
Abstract
Introduction:
Orthopaedic procedures are associated with the highest rates of opioid use among surgical specialties. Factors such as time constraints, communication barriers, and variable patient preferences are recognised challenges. There is limited research explicitly addressing the drivers for opioid prescribing in surgical patients or seeking to understand how health professionals engage patients in decision-making. This study aimed to explore patient and healthcare professional perceptions of the role of opioids in pain management in the orthopaedic context.
Methods:
This research adopted a qualitative study design underpinned by critical realism. Interviews were conducted with patients and healthcare professionals involved in the care of patients with pain in an orthopaedic setting at a metropolitan tertiary hospital in South Australia. Analysis of the interviews was informed by a reflexive thematic analysis approach.
Findings:
Forty participants (20 patients and 20 healthcare professionals) participated in this study between June and October 2020. A total of three themes, with sub-themes were identified (1) The patient as an individual; (2) the acute care setting; and (3) patient engagement and education. It was clear from both patient and healthcare professional participants that individual patient factors influence patients’ understandings of opioids and pain management as well as the acute care setting. Additionally, all participants described the importance of patient engagement and education for improvement in pain management and opioid use.
Conclusions:
This study demonstrates the complex factors that influence pain management and opioid perceptions within the orthopaedic context. We recommend that patient engagement and education is the critical factor to navigating individual patients and the acute care setting when it comes to pain and pain management.
Introduction
Orthopaedic procedures are associated with the highest rates of opioid use amongst surgical specialties. 1 Prescribing commences pre-procedure, 2 or in the immediate post-operative period and is consistently linked to long-term dependence. 2 Despite well-documented risks associated with opioids, including overdose, mortality and chronic dependence, opioids remain a cornerstone of post-operative pain management in surgery.3–5 There is a growing body of literature to support alternate pain management strategies including use of multi-modal analgesia, 6 education interventions 7 and prescription monitoring systems in reducing the prescribing of opioids.3,8,9 However attempts to reduce the rates of opioid prescription are having limited effects on long-term rates of dependence and overdose underscoring a critical gap in understanding the drivers of opioid prescription and administration and ongoing use from both patient and provider perspectives.10–13 Post-operative reliance is driven by complex interactions between patient needs and experiences, healthcare provider practices and systemic factors. Qualitative studies emphasise patients’ reliance on opioids for pain control and healthcare providers’ challenges in balancing risk mitigation strategies with effective pain management. 10 Factors like time constraints, communication barriers and varied patient preferences are recognised challenges; however, there is limited research explicitly addressing the drivers for opioid prescribing in surgical patients or seeking to understand how health professionals engage patients in decision-making. 14 Therefore, this research aims to explore these dynamics to inform strategies that reduce opioid dependency while optimising postoperative pain care.
Strong evidence alone is not sufficient to change practice. 15 It is important to understand the contextual factors that promote or hinder evidence-informed change. 15 Despite a lot of research describing the opioid problem, 16 there are few qualitative studies that explore the drivers and contextual factors that influence opioid prescription. 17 Whilst qualitative studies explore the post-operative pain management educational needs of patients, 18 and their experience of pain 19 they expose a complex interplay influenced by personal experiences, assumptions regarding addictive personality traits and external influences. 20 These studies reveal that there is a still much we need to learn about patients experiences of pain management and opioid use, to enable us to understand what is needed to embed the best available evidence into practice. 21 This is a critical gap that needs addressing so that meaningful and sustainable change can be implemented in practice. Therefore, the overall aim of this research was to explore patient and healthcare professional perceptions of the role of opioids in pain management in the orthopaedic context.
Methods
Study design
This study adopted a qualitative study design underpinned by critical realism. 22 Taking this approach allowed us to undertake a broad examination of a real-world problem whilst acknowledging the complexities and influence of individual perspectives and experiences. Interviews were conducted with patients and healthcare professionals in an orthopaedic unit at a metropolitan tertiary hospital in South Australia. Ethics was approved by the Central Adelaide Local Health Network Human Research Ethics Committee (reference number: 12836). Informed written consent was gained from all participants. The consolidated criteria for reporting qualitative research checklist was used to ensure accurate reporting. 23 Two of the team members have PhDs (LBS, SCH) and many of the team members have extensive experience in conducting qualitative research (SM, JC, LBS, SCH). SM is an education researcher and pharmacist with clinical experience in a broad range of clinical areas including surgery, intensive care and rehabilitation medicine but also a personal experience with chronic pain. JC, VS, PW, SB, SF are all hospital clinical pharmacists working primarily in the surgical and orthopaedic space at the time of the study. LBS is a physician having worked for more than 20 years in the specialty of orthopaedics. At the time of the study, JB was a medical student, having completed general medical rotations. SCH is trained in psychology and has worked as an implementation scientist on projects focused on health since 2018. Throughout the research process, the researchers reflected on personal experiences and interests and how this may influence our analysis. We considered the data and whether it reinforced or refuted our assumptions about pain management and opioid use in hospital and beyond. For example, some members of our team were surprised that most of prescribing of opioids is undertaken by our most junior doctors (intern medical officers), and that some patients were quite fearful of becoming addicted to opioids.
Participants and recruitment
Patients and healthcare professionals at one metropolitan tertiary hospital in South Australia were recruited. The orthopaedic unit provides care to 40–50 adult patients across a wide range of admission types with an average length of stay of approximately 5 days. Common reasons for admission include fractured femur, distal radius, ankle, osteoarthritis and infection. Patient participants were eligible to take part if they were a patient on the orthopaedic unit within the hospital and met the inclusion criteria listed in Table 1.
Patient participant inclusion criteria.

Patient participants were randomised using online randomizer.org before being screened to determine if they met the inclusion criteria. The clinical research team members (PW, SB, SF) used the inclusion and exclusion criteria to identify eligible patients using electronic medical record software. Eligible participants were approached by a member of the clinical care team (not the research team) to invite their participation in the study. Following this verbal introduction to the study, one of the clinical research team members (PW, SB, SF) provided eligible participants with a study information pack that included the participant information sheet and consent form. If participants provided written consent to participate, an interview was conducted in-person, during their stay on the orthopaedic unit.
Healthcare professional participants were eligible to take part if they were currently employed and working on the orthopaedic unit during the study period. Healthcare professional participants were recruited using convenience sampling in the first instance and then purposeful sampling was applied to ensure that the recruited sample included participants that represented a range of professions involved in pain management including pharmacy, physiotherapy, nursing and medical. All eligible participants were provided with a study information pack including the information sheet and consent form via email from hospital administration staff. Following this, one of the clinical research team members (PW, SB, SF) approached eligible participants to discuss the study and if they provided written consent to participate, an interview was conducted in-person, during their shift on the orthopaedic unit.
Data collection
Semi-structured interviews were conducted in-person in a private room within the orthopaedic unit. An interview guide was developed based on the research aim of exploring patient and healthcare professional perceptions of pain management and the role of opioids. The guide was refined through pilot testing with one pharmacist and one patient. Interview questions explored patient experiences with pain and pain management, perceived risks of pain medicines, their engagement in decision-making and their expectations for pain management (see Appendix 1 for the full interview guide). Interview questions with healthcare professionals explored influences on opioid prescribing and pain management, engagement of patients in decision-making and information provided to patients and community healthcare providers on pain management plans (see Appendix 2 for the full interview guide). Probing questions were asked to facilitate deeper understanding of perspectives and clarify responses. Data adequacy was achieved, as evidenced by later interviews which did not identify new information or themes. Interviews were conducted in-person by one of clinical research team members (PW, SB, SF) and were audio-recorded and transcribed verbatim by a professional transcription service. Basic demographic data (age and sex) was collected from patients who participated in the study. For those who were randomised but not included in the study, reasons for this exclusion were collected. For healthcare professions basic demographic data included profession and sex. As healthcare professions were recruited via email, no data were kept on reasons for not participating in the study.
Data analysis
Analysis of the interview transcripts was informed by a reflexive thematic analysis approach, allowing the research team to explore the complexity of real experiences, needs and priorities of patients and healthcare professionals without being limited by existing theories. This involved following the six steps of reflexive thematic analysis as described by Braun and Clarke.24–27 First, transcripts were read and checked for accuracy by the clinical research team members who collected the data (PW, SB, SF). The analysis team (SCH, JB, and SM) immersed themselves in the data by carefully listening to the recordings and thoroughly reading the transcripts. The analysis team took notes as they familiarised themselves to ensure meaningful engagement with the data. Initial inductive coding was systematically conducted by JB in NVivo 2020 (QSR International Pty Ltd. 2018), where transcripts were coded line by line with regular reflexive meetings with the analysis team. Reflexive memos were maintained throughout to review thoughts about the meaning and content of themes as they developed. The analysis held regular peer debriefing meetings to discuss the coding process and to iteratively refine, merge and consolidate codes into initial themes. Team meetings were held with the analysis team and the clinical research team along with their clinical supervisor (VS) to discuss codes and further develop, define, and refine the themes and consider how our experiences and expectations influenced our interpretations and understanding of the data. Themes were finalised through an iterative re-writing process by SM, JB, SCH with continual checking of transcripts. The final themes were discussed in depth and confirmed with the broader research team. PW, SB, SF maintained interview field notes and JB maintained a reflexive analytic journal throughout this process.
Research rigor
To ensure research rigour, the study adhered to four established criteria: credibility, dependability, confirmability and transferability. 28 Credibility was strengthened through utilizing rigorous methods to collect and analyse the data and being led by researchers with experience and training in undertaking qualitative research. Strategies such as recruiting participants from a range of patients and health-care professions familiar with the context of pain management in an orthopaedic setting and maintaining researcher reflexivity also facilitated rich findings. SM and JB documented personal biases and assumptions in a reflective journal, drawing on their professional backgrounds, SM as a clinical pharmacist and research lead and JB as a medical student to critically engage with the data. A reflexive thematic analysis approach further supported this process, enabling ongoing reflection on the researchers’ roles.
Dependability was achieved through meticulous documentation of the analytic process, including the use of reflexive memos to track evolving interpretations and an audit trail to record decisions about theme development. Confirmability was achieved by utilizing independent interviewers unaffiliated with participants, alongside a collaborative review of all transcripts and codes by the research team to resolve discrepancies and refine interpretive findings.
Findings
Forty participants (20 patients and 20 healthcare professionals) participated in this study between June and October 2020. A total of 147 patients were screened for inclusion in the study. Reasons for exclusion were patient unavailable at the time of screening (e.g. in operating theatre; n = 54, 42%), cognitive impairment (n = 23, 18%) non-English speaking (n = 21, 17%), interviewer unable to complete the interview due to competing clinical demands (n=7, 6%), interviewer was involved in the care of the patient (n = 4, 3%), patient not involved in managing their own medicines (n = 3, 2%), no opioids currently or previously prescribed (n = 2, 2%), opioids prescribed for indication other than pain (i.e. opioid substitution program; n = 1, 1%), visual and or hearing impairment (visual or hearing aids acceptable; n = 1, 1%), did not consent in the timeframe given (n = 1, 1%). Only 10 patients declined participation in the study (8%). Patients that were included in the study had a mean age of 60 years (range 26–83 years), and 45% were female. Interviews lasted an average of 14.28 min (7.47–31.53 min with a median of 12.04 min).
Health professionals that participated in this study included Physician (interns to advanced trainees working in orthopaedics and orthogeriatrics; n = 9), Nurses (enrolled, registered and nurse practitioners; n = 7), Pharmacists (n = 2) and Physiotherapists (n = 2). A total of 70% of health professionals were female, which is reflective of the health care profession.
A total of three themes were identified through the analysis: (1) The patient as an individual; (2) the acute care setting and (3) patient engagement and education. Table 2 outlines the themes and sub-themes identified.
Themes and sub-themes.
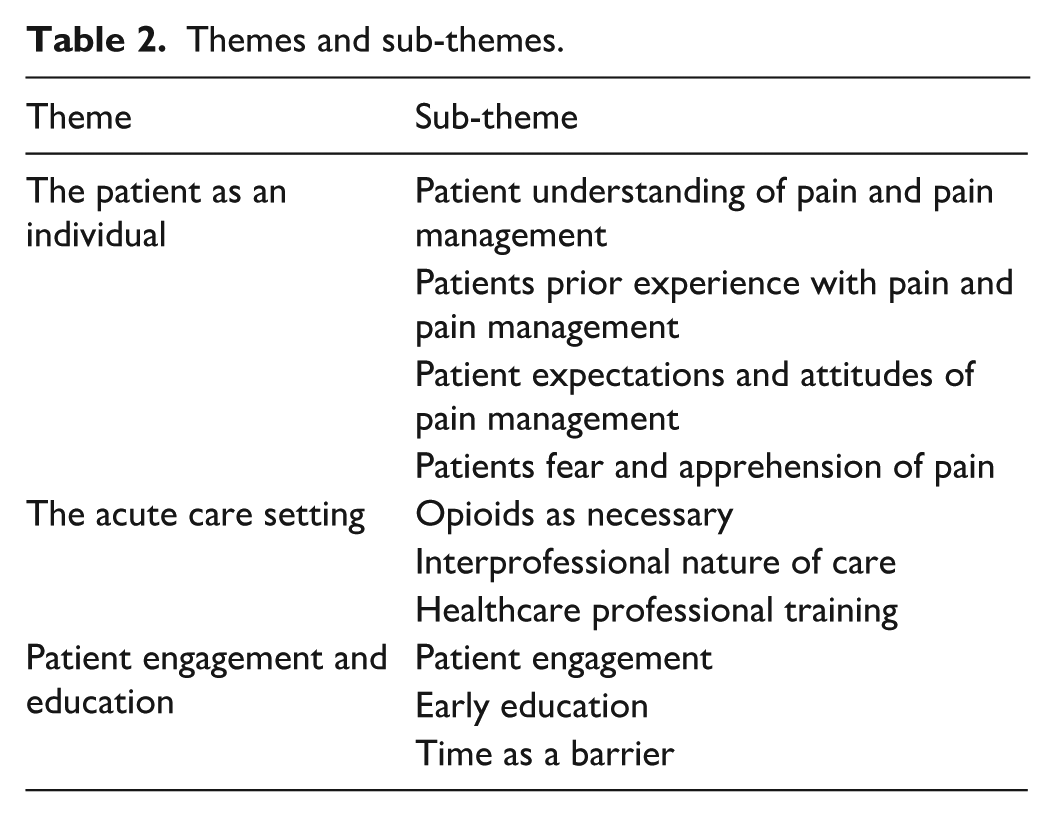
Theme 1 – The patient as an individual
It was clear from both patient and healthcare professional participants that personal experiences and individual factors influenced their understanding of opioids and pain management. We identified four sub-themes or individual factors: those which encompassed a patient’s history and personal journey such as previous pain management, and personal expectations of the risk and effectiveness of different pain management options.
Patient understanding of pain and pain management
Both patient and healthcare professional participants made clear that patients vary significantly in their knowledge about opioids, specifically their side effects, and how often they can be given. Healthcare professional participants described that it is unrealistic for patients to have an understanding: ‘. . .unless they’ve done a pharmacy degree, they’re not going to have a good understanding’ (HP_5). Supporting this notion patient participants did not describe themselves as experts and were happy to delegate decision-making to healthcare professionals: “. . .I’m going, ‘I’m not a pharmacist, I’m not a doctor. I don’t really take a lot of painkillers. I know that I can’t have this and that’” (P_10). Despite this, many patients demonstrated a good understanding of pain and pain management:
When I first got admitted, I was taking two tablets. And then I had a really rough night, so it went up to four. We continued on with the four tablets the following day, and I felt really groggy that day. So I asked to go back to two during the day and then back up to four in the night. So we’re finding that kind of nice balance and they’re [healthcare professionals] pretty good at that as well. (P_14)
Health professionals described ‘language barrier, education level, does affect the general understanding of medications, including the opioids as well’ (HP_1). Patients vary considerably in their education needs based on these individual factors to support good understanding of opioids and pain management strategies.
Patients prior experience with pain and pain management
Interviews with both patients and health professionals demonstrated that patients with chronic conditions or previous experience with opioids may have a better understanding of pain management: ‘In a few weeks, I only want to be on the Panadol. I don’t want any more Endone, I mean, it’s a very, very strong tablet’ (P_06) and ‘I have a simple sort of opinion. I say, sometimes the medication is worse than the disease. To me, they only camouflage the problem, they don’t solve the problem’ (P_07). When discussing patient’s understanding of long-term opioid risks, clinicians noted that those with chronic conditions frequently underestimated the implications: ‘Possibly not because some, [patients] request a lot [of opioids] and we do get a lot of people who've admitted they have had chronic [opioid use], they’re on a lot of medications and whether they understand the implications of all that, I don’t know that they do’ (HP_11). Whilst this history of opioid use enabled good understanding and informed choices around future pain management, in other instances chronic use enable patients to downplay or overlook risks.
Patient expectations and attitudes of pain management
Patients’ expectations ranging from desiring no pain management to seeking complete pain relief, represented another individual factor influencing perceptions of pain and treatment approaches: ‘Some are afraid of getting addicted to it. . . .others, how do I put it? They are asking too much. They expect to be pain free’ (HP_2). Some patients expressed a desire to avoid side effects of opioids, specifically confusion, leading them to avoid or decline the use of opioids: ‘As far as my pain goes, they’re going to give me oxycodone but it’s going to be my last resort. I’m going to. . . you know, in my own surroundings, my own mindset, positive, you know, surroundings at home, do it my way without having to refer to drugs that make you zonk out’ (P_12). Many patients had realistic expectations of pain management to achieve comfort and support movement: ‘As long as it’s dulled [the pain], that’s what I’d be happy with. But if there’s no pain at all, then obviously that’s ideal’ (P_14). Each individual patient bought their own expectations on what pain they should experience and the goals of pain management plans, which health professionals found challenging.
Patients fear and apprehension of pain
Lastly, patients’ fear and anxiety about post-discharge pain emerged as another individual factor shaping perceptions of pain management and opioid use. Some patients described experiencing a lot of pain at home: ‘I feel that I deal with far too much pain on a daily level when I’m at home’ (P_5) and health professionals described it being easier to prescribe opioids pre-emptively to aid in pain management: “In the hospital, if anything happens, the nurses and doctors are there but at home . . . if anything happens, ‘What pain relief am I going to take?’ So, whatever worked in the hospital, it’s easier to [continue the same medicines], [they] know how it works. So, it’s always a good thing to discharge them with some pain relief” (HP_3). Patient comfort and pain management once they get home was a driver for prescription of opioids when patients left hospital.
Theme 2 – The acute care setting
Both patient and healthcare professional participants identified that the acute care setting influences understandings of opioids and pain management. We identified three sub-themes, these included: opioids as necessary, the multiprofessional nature of care, and the need for healthcare professional education and training.
Opioids as necessary
In the acute care setting, healthcare professionals expressed a primary objective of addressing acute pain, particularly for the goal of early mobilisation. Therefore, opioids were considered essential, with few other pain management options, due to their perceived efficacy:
Their ability to get moving is probably the most important thing. To be able to participate in physio and rehab, especially with knee replacements, getting their knees moving as soon as possible. So I will always encourage patients to keep in mind that while they’re resting, if their knee is like a little bit sore, they may still need to take something in light of the fact they’re going to be moved around very soon. (HP_14)
However, patients described rarely being provided with alternative options for pain management, feeling they were often given a standard regimen of pain medicines including opioids: “No, they just say, ‘Endone, Panadol, Panadol, Endone, Endone, Panadol?’ That’s it. That’s all they say” (P_6). Patients identified the value of non-pharmacological strategies for their pain management:
I went to the pain clinic. . .and spent quite a time in there, learning how to control it. It’s the best thing I ever did. They teach you to try and mask out the main part of the pain and think it’s not as bad as it really is. (P_17)
Non-pharmacological strategies were rarely identified by health professional participants and patients shared that these strategies were often learnt by patients outside of the acute care context. Use of the term ‘pain killers’ which came up in many of the interviews could be contributing to unrealistic expectations around the role of pain medicines.
Multiprofessional nature of care
Through the interviews, we identified that the multiprofessional nature of acute care resulted in several barriers to pain management. As all health professionals are responsible for discussing patient preferences and pain management options, when things are busy, it is often missed and assumed someone else will do it:
I would always think or formulate a plan first and then I would escalate it first to acute pain services if I thought that was necessary and then I would always relay that plan back to the patient and see what their thoughts were, but I think often that gets missed when you’re busy sometimes. (HP_10)
Health professionals also dismissed their responsibility attributing other health professionals as more appropriate: ‘I probably don’t do a very good job in terms of educating them; but I think pharmacy probably does a better job of doing that’ (HP_07). However, patient interviews highlighted the consequences of this multiprofessional care:
. . .there are other people when perhaps handover doesn’t happen. I had someone try and give me Endone yesterday and they said, ‘Here’s your painkillers’ and I said, ‘What is it?’ and I’m glad I asked because it was Endone and that would have made me feel quite sick. (P_10)
The multiprofessional nature of acute care also created difficulties in the coordination and timing of administration of pain management. For example, the timing of analgesia dosing prior to physiotherapy sessions, which is critical for managing pain during or after mobilisation. Patients reported an exacerbation in pain when exercising where pain medicines were not administered pre-emptively contributing to a further fear of pain:
The physio give you a half an hour notice but I did not get any notice and they walked through the door and expected me to do some exercises and I said, ‘Well, I haven’t taken my pain killers’. . .the pain then following was excruciating. (P_9)
Lack of a primary person or profession responsible for developing and communicating pain management plans with patients resulted in inconsistencies in how well this was done. The need for professions to work together and co-contribute to pain management plans was apparent. This also left the patient in dark, depriving the on the opportunity to advocate for their pain management needs.
Healthcare professional training
Where opioids are utilised as part of pain management, we identified that education and training of health professionals, especially junior doctors and nurses, may be necessary to support appropriate use of opioids. Specifically, some health professionals raised concerns about the disconnect between prescribing of opioids on discharge and patients’ actual needs based on utilisation in the period leading up to discharge:
I’ve noticed this is more common with interns. . . ‘Oh, the patient has had oxycodone’, so they just put it on their discharge script. And they haven’t checked how much the patient has used in the last 24 h or the last 48 h. (HP_1)
Good training was thought to support better processes by prescribers in choosing pain management that is appropriate to the individual patient and enabled all health care professions to engage with patients in decision-making and educating them to optimise their pain management.
Theme 3 – Patient engagement and education
Both patient and healthcare professional participants described the importance of patient engagement and education for appropriate pain management and opioid use. We identified three sub-themes, these included patient engagement, early education and time as a barrier.
Patient engagement
Both patient and healthcare professional participants described patients as playing a passive role in their pain management. Instead, they relied on healthcare professionals and hospital protocols to manage their pain: ‘They know more than me. All I can know is what I feel right away’ (P_4). This also varied based on the stages of pain, with patients in acute overwhelming pain heavily reliant on health professions to take the lead in providing the care and medication needed as their decision-making was impacted by the acute nature of the pain.
Early education
Health professionals reported that early patient education on pain management, led to realistic expectation of pain management:
I get the opportunity to educate them in advance, to sit down and say to them that it [pain] is subjective. ‘These are the people that you need to talk to about it while you’re here. These are the reasons why. And these may be some of the options that are going to be presented to you’. I think that if they don’t have a little bit of an understanding, at that point, they’re not going to. There are some people that just don’t necessarily take it in, overwhelmed or whatever. But I think overall, my patients probably have a realistic expectation. (HP_14)
As many patients had no prior experience with acute pain or orthopaedic pain requiring opioids, many experienced confusions around the timing of doses and were not provided with appropriate education. During busy periods, requests for opioids were often followed by delayed dosing, resulting in uncomfortable waiting times. These experiences led to a belief that opioids were given by a strict protocol that was not responsive to their individual pain experience:
I would press the button before the hour so that when it got to the hour, they would bring the medication. But I would have the nurses come in and say, ‘You’ve got 3 or 5 min to wait’, and then they would have to come in for me to ask again, and then they would go away again and come back 10 min later, so, then I would be in pain for another 20 min, and then it would take another 10–20 min to kick in, so, it was this revolving door of not having enough pain medication. So, it was a really bad experience the first night I was here because I did not understand the protocols and they did not explain it to me very well. (P_3)
Even patients who did have prior pain management experience also expressed confusion with their pain management plan as it was not explained to them. A critical concern arose when patients were unable to increase dosage amounts or frequency beyond their standard pre-operative opioid regimen:
I was taking regularly two 5 mg oxycodone prior to surgery . . . I made a comment along the lines of, ‘do you reckon this is going to do it? Because I don’t’, and they said, ‘oh, well, you start off with this’, and I said, ‘they must be nuts’. (P_9)
Time as a barrier
Despite recognising the value of early education and patient engagement, time constraints in acute care settings were identified as the primary barrier to delivering timely or comprehensive patient education, limiting opportunities for individuals to actively participate in their pain management plans or address concerns: “Because we’re busy, we just tend to go, ‘Yep, we’ll do it now. We’ll give it to you’, and move on to the next thing. We probably lack a bit about giving them the education they require” (HP_11).
Patients described this lack of education and indicated interest in receiving more information around their pain management:
I would have expected a little bit more information being told to the patient. I like to research. I’ve had a lot of problems with communication within this hospital, and meds was one of them. (P_12)
Patients desire to be able to request medicines when needed for pain, requires a greater understanding on what pain management options are available to them and when and how they are used.
Discussion
Acute post-operative pain is a complex and subjective experience. 16 This study demonstrates the complex factors that influence pain management and opioid perceptions within the orthopaedic context. Health professional and patient experiences found that individual patient factors such as understanding of pain and pain management, prior experiences with pain and pain management, expectations and attitudes of pain, and fear of pain, influenced their understanding and engagement with pain management. This finding builds on research that found that patients undergoing knee arthroplasty often have a preconceived notion about how they would respond to pain.19,20 Our study explored perceptions in a much broader cohort, not focusing on a specific orthopaedic procedure, contributing experiences and perceptions from a broad range of patients with variable past experiences in having pain, and managing that pain.
Our study also identified the unique context of the in-hospital acute care setting, and how this influences pain management and opioid use. We identified that opioids are viewed as critical for managing acute orthopaedic pain, supporting previous research highlighting that opioids are prescribed and administered due to perceptions of the importance of pain control, and the efficacy of opioids. 29 However, we identified that pain and opioid management is poorly managed due to the multiprofessional nature of acute care with many healthcare professionals assuming someone else will take responsibility for engaging patients, supporting previous research. 30
The critical importance of patient engagement and education was the final key theme identified in our study. In general, patients were treated as passive in the pain management process, with very little early education on pain and pain management, despite healthcare professionals identifying the importance of early engagement and education. Overall, lack of time was attributed as the main barrier to appropriately education and engagement patients in the pain management process.
Based on the themes identified in this study, we recommend patient engagement as the key to navigating the acute care setting and individual patient factors. This supports existing endeavours that have sought to navigate barriers around pain, pain management, and opioids, such as opioid stewardship programs. Opioid stewardship programs are an approach that aim to ensure the right medication, for the right patient, at the right time, recognising that one size does not fit all. 31 Whilst much of the efforts have been focused on reducing prescribing, increasingly, a call for more patient perspectives in shared-decision-making has been called for. 31 Figure 1 outlines our perspective on how patient engagement and education is critical to navigating individual patients and the acute care setting when it comes to pain and pain management:

Visual representation of themes identified from the perceptions and experiences of patients and healthcare professionals on the use of opioids.
Individual factors are factors that cannot be changed, and the acute care context is beyond the scope of individual, on the ground healthcare professional’s control. However, patient engagement and education can be addressed and can overcome the difficulties that result from individual factors and the acute care context. When considering these results against the i-PARIHS implementation framework, 32 we can start to see clear strategies to implement to support better pain management.
The i-PARIHS framework outlines that to successfully implement practices to improve patient care, there are four key constructs that need to be considered: (1) the innovation, what you’re trying to achieve (2) the recipients, the people you are asking something of (3) the context, where you are trying to improve practice and (4) facilitation, how you are going to make it happen. 32 In our study, we identified that the innovation, tailored pain management processes, is not currently happening. The recipients, the patients, have various individual factors that cannot be changed, but can be better understood to tailor pain management. We also identified that the context, the acute care and orthopaedic setting, often requires opioid prescribing and interprofessional care. However, through facilitation, patient engagement and education, the innovation of tailored pain management, is possible, with these recipients and in this context.
Therefore, the findings of this study identify that the current pain management approach within orthopaedic settings reflects a fragmented system of care that does not address the complexity or interaction of these factors and ultimately results in a lack of patient-centred care or tailored pain management.
Protocol-driven pain management that does not engage the patient in decision-making about their pain management or provide the necessary education to enable patients to be active decision-makers in their care may be contributing to an overuse of opioids in this patient cohort. Our study supports previous research that highlights that this lack of patient engagement leaves patients feelings disempowered, judged and stigmatised when they seek additional pain management, and ultimately leaves them feeling as though their pain has not been properly managed.33,34 In contrast, active engagement could improve appropriate opioid use and quality of care. 30 It is important to understand what level of engagement the patient would like with decision-making around their medicines, and to work with the patient to develop their pain management plans.30,34,35
This study provides opportunity for further research into the use of opioids for pain management. Based on the results of this study, we recommend that interventions which focus on a patient centric model of care for post-operative pain management and increase patient engagement with decision-making around their care need to be developed. 30 These would aim to place patients at the centre of personalised pain management plans that provide stepwise analgesic options, optimising adjuvant analgesics and non-opioid modalities which may lead to reduced opioid use. This study indicated that many patients wished to be involved in decisions around their pain management. Further research is needed to explore approaches such as co-designed pain management plan where there is early engagement with patients, starting with education prior to elective procedures to develop patient understanding and realistic expectations of the pain management process, opioids and their role. 30 This research should also explore longitudinal evaluation to determine the impact of early education. Additionally, having clearer governance guidelines that support patient engagement with an embedded pain management processes with designated responsibility focussed on patient-centred care could further facilitate expectations and understanding.5,17,30
Barriers to delivery of this model of care include a lack of time available to dedicate to having conversations with patients about their care. 17 Whilst it is vital that all health care providers have necessary training to enable them to have meaningful conversations with patients about pain and pain management, it was clear from our research the importance of having good governance of individual pain management plans, with primary responsibility being assigned to a team member to ensure this occurs. 5
The main strengths of the study come from having a broad scope of patients and healthcare professionals interviewed, providing a spectrum of ideas and perceptions to be explored. Additionally, conducting interviews during patients’ admission, results in a focus on more recent experiences. However, the limitations of this study must be considered. The interview guide was intentionally designed to ask open but direct questions to accommodate participation in the study by patients in pain, and busy health professionals caring for these patients and limit the burden of their participation. We must acknowledge the lens from which these interviews were undertaken. Pharmacists working within the orthopaedic surgical unit conducted the interviews, each bringing their own perspectives and experiences. Opioids are commonly used and their harms are well known to pharmacists who often play an important role in judicious use of opioids in pain management plans. Whilst none of the pharmacists were providing clinical care to any of the patient participants, it is important to recognise the potential for perceived power differentials between patients and health professionals, and how this influenced the responses given. This study may not reflect the full spectrum of patient and health professional experiences and perceptions of the use of opioids in pain management, we sought to understand a specific context in detail rather than include a broader context and perspectives. One theme provided insight into healthcare professional’s perceptions that patients with cognitive impairment or non-English speaking background may have different needs; however, these patients were not included in this study as they were unable to consent and engage in a semi-structured interview. Further studies should explore a more diverse sample including patients with cognitive impairment and non-English speaking patients to better understand the perspectives of this cohort and aid in tailoring implementation to different contexts. Therefore, the research was limited in its insights into the cultural influences on pain and pain management. Further research is required to explore this. Additionally, non-pharmacological strategies were not identified as a strong theme in our study. This may be due to the interview guide not explicitly asking about these strategies. Therefore, future research should further explore opportunities for non-pharmacological strategies in pain management within orthopaedic settings.
What this study does provide is a deeper understanding of the context of patient’s experiences of pain post-operatively and helps to understand what knowledge gaps exist and how patients may be enabled to be drivers of optimal pain management.
Conclusion
In conclusion, this study provides the contextual and recipient factors required to develop improved delivery of care for patients with pain in an orthopaedic setting. Interventions that could be trialled focus on pre-operative communication and counselling; developing a pain management process focussed on patient-centred care embedded within the health care system with clearer guidelines; and identifying the roles and responsibilities of the interprofessional healthcare team in delivery of care.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121251398434 – Supplemental material for Perceptions and experiences of pain management and opioid use among orthopaedic patients and health professionals: Insights from a qualitative study in a metropolitan tertiary hospital
Supplemental material, sj-pdf-1-smo-10.1177_20503121251398434 for Perceptions and experiences of pain management and opioid use among orthopaedic patients and health professionals: Insights from a qualitative study in a metropolitan tertiary hospital by Sally B. Marotti, Jonathan Beacham, Jennifer Collins, Valerie Sim, Peter White, Sonia Bushby, Stephanie Fontanarosa, Lucian Bogdan Solomon and Sarah C. Hunter in SAGE Open Medicine
Footnotes
Appendices
Acknowledgements
We would like to acknowledge Constance Kourbelis for her assistance with coding and thematic analysis of the transcripts.
Author contributions
VS, SBM, PW, SB, SF, and LBS conceived the study and developed the study protocol. PW, SB, SF, and PW collected the data. SBM, JB, and SCH led the data analysis with input and support from VS, PW, SB, and SF. SBM, SCH, JC, and JB drafted the manuscript, and all authors provided edits and feedback. All authors confirmed the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding has been provided by Statewide services – SA Health to fund the pharmacist time in undertaking this project for $19,956. Transcription of interviews was funded by an SA Health allied health seed funding grant of $3000.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.