
Abstract
Objectives:
Early surgery is recommended for hip fractures in elderly patients. This study was performed to evaluate factors contributing to delayed surgery and associated outcomes in a secondary hospital in Japan with a rehabilitation centre.
Methods:
We retrospectively reviewed the records of 895 patients aged >50 years [median age, 86 (81–91) years] treated for hip fractures at our institution from 2016 to 2020. We defined surgical delay as surgery performed >48 h after admission. We evaluated several risk factors for surgical delay and associated outcomes: mortality, length of hospital stay and walking status.
Results:
Binomial logistic regression analysis showed that several factors, including preoperative echocardiographic delay (odds ratio, 9.38; 95% confidence interval, 5.95–15.28), were risk factors for surgical delay. In the multiple regression analyses, surgical delay was a significant risk factor for a longer hospital stay (partial regression coefficient, 6.99; 95% confidence interval, 3.67–10.31).
Conclusions:
Our findings indicated that preoperative echocardiographic delay was one of the risk factors for surgical delay of hip fractures in elderly patients. Surgical delay was a risk factor for a longer hospital stay, including rehabilitation.
Introduction
Hip fracture is a common injury in patients of advanced age and results in high morbidity and mortality rates. 1 The total number of hip fractures worldwide is increasing and is estimated to reach 4.5 million by 2050. 2 Surgery is still the primary treatment option for hip fractures. The timing of surgery is regarded as a major modifiable predictor of mortality, complications and healthcare costs. 3 Therefore, it is recommended across orthopaedic departments worldwide that surgery be performed within 24–48 h of fracture. 4 However, surgical delay in patients with hip fractures has been reported globally. 5 Elderly patients with hip fractures often require adequate preoperative evaluation, and surgery is often delayed.
Japan has one of the most rapidly aging populations worldwide, 6 and our institution is located in a region of Japan with a high aging population. In Japan, surgeries are performed not only in large general hospitals including trauma centres but also in smaller hospitals. Our institution is a 200-bed secondary hospital that also performs surgeries and includes a 100-bed rehabilitation centre. To the best of our knowledge, most reports of hip fractures have been from large general hospitals or national registries.7,8 To the best of our knowledge, there are no reports of hip fractures in institutions such as ours, which offer all care from surgery to rehabilitation. In addition, the benefit of surgery within 48 h has been reported 4 but the risk factors for surgical delay and the long-term benefits of avoiding surgical delay have not been clearly identified.
We hypothesised that risk factors specific to our institution as a secondary hospital (e.g. lack of cardiologists, anaesthesiologists and availability of care on holidays) exist for a >48-h surgical delay in patients with hip fracture. The primary aim of this study was to identify the risk factors for a >48-h wait time for hip fracture surgery in our institution. The secondary aim was to evaluate the impact of surgical delay on the following outcomes: in-hospital mortality, 1-year mortality, length of acute care and total hospital stay, and walking status at discharge.
Materials and methods
Participants
We retrospectively reviewed the records of 968 patients aged >50 years who were treated for hip fractures at our institution from 2016 to 2020. In Japan, the incidence of hip fracture has been reported to increase from the age of >40 years. 9 However, we included patients aged >50 years in our study because the mechanism of injury in patients in their 40s was high-energy trauma, not falls. The exclusion criteria were transferred to a different hospital (n = 29) and conservative treatment with no request for surgery or transfer (n = 44). After applying the exclusion criteria, the final number of included patients was 895.
Data extraction and variables
We assessed several clinical characteristics that previous research has suggested affect the outcomes of interest.10–12 Data on these characteristics were collected from the patient’s medical records. These clinical characteristics were sex, age, admission day and time, general health status according to the American Society of Anaesthesiologists (ASA) classification, time to preoperative echocardiography, time to surgery, fracture site (femoral neck/trochanter), surgery type (arthroplasty/osteosynthesis) and walking status before injury. We assessed the walking status before injury by interviewing the patients and their families. The anticoagulation status has been reported to be a risk factor for surgical delay.13,14 In this study, however, we did not include the anticoagulation status as a variable. In accordance with previous studies, we make surgical decisions regardless of the anticoagulant status.
The admission was defined as weekend admission if it took place between 00:00 on Saturday and 23:59 on Sunday. We defined out-of-hours admission as admission outside the hours of 09:00–17:00. The time of surgery was calculated from the time of admission to the time of surgery. The most widely accepted guideline for the timing of surgery is within 48 h of injury. However, the time of injury was uncertain in this study because it was based on interviews with the patients and their family members. We defined surgical delay as surgery performed >48 h after admission. We evaluated preoperative echocardiography in all patients in our institution. All 895 patients involved in the study underwent preoperative echocardiography. The time to preoperative echocardiography was calculated from the time of hospital arrival to the end of the examination. Delayed examination was defined as >24 h. Preoperative echocardiography results were assessed by a cardiologist. The functional outcome was assessed in terms of the walking status, which was assessed before the fracture and at discharge using the following categories (from best to worst): able to walk without help, able to walk with a walking cane, able to walk with a walking frame and unable to walk.
Primary and secondary outcomes
The primary outcome in this study was a >48-h surgical wait time for hip fracture surgery at our institution. The secondary outcomes were in-hospital mortality, 1-year mortality, length of hospital stay and walking status at discharge from the rehabilitation centre.
Statistical analysis
Data are presented as the mean and standard deviation for normally distributed values and as the median and interquartile range for non-normally distributed values. Continuous data were analysed using Student’s t-test or the Wilcoxon rank sum test according to their distribution, while categorical data were analysed with the chi-squared test or Fisher’s exact test. A multivariate analysis was performed to adjust for potential confounders. The results are summarised as odds ratios, 95% confidence intervals, partial regression coefficients, and p values. A p-value of <0.05 was considered statistically significant. All statistical analyses were carried out using JMP pro 16.0 (SAS Institute, Cary, NC, USA). The sample size was calculated using JMP with a power value of 0.8 and a significance level of 0.05. In our evaluation of the major outcome (length of hospital stay), we considered 5 days to be a clinically meaningful difference with a standard deviation of 25 based on previous reports,5,15 resulting in a minimum sample size of 790 patients.
Results
A total of 324 (36.2%) patients underwent surgery within 48 h of admission (Table 1). The proportion of patients who underwent surgery within 48 h was 16.4% in 2016, 24.0% in 2017, 34.9% in 2018, 40.9% in 2019 and 62.9% in 2020; that is, the number of patients whose surgery was delayed decreased each year. Of the independent variables examined, weekend admission, preoperative echocardiographic delay, fracture type and surgery type showed a significant difference between patients who underwent surgery within 48 h and patients with surgical delay (Table 1). The binomial logistic regression analysis showed that preoperative echocardiographic delay and arthroplasty surgery were risk factors for a >48-h wait time for hip fracture surgery (Table 2). We excluded femoral neck fracture from the regression model because of collinearity with arthroplasty surgery.
Comparison of clinical characteristics between patients who underwent surgery within 48 h and patients with surgical delay.

ASA: American Society of Anaesthesiologists.
Data are presented as n (%) or median (interquartile range).
Preoperative echocardiography was performed in all patients.
Delayed examination was defined as >24 h.
Binomial logistic regression analysis of risk factors for surgical delay.

OR: odds ratio; CI: confidence interval.
Coefficient of determination (R2) = 0.24.
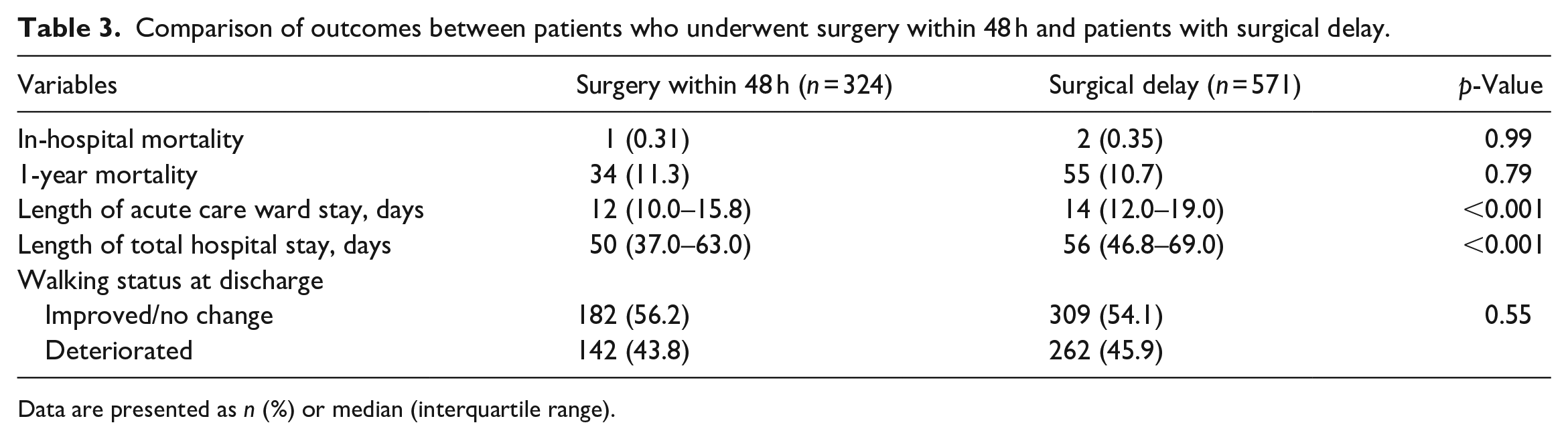
Among the patients who underwent surgery, three (0.3%) died during hospitalisation, and the difference in mortality according to surgical delay was not statistically significant. In addition, 1-year mortality and deterioration of the walking status at discharge were not significantly different between patients with and without a >48-h wait time for hip fracture surgery. The length of acute care ward stay and total hospital stay were significantly different between the two groups (Table 3).
Comparison of outcomes between patients who underwent surgery within 48 h and patients with surgical delay.
Data are presented as n (%) or median (interquartile range).
In the multiple regression analyses adjusted for sex, age, surgery type, weekend admission and walking status at discharge, surgical delay remained a significant risk factor for a longer hospital stay (Table 4).
Multiple regression analysis of risk factors for increased length of total hospital stay.

B: partial regression coefficient; CI: confidence interval.
Coefficient of determination (R2) = 0.11
Discussion
Several reports have shown that the risk of surgical delay for hip fracture is increased by various factors, including weekend admission,16,17 fracture type, 5 surgical type, a high ASA score,11,15 securing an operating room 5 and anticoagulant use. 11 Among the independent variables examined in the present study, weekend admission was a risk factor for surgical delay. Weekend admission was associated with difficulty securing anaesthesiologists and operating room staff because surgeries were performed on holidays. The multivariate analysis showed that the risk factors for surgical delay of >48 h were arthroplasty surgery and preoperative echocardiographic delay. Arthroplasty surgery was associated with surgical delay because preparing implants and securing surgeons and assistants were more difficult than for osteosynthesis. Our findings suggest that preoperative echocardiography may have an influence on surgical delay in patients with hip fractures.
The effect of preoperative echocardiography on the outcome of patients who undergo surgical treatment of hip fracture remains controversial.18–21 Most patients with hip fractures are older and have multiple comorbidities, especially cardiac disease. Therefore, preoperative echocardiography is required to identify cardiovascular risks that may increase postoperative mortality. 22 Canty et al. 23 reported that among patients who underwent echocardiography, mortality was lower both during the first 30 days postoperatively and within 12 months postoperatively. Chang et al. 20 reported that preoperative echocardiography was associated with postoperative mortality and also resulted in surgical delay. Preoperative identification of cardiac abnormalities may improve perioperative management and reduce postoperative complications and mortality. 21 In this study, the in-hospital mortality rate was significantly lower than that in other studies. The reason for this might be that patients with severe cardiac morbidity detected by preoperative echocardiography were transferred to hospitals with more advanced medical treatment.
By contrast, Yonekura et al. 18 reported that preoperative echocardiography was not associated with mortality or postoperative complications in a propensity score-matched cohort including more than 50,000 patients from a nationwide inpatient database in Japan. According to the American College of Cardiology/American Heart Association practice guidelines, 19 unnecessary echocardiographic examinations should be reduced, and we should also avoid routine examinations. In any case, preoperative echocardiography should be considered an urgent test to prevent surgical delay. However, secondary hospitals such as ours do not have a full complement of cardiologists, which leads to delays in echocardiography and ultimately surgery. This suggests that the optimisation of medical care might be difficult to achieve.
Surgical delay of hip fracture reportedly increases the risk of preoperative and postoperative complications, 24 mortality,25,26 a poor functional status25,27 and a longer hospital stay.24,28 In the present study, surgical delay of >48 h was associated with a longer total hospital stay, including both in the acute care ward and the rehabilitation unit. Longer hospital stays lead to rising costs 29 ; thus, surgical delay may be detrimental from a financial standpoint as well. In addition, prolonged hospitalisation is associated with an increased risk of debility in elderly patients. 30 It is necessary to prevent surgical delay for patients with hip fractures to the greatest extent possible.
Our study has several limitations. First, it was a retrospective analysis rather than a randomised controlled trial. Many factors that influence the risk of surgical delay in hip fracture have been reported.5,11,15–17 In our study, there were no significant differences in sex, age, out-of-hours admission, preoperative ASA score or walking status before the injury. However, factors that could not be assessed, including anticoagulant status, may have distorted our results because of the lack of randomisation. Second, we lacked data on postoperative complications. The patients had multiple and varied postoperative complications, making it difficult to accurately assess these complications. Therefore, we were unable to ascertain whether surgical delay affected complications or extended the hospital stay. Third, the data were drawn from a single institution, namely a secondary hospital that provides total rehabilitation. Generalisation of the conclusions may be limited. Fourth, the sample size was slightly larger than initially calculated, which might have influenced the observed differences. However, we believe the results remain significant and meaningful, suggesting the involvement of factors beyond just the sample size.
One of the strengths of our study is that although previous studies have evaluated hip fracture and surgical delay, most were from trauma centres and acute care hospitals; few have been reported from secondary hospitals such as ours, which provides total rehabilitation. The length of the total hospital stay, including rehabilitation, may be accurate. Surgical delay depends on both patient and hospital factors, 31 and our findings are useful for other populations and settings where surgery is performed in a secondary hospital. Another strength of our study, although controversial, is that all patients underwent preoperative echocardiography. To the best of our knowledge, there are no previous reports describing the performance of echocardiography in all patients undergoing hip fracture surgery along with the survival rate and length of hospital stay. In addition, although there have been studies of surgical delay in which the presence or absence of preoperative echocardiography was assessed as a risk factor, few studies have assessed the timing of echocardiography (e.g. a delay of >24 h, as in the present study) as a risk factor for surgical delay. Addressing these issues will benefit both patients and physicians involved in the increasing number of hip fractures in recent years. Our findings apply to secondary hospitals that provide total rehabilitation because hip fracture affects all older populations worldwide.
Conclusion
Our findings indicated that preoperative echocardiographic delay was one of the risk factors for surgical delay of hip fracture in elderly patients. Surgical delay was a risk factor for a longer hospital stay, including rehabilitation.
Footnotes
Acknowledgements
Authors’ contributions
MK and YF designed the study and wrote the manuscript. MK, YA and YT collected the clinical data. MK and YF analysed the clinical data. TO and NT critically revised the manuscript for important intellectual content. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study protocol was approved by the Clinical Ethics Committee of Kohshinkai Ogura Hospital (no. 2022-B14) and was performed in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All patients provided written informed consent for the publication of their medical data.
Informed consent
Written informed consent was obtained from all patients before the study. We did not obtain written informed consent from the legally authorised representatives of the deceased patients prior to study initiation because this requirement was waived by the Institutional Review Board/Ethics Committee.
Trial registration
Not applicable.