.05; 95% CI: 0.03–0.07; I2 = 58.0; p = 0.020) (Figure 6), 4% (PP = 0.04; 95% CI: 0.02–0.05; I2 = 76.1; p = 0.000) (Figure 7), and 16% (PP = 0.16; 95% CI: 0.06–0.26; I2 = 99.2; p = 0.000) (Figure 8), respectively.

The incidence of in-hospital death among patients with acute coronary syndrome in Africa.

The incidence of in-hospital heart failure among patients with acute coronary syndrome in Africa.
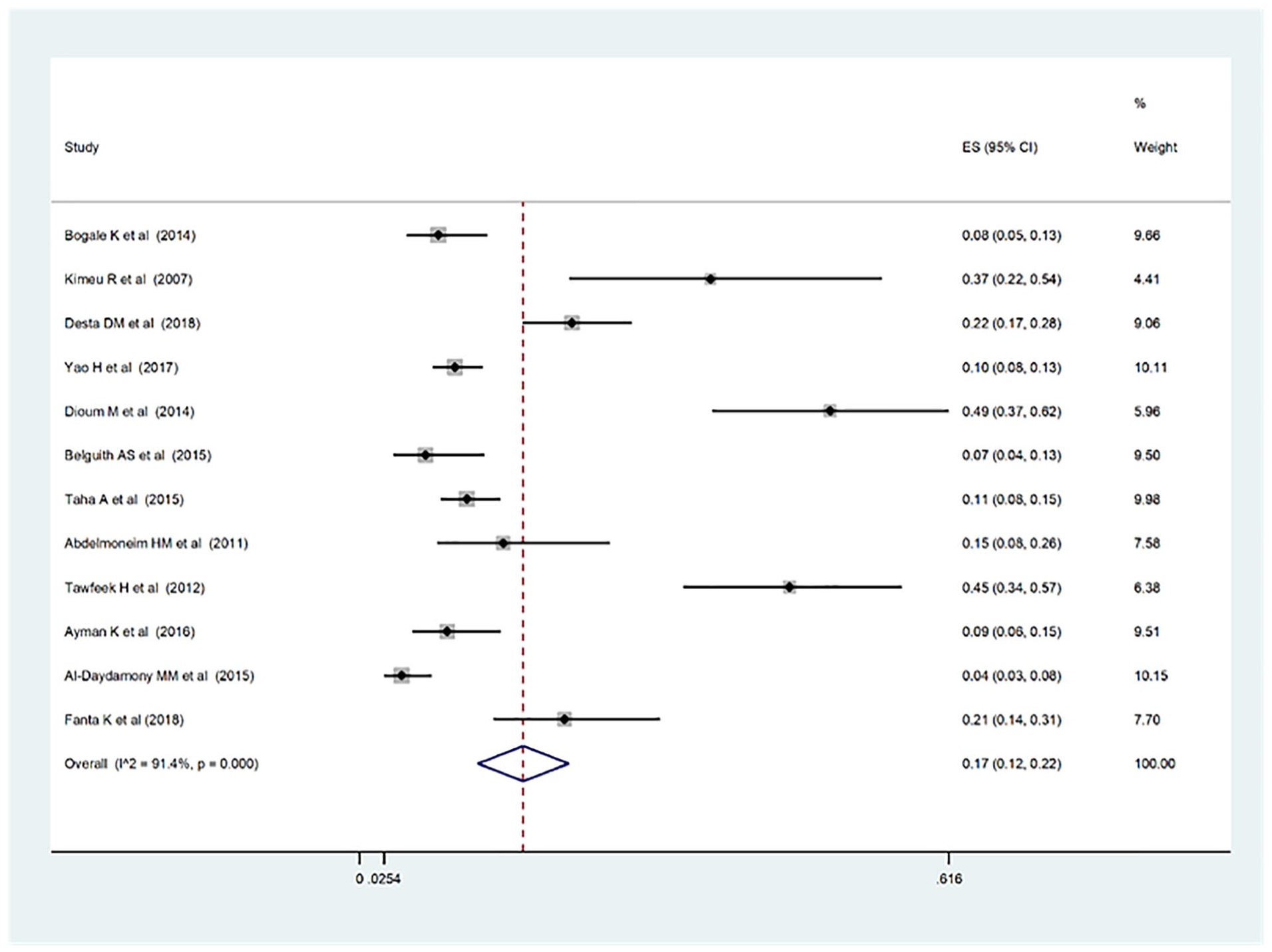
The incidence of in-hospital cardiogenic shock among patients with acute coronary syndrome in Africa.

The incidence of arrhythmia among patients with acute coronary syndrome in Africa.

The incidence of reinfarction among patients with acute coronary syndrome in Africa.

The incidence of acute stroke among patients with acute coronary syndrome in Africa.

The incidence of bleeding among patients with acute coronary syndrome in Africa.
Sensitivity and subgroup analysis
Sensitivity analysis, based on the omission of five studies12,24,36,37,40 that were considered outliers showed in the occurrence of all secondary outcomes. Besides, subgroup analysis for primary outcome showed that the incidence of in-hospital death rate in Eastern Africa 23% (PP = 0.23; 95% CI: 0.19–0.27; I2 = 38.6; p = 0.13) was comparable with the incidence in Northern Africa 22% (PP = 0.22; 95% CI: 0.16–0.28; I2 = 97.6; p = 0.00). However, the incidence of in-hospital death rate in the cardiac centers 14% (PP = 0.14; 95% CI: 0.05–0.23; I2 = 97.4; p = 0.00) was 10% lower compared to the incidence in referral hospitals 24% (PP = 0.24; 95% CI: 0.17–0.31; I2 = 96.1; p = 0.00). On the other hand, the incidence of in-hospital death rate in STEMI patients (PP = 0.14; 95% CI: 0.06–0.21; I2 = 93.7; p = 0.00) was lower than the incidence of STEMI/NSTEMI/UA (PP = 0.22; 95% CI: 0.15–0.30; I2 = 94.3; p = 0.00) combined. Likewise, it was lower than the incidence in STEMI/NSTEMI (PP = 0.26; 95% CI: 0.15–0.35; I2 = 97.1; p = 0.00) combined (Supplementary Table S1). The subgroup analysis for secondary outcomes showed that the incidence of in-hospital heart failure was comparable in Eastern (PP = 0.36; 95% CI: 0.16–0.56; I2 = 96.7; p = 0.00) and Northern Africa (PP = 0.39; 95% CI: 0.20–0.59; I2 = 99.2; p = 0.00). However, the incidence of in-hospital heart failure at the cardiac centers (69.0%) (PP = 0.69; 95% CI: 0.58–0.80) was higher when compared with the incidence in referral (36.0%) (PP = 0.36; 95% CI: 0.24–0.48; I2 = 97.1; p = 0.00) and general hospitals (35.0%) (PP = 0.35; 95% CI: 0.25–0.46). Similarly, the incidence of in-hospital heart failure among STEMI patients (57.0%) (PP = 0.57; 95% CI: 0.39–0.75; I2 = 96.4; p = 0.00) was higher when compared with the incidence in STEMI/NSTEMI combined (36.0%) (PP = 0.36; 95% CI: 0.17–0.56; I2 = 98.0; p = 0.00) (Supplementary Table S2).
The incidence of cardiogenic shock in the Eastern Africa (20.0%) (PP = 0.20; 95% CI: 0.10–0.31; I2 = 87.7; p = 0.00) was slightly higher when compared with the incidence in Northern Africa (13.0%) (PP = 0.13; 95% CI: 0.07–0.19; I2 = 90.6; p = 0.00), however, it was comparable with the incidence in referral hospitals (16.0%) (PP = 0.16; 95% CI: 0.10–0.21; I2=91.1; p = 0.00). The incidence of cardiogenic shock when STEMI/NSTEMI/UA combined (19.0%) (95% CI: 0.07–0.30; I2 = 95.7, p = 0.00) was slightly higher compared with the incidence with STEMI/NSTEMI combined (12.0%) (PP = 0.09; 95% CI: 0.09–0.15; I2 = 68.1; p = 0.00) (Supplementary Table S3).
On the other hand, the incidence of arrhythmia in Northern Africa (25.0%) (PP = 0.25; 95% CI: 0.19–0.30; I2 = 92.0; p = 0.00)] was 15% higher than the incidence in Eastern Africa (10.0%) (PP = 0.10; 95% CI: 0.05–0.15; I2 = 66.3; p = 0.03). Similarly, the incidence of arrhythmia at cardiac centers (24.0%) (PP = 0.24; 95% CI: 0.14–0.34; I2 = 97.4; p = 0.00) was slightly higher when compared with the incidence in referral hospitals (PP = 0.17; 95% CI: 0.11–0.23; I2 = 91.3; p = 0.00). However, the incidence of arrhythmia in STEMI patients (26.0%) (PP = 0.26; 95% CI: 0.12–0.39; I2 = 96.0%; p = 0.00) was comparable to the incidence of arrhythmia when STEMI/NSTEMI combined (21.0%) (PP = 0.21; 95% CI: 13–29; I2 = 92.5%, p = 0.00) (Supplementary Table S4).
Moreover, the incidence of reinfarction in Eastern Africa (7.0%) (PP = 0.07; 95% CI: 0.02–0.12) was slightly higher when compared with the incidence in Northern Africa (3.0%) (PP = 0.03; 95% CI: 0.03–0.04; I2 = 0.0; p = 0.55). Similarly, the incidence of reinfarction at referral hospitals (6.0%) (PP = 0.06; 95% CI: 0.03–0.08; I2 = 48.7; p = 0.08) was slightly higher when compared with the incidence at cardiac centers (3.0%) (PP = 0.03; 95% CI: 0.03–0.04). Moreover, the incidence of reinfarction when STEMI/NSTEMI/UA combined (6.0%) (PP = 0.06; 95% CI: 0.02–0.11) was similar with the incidence when STEMI/NSTEMI combined (6.0%) (PP = 0.06; 95% CI: 0.03–0.09), however it was slightly higher when compared with the incidence in STEMI only (3.0%) (PP = 0.03; 95% CI: 0.03–0.04) (Supplementary Table S5). Likewise, the incidence of in-hospital acute stroke was similar in Eastern (4.0%) (PP = 0.04; 95% CI: 0.01–0.08; I2 = 73.4; p = 0.01) and Northern Africa (3.0%) (PP = 0.04; 95% CI: 0.01–0.06; I2 = 75.1; p = 0.00). However, the incidence of in-hospital acute stroke at referral hospitals (4.0%) (PP = 0.04; 95% CI: 0.02–0.07; I2 = 57.4; p = 0.02) was higher when compared with cardiac centers (1.0%) (PP = 0.01; 95% CI: 0.00–0.01). Similarly, the incidence of in-hospital acute stroke in STEMI/NSTEMI/UA combined (5.0%) (PP = 0.05; 95% CI: 0.01–0.08; I2 = 74.0%; p = 0.01) was slightly higher than the incidence in STEMI/NSTEMI combined (3.0%) (PP = 0.03; 95% CI: 0.00–0.07; I2 = 73.4%; p = 0.01) (Supplementary Table S6).
The pooled estimate of bleeding incidence rate in Northern Africa (25.0%) (PP = 0.25; 95% CI: 0.01–0.51; I2 = 99.0; p = 0.00) was 23% higher compared to the incidence in Eastern Africa (2.0%) (PP = 0.02; 95% CI: 0.01–0.03; I2 = 15.9; p = 0.31). Similarly, the estimate of incidence of bleeding at referral hospitals (17.0%) (PP = 0.17; 95% CI: 0.01–0.34; I2 = 99.3; p = 0.00) was slightly higher compared to the incidence at cardiac centers (12.0%) (PP = 0.12; 95% CI: 0.11–0.13). In addition, the incidence of bleeding when STEMI/NSTEMI/UA were combined (20.0%) (PP = 0.02; 95% CI: 0.00–0.39; I2 = 99.6; p = 0.00) was slightly higher when compared with the incidence when STEMI/NSTEMI were combined (11.0%) (PP = 0.11; 95% CI: 0.07–0.15) (Supplementary Table S7).
Publication bias
The symmetrical funnel plot suggests no publication bias, however asymmetrical funnel plot indicates a publication bias (Supplementary Table S8). The Egger’s and Begg’s test were interpreted based on the p-value of test results. Thus, both Egger’s and Begg’s tests did not show the presence of publication bias for in-hospital heart failure (Egger’s test p = 0.176, Begg’s test, p = 0.893), reinfarction (Egger’s test, p = 0.081, Begg’s test, p = 0.602), arrhythmia (Begg’s test, p = 0.06, Egger’s test, p = 0.716), and major bleeding (Begg’s test p = 0.152, Egger’s test p = 0.316).
Discussion
The magnitude of ACS is increasing in recent years in Africa and the prevalence was estimated to be 0.21–22.0%. 41 This systematic review and meta-analysis assessed in-hospital outcomes of ACS among hospitalized patients in Africa. The majority of included studies were conducted in the northern region of the continent and most of them were conducted in referral hospitals. The overall estimated in-hospital death rate was 22%. The death rate was slightly lower in patients who were treated in cardiac centers (14%) as compared to patients who were treated in referral hospitals (24%). Compared to our results, a study by Orvin et al., 42 that evaluated 1188 ACS patients in Israel reported lower (10.4%) incidence of in-hospital mortality. Similarly, a multicenter study by Satoshi et al. 43 that looked at trends in the incidence, in-hospital, and long-term mortality among ACS patients reported 19.5 and 12.5% in-hospital mortality rates in STEMI and NSTEMI patients respectively. The higher in-hospital mortality rate observed in our review could reflect the growing increase in the risk factors for cardiovascular disease in low- to middle-income countries as well as delayed access to treatment.4,44
This review also identified that in-hospital heart failure was the most common (42.0%) nonfatal MACE. The occurrence of in-hospital heart failure in patients with ACS has often associated the acute myocyte loss that leads to contractile dysfunction and acute decompensated heart failure. This in turn results in structural, hemodynamic, neurohormonal, and genetic alterations. 45 The overall prevalence of in-hospital heart failure complicating ACS in this review was higher when compared with previous reports (range 2.9–19.1%).46,47,48 Acute heart failure is a frequent complication of ACS, and the combination is associated with poor prognosis and outcomes. 49 Our review identified that the occurrence of heart failure was higher in cardiac centers (69%) compared to referrals (36%) and general hospitals (35%). This possibly indicates that the cases presented to cardiac centers are those with higher rates of complications and warrant timely recognition and treatment of acute heart failure to curb the increased risk of in-hospital complications and poor outcomes of patients with ACS. 50 ACS is the most common cause of cardiogenic shock 51 and is mostly due to severely compromised left ventricular function. 52 Cardiogenic shock is the leading cause of death among patients hospitalized with ACS. 53 In our review, cardiogenic shock was the second most common (21.0%) nonfatal MACE with a significantly higher rate in referral hospitals (20%) compared to cardiac centers (10%). This perhaps reflect better quality care provided at cardiac centers compared to referral hospitals 54 and that cardiac centers are well equipped to reduce the increased risk of mortality associated with cardiogenic shock in patients with ACS.55,56
Major in-hospital arrhythmia was another common (20%) nonfatal adverse cardiovascular event identified in our review. The occurrence of cardiac arrhythmia is usually associated with larger infract, ventricular wall dyskinesia, severe coronary artery disease, and STEMI 57 and has a negative impact on patient outcomes. 58 Analysis of global ACS registry data that looked at trends of atrial fibrillation among patients with ACS hospitalized at 113 hospitals from 14 countries reported that 4494 (7.6%) out of 59,032 patients had a history of atrial fibrillation and 5.3% of them developed a new-onset atrial fibrillation during hospitalization. 59 The higher prevalence of atrial fibrillation found in this review coupled with higher rates of other cardiovascular diseases such as heart failure and diabetes imply increased risk of not just in-hospital but also long-term outcomes of patients with ACS. Therefore, there is a need for early identification of high-risk patients who would benefit from treatment with long-term mortality outcomes.60,61
Our review found that acute stroke was among the most common nonfatal MACE in patients hospitalized with ACS. Although it was less common (3%) compared to other MACE found in this review, however, stroke could be associated with significant morbidity and mortality. 62 The pooled prevalence for acute stroke was higher in referral hospitals (4%) compared to cardiac centers (1%). The emboli during revascularization or from atrial fibrillation and blood stasis in poorly functioning ventricles are some of the possible underlying causes for the occurrence of acute stroke in patients with ACS. 63 Besides, a stroke and acute myocardial infarction share similar risk factors such as hypertension, smoking, hypercholesterolemia, and diabetes.
This review also found that in-hospital bleeding was a common (14.0%) MACE in patients with ACS. It is known that major in-hospital bleeding in patients with ACS has a significant impact on disease prognosis and patient outcomes. Often bleeding could be procedure-related or due to pharmacologic therapy. The magnitude of in-hospital bleeding identified in this review was higher when compared with other studies. A systematic review and meta-analysis (42 studies, N = 533,333 patients) that looked at peri-procedural bleeding complication and its impact reported that 6.8% of patients experienced major bleeds and that major bleeding after invasive procedure is associated with a three-fold increase in mortality and MACE outcomes. 64 Likewise, a study by Steven et al. 54 that examined the impact of major bleeding among 13,819 patients with ACS reported that 4.7% of the participants experienced major bleeding. The magnitude of in-hospital reinfarction identified in our review was comparable with a larger scale study of 7930 ACS patients from Gulf registry that reported 172 (2.2%) reinfarction rate during hospitalization. 65 Overall, most of the outcomes evaluated in this review were higher when compared with the findings of studies conducted in other regions. Thus, there is an urgent need to establish new coronary units, strengthen existing cardiac services, and improve the availability and access to cardiovascular medicines to reduce the burden of ACS in the continent.
Implications
This review provides insights into in-hospital mortality rate and MACEs among patients with ACS in Africa. The findings of this review will have significant contribution toward building quality evidence on the magnitude of the problem that could inform policy, practice, and future research to reduce the burden of ACS in the continent. Additionally, such data would provide insights into the quality of current in-patient care provided for patients with ACS across healthcare facilities in the continent.
Strengths and limitations of this review
We performed a compressive evaluation of in-hospital fatal and nonfatal MACEs from studies conducted in various countries and settings in Africa.
Included studies in this review varied in their settings, design, and quality, types of ACS studied, and treatment regimen provided.
We were unable to evaluate factors associated with in-hospital mortality and the impact of nonfatal MACEs on clinical outcomes.
Moreover, the publication bias and high degree of heterogeneity were also the limitations of this study.
Conclusion
Our review of 29 studies conducted in various parts of African countries revealed that the all-cause in-hospital mortality rate associated with ACS is 22%. The mortality rate in cardiac centers was 10% lower compared to referral hospitals. The review also provides insights into the incidence of nonfatal MACE such as in-hospital heart failure, cardiogenic shock, in-hospital acute stroke, arrhythmia, bleeding, and reinfarction. The magnitude of most of the events identified in our review was higher when compared with reports in other parts of the world. This may reflect the higher burden of ACS morbidity and mortality in the continent. Therefore, establishing coronary units, strengthening existing cardiac services, and improving availability and access to cardiovascular medicines could help in reducing the burden of ACS in the continent.
Supplemental Material
sj-docx-2-smo-10.1177_20503121221143646 – Supplemental material for In-hospital mortality from acute coronary syndrome in Africa: a systematic review and meta-analysis
Supplemental material, sj-docx-2-smo-10.1177_20503121221143646 for In-hospital mortality from acute coronary syndrome in Africa: a systematic review and meta-analysis by Fuad Adem, Semir Abdi, Firehiwot Amare and Mohammed A Mohammed in SAGE Open Medicine
Research Data
sj-xlsx-1-smo-10.1177_20503121221143646 – Supplemental material for In-hospital mortality from acute coronary syndrome in Africa: a systematic review and meta-analysis
Supplemental material, sj-xlsx-1-smo-10.1177_20503121221143646 for In-hospital mortality from acute coronary syndrome in Africa: a systematic review and meta-analysis by Fuad Adem, Semir Abdi, Firehiwot Amare and Mohammed A Mohammed in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledged the staffs of the school of pharmacy, College of health and medical sciences, Haramaya University, Ethiopia
Author contributions
FA conceptualized the study. FA, SA, and FA participated extensively in searching the studies, doing the quality assessment, extracting out the relevant data, conducting the analysis, and interpreting the results. MAM is involved in conceptualization, methodology, analysis, and editing and approving the final manuscript. FA drafted and finalized the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Sharing
All data relevant to the study are included in the article or uploaded as supplementary.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.