
Abstract
Objectives:
The purpose of this study was to determine the level of satisfaction with preoperative education and surgical services among adult elective surgical patients at governmental hospitals in Addis Ababa, Ethiopia.
Methods:
Four hundred and twenty-two elective surgical patients at Addis Ababa’s governmental hospitals took part in a facility-based cross-sectional study from 8 October to 8 November 2021. Based on past experiments, an instrument for structured data collection was modified and employed. The data were cleaned and sent to Epidata version 4.2 before being exported and analysed in SPSS version 25. Descriptive statistics were used to describe the participant characteristics, and logistic regression, which also included bivariate and multivariate analysis, was used to evaluate the association between the independent and outcome variables. The level of statistical significance was indicated by a p value of 0.05.
Results:
84.6% of the participants reported feeling very satisfied with their preoperative education. Preoperative education about surgery (adjusted odds ratios (AOR) = 0.005; 95% confidence interval (CI): (0.000, 0.061)), previous surgery (AOR = 2.7; 95% CI: (2.51, 6.85)), and preoperative anxiety (AOR = 0.013; 95% CI: (0.003, 0.06)) were all significantly associated.
Conclusions:
About 84% of survey participants reported being satisfied with preoperative education and services. Preoperative patient satisfaction was negatively predicted by preoperative anxiety, prior surgery, and preoperative information about surgery. The decrease of anxiety and enhancement of surgical patient satisfaction may be significantly impacted by proper preoperative education.
Introduction
The value and reaction of patients to the care they received has been referred to as patient satisfaction. Currently, it is the healthcare system’s top priority, especially in emerging nations. Patients who are satisfied are more likely to have positive interactions with healthcare personnel and feel that their expectations, goals, and preferences have been met to some level. It is described as a complicated and individualized idea influenced by social, cultural, psychological, emotional, and physical variables. Patient satisfaction with healthcare services is an important outcome that is increasingly used as a benchmark for treatment quality.1–3
Preoperative instruction is provided by medical professionals all around the world to help patients get ready for surgery. The foundation of preoperative teaching for surgical patients consists of nursing staff providing education that takes surgical procedure preferences, medication, and dietary restrictions into account before the procedure, as well as providing instructions for after-care once a patient is discharged home. Patients can actively participate in their care and improvement through preoperative education.4–6
Patients can provide information about a hospital’s communication, education, and pain-management procedures as well as whether or not they received respect and dignity in their care. Their experiences frequently demonstrate the efficiency of a hospital system and can spark crucial insights regarding the kinds of adjustments needed to close the gap between the treatment supplied and the care that should be provided. A preoperative patient education program gives patients enough knowledge about the risks and procedure of surgery, which may help to boost their satisfaction and lower their worry.7–9
Patient satisfaction enhances communication, patient-centred attention, and a trustworthy relationship between patients and healthcare professionals. Effective communication between the patient and the surgeon prior to and on the day of operation has an impact on satisfaction as well. Patients place a great value on being respected and feeling heard by healthcare professionals.10,11
Preoperative education is the surgical nurses’ most significant duty in the preoperative patient information processes. Although more than half of participants (56.2%) were happy with the preoperative information their nurses provided, less than half said they were extremely happy (42.8%). According to studies, participants who got preoperative instruction saw their anxiety scores decline more quickly.6,12
Patients are engaged during preoperative instruction to decrease postoperative complications, boost patient satisfaction, lessen anxiety, and cut down on hospital stays. These initiatives decreased the length of hospital stays and healthcare expenses. Likewise, it drastically decreased the average duration of stay from 7 days for patients who did not receive preoperative education to 5 days for those who did.9,13
Patients are extremely afraid of dying under anaesthesia, awakening during anaesthesia, feeling postoperative pain, and experiencing postoperative nausea, according to previous patient surveys on anaesthesia. 14
High-quality patient-centred education aimed at addressing patients’ problems should begin with an understanding of the patient’s context. Prior education was significantly linked to more reasonable patient expectations and greater satisfaction. It comprises educating the patient about the process and should satisfy their expectations for the anaesthetic, preoperative medicine and fasting. Giving the patient pertinent instructions that will aid them after surgery and when they are discharged is crucial. On the other side, it has been demonstrated that preoperative education and information can increase patients’ satisfaction with the treatment they receive from medical professionals.7,13,15,16
An incidence of 60–80% has been found for patient anxiety in the operating room environment. Long surgical procedures, anaesthesia, unfamiliar surroundings, and unanticipated delays typically make patients more anxious. A third or so of patients undergoing regional anaesthesia for surgery had significant preoperative anxiety. Therefore, before having surgery, it is vital to address preoperative anxiety.17–19
There are gaps between the participant’s perspective of instruction about a surgical operation and how nursing staff provides preoperative information, according to recent studies and material examined in many journals. 4
Although preoperative patient education about the surgical process has been provided, it is insufficient and the patients still experience anxiety. As a result, this study will assess how satisfied patients are with preoperative education in order to close the knowledge gap and lower surgery patients’ lack of knowledge.
Methods and materials
Study design, study area, and period
From 8 October to 8 November of 2021, three public hospitals in Addis Ababa, Ethiopia, underwent an institutional-based cross-sectional study design. In Ethiopia, 25% of Ethiopia’s urban population resides in Addis Ababa, the nation’s capital. In 2015, the city’s health coverage rate was expected to be 52.2%. A total of 52 hospitals, 12 of which are public hospitals, are located in the city (39).
The largest teaching hospital run by the federal ministry of health is Tikur Anbessa Specialized Hospital, which is a part of Addis Ababa University’s College of Health Sciences. It receives between 370,000 and 400,000 patients annually. There are 169 specialists, 75 surgeons, 65 non-teaching doctors, 627 nurses, and 11 operating rooms among the hospital’s 850 beds, of which 181 are set aside for surgical situations (information from Tikur Anbessa’s specialist surgery department and nursing office).
The hospital was founded in 1968, and St. Paul’s Millennium Medical College, as it is presently known, was founded in 2010 by the council of ministers. Although there are more than 700 beds available for inpatient care, the college sees an average of 1200 emergency and outpatient patients each day. The college has more than 2800 clinical, academic, administrative, and supportive staff that provide medical speciality services to patients who are referred from all over the country (ST.PMH human resource).
In 1933 GC, the Zewditu Memorial Hospital was founded. It is a teaching hospital with 280 nurses, 175 beds, and other amenities. It features a regional laboratory and a dialysis centre (ZMH human resource 2021).
Populations
The source population were all elective patients visiting selected public hospitals, in Addis Ababa, Ethiopia during the study period. Study populations were randomly selected adults with elective surgical patients and who fulfilled the inclusion criteria during the study period.
Eligibility criteria
All randomly selected elective adult patients who had undergone surgery in selected public hospitals of Addis Ababa, Ethiopia in 2021 were included in the study. Those patients who came and got treated as outpatients, severely ill (unconscious) patients, and patients with known mental problems were excluded.
Sample size determination
The sample size was estimated by using single population proportion formula and assuming the level of significance (α) equals to 0.05 and marginal error of 5% and proportion of 50%.

Where, n = the required sample size
a = confidence interval (95%)
p = previous level of satisfaction 50% = 0.5 (since there is no study done on the specific topic)
d= is the margin of sampling error tolerated (5%) = 0.05
ni= (1.96)2 (0.5) (1 − 0.5)/(0.05)2 = 384
With 10% non-response rate the sample size was:
= 384 + 384 (0.1) = 422
Sampling techniques
Three hospitals were chosen by simple random sampling from the 12 governmental hospitals that operate in Addis Ababa. Proportionally, the number of participants for each hospital was distributed based on how many patients used the facility’s services each month.
According to records from each facility, Tikur Ambessa Specialized Hospital (TASH), Zewuditu Memorial Hospital (ZMH), and St. Paul Millenium Hospital (St. PMH) saw, respectively, 572, 42, and 270 patients per month. The number of participants was then estimated using the Proportional allocation formula. The number of participants is equal to Ni × n/N, where Ni is the number of patients who visit the hospital per month for services, n is the sample size of 422, and N is the sum of the total number of patients who visit each hospital each month for services.
According to the aforementioned calculation, there were 266, 21, and 133 participants from TASH, ZMH, and St. PMH, respectively. Finally, a list of the patients scheduled for surgery was received from the ward based on the number of beds, after which every other patient was taken into consideration in order to choose a specific study unit (Figure 1).

Schematic representation of sampling procedure on patient satisfaction towards preoperative education in selected public hospitals of Addis Ababa, Ethiopia, 2021.
Operational definitions
Patient satisfaction: This is defined as a subjective reaction to the context, process, and result of the service experience one has received.
Good satisfaction: The mean was derived after computing each respondent’s individual response for the satisfaction questions. Scores over the median (50%) were seen as indicating high levels of satisfaction.
Poor satisfaction: The individual response for each satisfaction question was computed and then those scored less than or equal to 50% of the total questionnaires were considered as having poor satisfaction. 6
Adult: People who have attained a certain age, typically eighteen, and are regarded by the law as being able to manage their own affairs.
Study variables
Dependent variable was patient Satisfaction towards preoperative education. Independent variables were Socio-demographic factors, patient and family factors, Institution-related factors and Health providers-related factors.
Statistical analysis
Patients who met the inclusion criteria and those who were admitted to the preoperative unit during the study period at chosen public hospitals had their data collected through face-to-face interviews. Excel was used to examine and clean the data before being exported to SPSS version 25 for analysis. The analysis was not conducted on data that were inconsistent or incomplete. To describe the sample, descriptive statistics were used. As percentages and frequencies, the descriptive statistics’ findings were presented.
Bi-variable analysis was used to initially discover characteristics that were linked with the result variable by analysing associations between independent and dependent variables. To control confounding variables, multivariable logistic regression analysis was used to those components that were found to have a correlation with the outcome variable at p = 0.2 and that fit the binary logistic regression model.
Using adjusted odds ratios (AOR) and the 95% confidence interval (CI), the strength of the correlation between the various independent factors and the dependent was calculated. p Values below 0.05 were considered statistically significant. Tables and graphs were used to present the results, and conclusions were reached in light of them.
Data collection instrument
A standardized and structured set of instruments was adapted from many literary works. The information was then gathered using this standardized questionnaire that was presented by an interviewer. Experts translated each question from its original English version into Amharic, and then, for consistency, they all were translated back into English. Four sections make up the questionnaire.
Part I: Sociodemographic characteristics of adult elective patients
Age, gender, educational status, residence, and so on.
Part II: Patient satisfaction on preoperative education
The tools include inquiries on patient satisfaction levels and contains 22 questions. Each question is scaled from 1 to 5, the theoretical ranges and categorization limits for the total variables were as follows: 1.00–2.49 = poor, 2.50–3.49 = satisfactory, and 3.50–5.00 = good.
Each item in the survey was given a rating between 1 and 5, and all response types were translated into percentages. Consequently, a five-point Likert-type scale with an extremely unhappy 1, unhappy 2, neutral 3, satisfied 4 & very satisfied 5. Numbers 1 through 5 were transformed into percentages as follows: 0 = 0%, 2 = 25%, 3 = 50%, 4 = 75%, and 5 = 100%. As a result, people with scores higher than 50% are considered to have good contentment, while those with scores of 50% or below are considered to have poor satisfaction. 6
Data about patient satisfaction on preoperative education was collected by using structured questionnaire tools which was adopted from previously conducted research on Patient satisfaction with the perioperative surgical services and associated factors at a University Referral and Teaching Hospital in Gondar Ethiopia. 20
Part III: Preoperative education
Structured questionnaire techniques that were adapted from earlier research on patients’ experiences with informed consent and preoperative education in Turkey were used. The questionnaire has 16 total questions and the mean was derived after computing each respondent’s individual response to the questions. Those who performed better than the average were deemed satisfied. 6
Data collection methods
To gather data on patient satisfaction with preoperative education and related parameters, an interviewer-administered questionnaire was used. The investigators were in charge of the project’s general workflow, the creation of the final questionnaire, securing the participation of the chosen patients, and designating data collectors (DCs) and supervisors.
Three trained BSc nursing professionals who were allocated preoperatively to each of the three institutions and were overseen by two BSc nurse professionals served as the DCs. The daily overall supervision was made by the investigators.
Data quality assurance
The questionnaires were pretested in the Menelik II referral hospital using 5% of the sample size, which translates to 21 study units, to ensure the quality of the data. Two days of training for both the DCs and the supervisors covered the process of data collection and supervision. To ensure consistency and semantic comparability, the questionnaire was translated from English into Amharic and then back into English by a different person.
Prior to the actual data collection, the data collecting instrument was evaluated for completeness, consistency, and application, and significant changes were made. The study’s procedures allowed for anonymous and voluntary participation, which preserved the patient’s privacy. For controlling mistakes during data analysis, a frequency check was conducted.
Results
Sociodemographic characteristics of adult elective patients
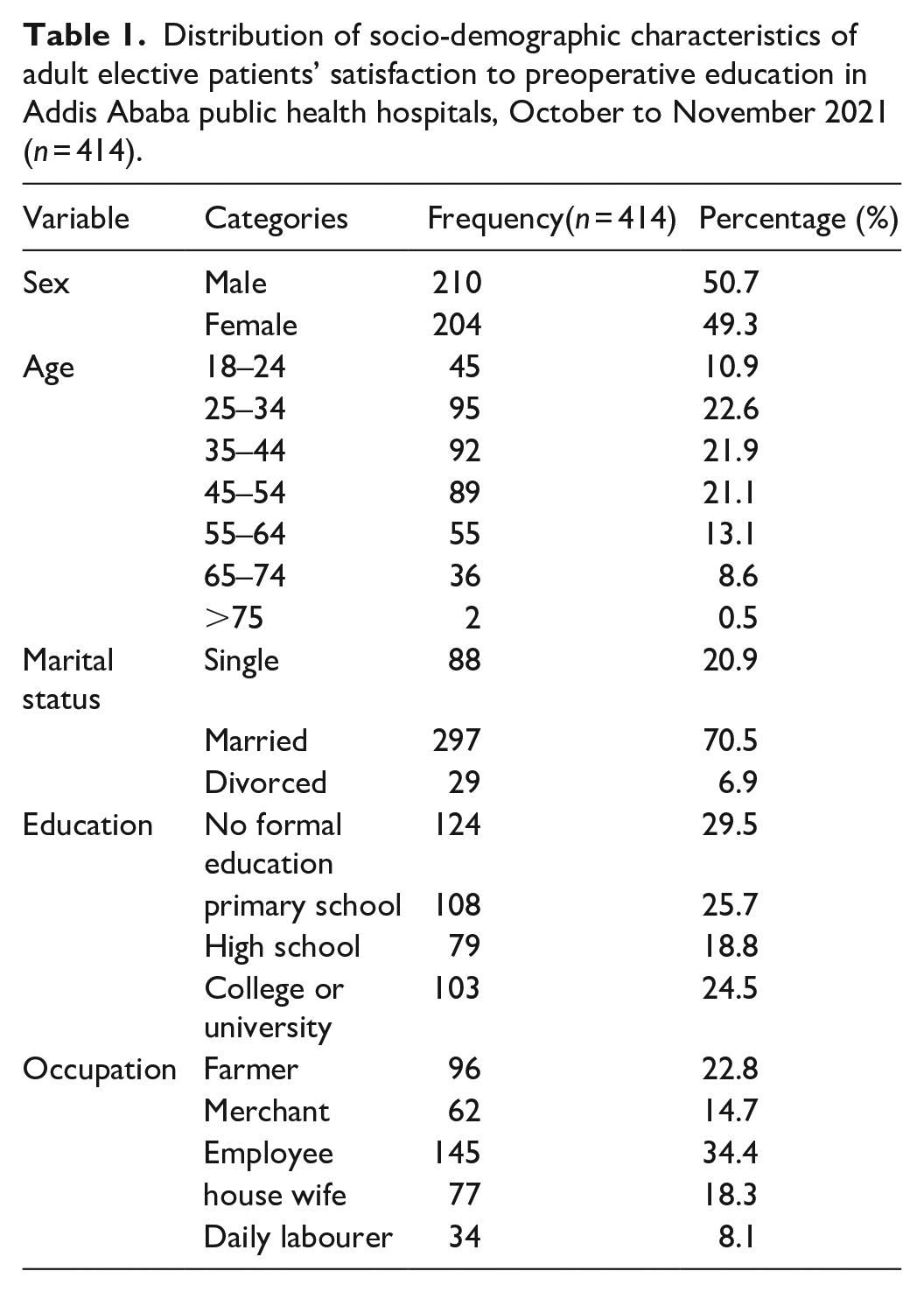
The study included a total enrolment of 422 participants, with a 98.1% overall response rate; 49.9% of the participants, or 210 people, were men. 95 (or 22.6%) were discovered in the 25–34 age range. About 124 (29.5%) of the total respondents had no formal education, while 79 (18.8%) had just completed high school (Table 1).
Distribution of socio-demographic characteristics of adult elective patients’ satisfaction to preoperative education in Addis Ababa public health hospitals, October to November 2021 (n = 414).
Percentage and frequency of factors associated with satisfaction towards preoperative education
From the total surgery-appointed patients’ group, those requiring abdominal surgery were the highest at 104 (25%). More than half of the participants 325 (78.5%) experienced preoperative fear and anxiety whereas 89 (21.1%) did not experienced preoperative fear and anxiety. Those having a fear of surgery-related death were 106 (25.2%), those who were undergoing complicated surgery and pain were 35 (8.3%), and those who felt they would never be the same again after surgery were 69 (16.4%). In terms of duration of illness 168 (40.6%) were in months’ and 118 (28.5%) were in days’ duration. Of them, in terms of surgery waiting time, 258 (62.3%) were less than 1 month and 53 (13%) were 3–6 months (Table 2).
Percentage and frequency of factors associated with preoperative education and other services among adult elective surgical patients at public hospital of Addis Ababa, October to November 2021.

Patient satisfaction towards preoperative education among adult elective surgical patients
Overall satisfaction of adult elective surgical patients was calculated using satisfaction to preoperative education which contains 24 questions. Using this score, 346 participants (83.6%), have good satisfaction and the prevalence of poor satisfaction to preoperative education was 68 (16.4%) (Figure 2).

Patient satisfaction to preoperative education in Addis Ababa public health hospitals, October to November 2021 (n = 414).
Patient satisfaction towards preoperative education
Among the respondents 165 (39.2%) were dissatisfied and 149 (35.4%) of them were satisfied, about adequacy of information provided and the possible complications that may occur during operation or treatment. Two hundred six (49.8%) patients were dissatisfied about the importance of information given by the ward nurses regarding the importance of laboratory investigations. Most of the participants 168 (39.9%) were dissatisfied, about accessibility of pharmacy and laboratory facilities while 64 (15.2%) were satisfied (Table 3).
Factors associated with patient satisfaction on preoperative education among adult elective surgical patients in Addis Ababa public hospitals, October to November 2021(n = 414).

AOR: adjusted odds ratio; COR: crude odds ratio; CI: confidence interval.
Statically significant at p value 0.05.
Factors associated with patient satisfaction on preoperative education
Both bi-variable and multivariable logistic regression analysis were implemented to determine the factors that associated with patient satisfaction on preoperative education. At bi-variable analysis the factors associated with overall Patient satisfaction on preoperative education includes the following: Gender of the participants and Payment status for treatment with crude odds ratio (95% CI): 0.76 (0.28, 5.62) and 0.60 (0.14, 3.04), respectively.
In multivariable analysis model, the result revealed that participants who had no preoperative fear/anxiety were 0.013 times less likely to have satisfaction on preoperative education when compared to those who had preoperative fear/anxiety AOR (95% CI): 0.013 (0.003, 0.067).
Similarly, the participants with no previous surgery were three times more likely to have satisfaction on preoperative education when compared to those who had Previous surgery AOR (95% CI): 2.7 (2.51, 6.85).
Participants with poor preoperative education about surgery were 0.005 times less likely to have satisfaction on preoperative education when compared to participants with good preoperative education about surgery AOR (95% CI): 0.005(.000, 0.061)
Whereas, kind of fear/anxiety, duration of the illness, number of admissions, perceived patient’s service expectation, self-rated health status during interview were not associated with patient satisfaction on preoperative education (Table 3).
Discussion
This study assessed the level of patient satisfaction and factors associated with patient satisfaction on preoperative education in three public hospitals of Addis Ababa, Ethiopia. The results of this study showed that the patients were satisfied, response to preoperative education was good in 83.6% of the total participants. This level of good patient satisfaction was lower than what has been reported in Gondar. This discrepancy might be due to study setting of hospital being over crowded. However, when compared to what has been reported in Turkey it is a better report. The difference might be due to difference in the study setting and sample size.6,20
This study showed that participants who had no preoperative education were 0.005times less likely to have satisfaction on preoperative education than those who had preoperative education. This is due to the reason that patients who have good preoperative education manifest good satisfaction from the preoperative education as they get enough understanding about the procedures. Reports from different countries also found that lack of preoperative education is significantly associated with low quality of life and poor satisfaction.8,21
Patients who had no preoperative anxiety were 98.3% more likely to have satisfaction on preoperative education when compared to those who had preoperative fear/anxiety. This study result was higher than in the study conducted in Turkey. This discrepancy might be due to the difference in the number and type of healthcare providers in those mentioned service delivery places and the variety of activities they run in their respective study areas. 22
A Study result revealed that, patients who have had no previous surgery had three times more likelihood of satisfaction on preoperative education than those who have had previous surgery. This is similar to the study done in Turkey. This similarity might be due to the patient’s past experience of suffering from the previous surgical trauma, hospital stay, and cost incurred. 22
However, there is no significant relationship between gender of the participants, and level of patient satisfaction on preoperative education; Whereas this finding contradicts a report from Sohang university (south Korea) which showed that male patients were more satisfied than females during the preoperative education period. 23
The report from this study concluded that there is no significant association between ages of surgical patients and their satisfaction toward preoperative education. Furthermore, the number of admissions to surgical ward has no association with satisfaction which was a contrary findings with the study from Turkey. 22
In this study, the patients who were dissatisfied with the information that had been given by physicians and nurses about the nature of the problem or operation were numbering to 136 (32.3%). These degrees of dissatisfactions were high compared with a previous study conducted in Jimma specialized University hospital. This might be due to sample size difference. 24
The study showed that communication gap between the patient and physicians resulted in patient dissatisfaction on preoperative education at 104 (24.7%). This report value was higher compared with a previous study conducted in Gonder specialized teaching hospital. 20
Generally, preoperative education increases the patient’s satisfaction toward the procedure. This understanding about the nature of their problem helps to lower negative emotional response and increase patient’s satisfaction.9,15 This result was similar with a previous study conducted in Turkey. This might be due to better understanding about their surgical procedure after preoperative education.9,13
Strengths and limitations
Strengths: The study used primary data which increases the reliability of the data. Additionally, the study used validated tool, thus it enables comparison as the reliability and validity of the instrument is high.
Limitations: This study is not without limitations. First, only Public health institutions were included in the study due to resource constraints. Next, absence of previously published data in Ethiopia makes comparison and discussion difficult. Then, the data on patient satisfaction towards preoperative education among adult elective surgical patients was also collected through self-reporting rather than direct observation which may cause recall and social desirability biases.
Conclusions
From the participants more than three-fourth of adult elective surgical patients who participated in this study had good satisfaction towards preoperative education. Among independent variables preoperative fear/anxiety, previous surgery and preoperative education about surgery were significantly and negatively associated with the patient satisfaction.
Recommendations
This study revealed that there is a need to improve patient satisfaction towards preoperative education. The following recommendations are forwarded to the respective stake holders:
For policy makers/health institutions management and Addis Ababa health bureaus
The investigator wishes to recommend to:
Organize and provide continuous refreshing trainings on patient satisfactions to preoperative education and related topics for healthcare providers to improve patient satisfactions so that they can share their knowledge with all surgical patients.
Work with higher stake holders to prepare comprehensive guidelines for ensuring patient satisfaction to preoperative education.
Advocating for adherence to preoperative education by using mass media like television, radio, face book and the like.
For healthcare providers
The healthcare providers working in surgical clinics should provide preoperative education both separately and with the family of the surgical patients on how to improve self-management during preoperative period.
The healthcare providers working in surgical clinics also should prepare preoperative education that can increase patient’s understanding about the planned procedure.
For future researchers
It is recommended to do further study by including private health institutions to increase the representativeness of the study.
Emphasize on the organizational and healthcare provider-related factors which were not well covered in this study but are associated with patient satisfaction towards preoperative education.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221143219 – Supplemental material for Satisfaction with preoperative education and surgical services among adults elective surgical patients at selected public hospitals in Addis Ababa, Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221143219 for Satisfaction with preoperative education and surgical services among adults elective surgical patients at selected public hospitals in Addis Ababa, Ethiopia by Dereje Deressa, Tigistu Gebreyohannis, Abdisa Boka and Yomilan Geneti in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our deepest gratitude to participating hospitals, data collectors, supervisors, and the study participants for their kind and invaluable contributions. Without them this study wouldn’t have been realized.
Author contributions
DD, conceived the study. All were involved in the design, field work, data analysis and interpretation and report writing. In addition, DD, TG, AB, and YG were involved in the manuscript preparation. All authors reviewed, read, and approved the final version of the manuscript.
Availability of data
Addis Ababa University electronic database library and in all other instances, however, by requesting the author of thesis and corresponding author permission will be obtained.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of Addis Ababa University, College of health sciences, School of Nursing and Midwifery (Form: AAUMF/03/008, Protocol N
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects and legally authorized representatives of illiterate subjects before the study initiation. Participants of the study were briefed about the objectives and aims of the study in detail. Participants were informed that their participation was purely voluntary and were assured of the confidentiality of all information. Confidentiality of the data was assured throughout the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.