
Abstract
Objective:
The study aimed to assess the magnitude and predictors of erectile dysfunction at Mettu Karl Comprehensive Specialized Hospital.
Methods:
Male diabetic patients visiting chronic care follow-up at Mettu Karl Comprehensive Specialized Hospital were face-to-face interviewed as part of a retrospective cross-sectional study from April 6, 2022 to May 6, 2022. SPSS version 21 for Windows was used to enter and analyze the data for the descriptive statistics. Following that, a binary logistic regression and a multivariate logistic regression model were used. Based on a p-value of 0.05, variables that had an independent link with sexual dysfunction were found. The adjusted odds ratio and its associated 95% confidence interval were also used to analyze the direction and intensity of the link.
Results:
A total of 307 diabetic men participated in the study, with a mean age of (52.74, 16.16) and a mean duration of (5.94, 2.974). In this study, 252 people (82.1%) experienced erectile dysfunction, with mild, moderate, and severe cases represented by 30%, 38%, and 14.1% of respondents, respectively. There were statistically significant associations between erectile dysfunction and age (adjusted odds ratio: 4.8, 95% confidence interval: 1.27–18.32), type of diabetes (adjusted odds ratio: 5.8, 95% confidence interval: 1.96–17.73), and comorbidities (adjusted odds ratio: 0.32, 95% confidence interval: 0.15–0.71).
Conclusion:
This study showed that the prevalence rate of erectile dysfunction is high in Mettu Karl Comprehensive Specialized Hospital. Age, type of diabetes mellitus, and the presence of comorbidity were factors associated with erectile dysfunction. Therefore, assessment and management of erectile dysfunction in the diabetic clinic should be part of routine medical care during follow-up visits with diabetic patients.
Introduction
Diabetes mellitus (DM), a chronic metabolic disorder marked by hyperglycemia and an estimated 30.3 million people in the United States, or 9.4% of the population, have diabetes. 1
Erectile dysfunction (ED), which can be caused by psychological, neurologic, hormonal, or vascular impairment, is the inability to obtain and sustain an erection strong enough to allow satisfying sexual interaction. 2
Diabetic men have a threefold increased risk of ED compared to nondiabetic men. 3 A number of processes such as endothelial dysfunction, the buildup of advanced glycation end products, oxidative stress, autonomic neuropathy, and inflammation of the prostate are involved in the pathogenesis of ED in diabetes.4,5 Furthermore, hyperhomocysteinemia (HHcys) is a strong and independent predictor of atherosclerosis progression as well as impaired cavernosal perfusion, which leads to ED. 6
Various studies have indicated a wide range of ED prevalence rates among diabetic males. According to this research, the prevalence of diabetic men is between 35% and 75%, compared to 26% in the overall population. 7
Age-related neuropathy, vascular insufficiency, poor glycemic management, hypertension, low testosterone levels, and lifestyle variables such as smoking, drinking, and inactivity are the main risk factors for ED in diabetics.3,8
The most prevalent psychological issue in the world, ED can cause sadness, social isolation, confidence loss, and self-esteem loss. 9 In addition, it has a considerable negative impact on life quality and marital and marital relationship dissatisfaction. 10 However, some of these detrimental effects can be minimized with good illness management. For instance, multiple studies have revealed that roughly one-third of men with ED experience improved sexual function as a result of lifestyle therapies such as counseling, quitting smoking, weight loss, nutrition, and exercise, as well as optimal glycemic control through diet. 4 Unless the patient is expressly questioned about potential symptoms by the healthcare professional, ED in diabetic individuals is frequently left untreated.
As the number of people with DM rises, there has been less research conducted in Africa and Ethiopia on the prevalence of ED. Therefore, the purpose of this study was to describe the incidence of ED and its contributing factors in diabetes patients who were being followed up at Mettu Karl Comprehensive Specialized Hospital (MKCSH).
Patients and methods
Study area, design, and period
From April 6, 2022 to May 6, 2022, a cross-sectional study was done to interview and evaluate medical records regarding sexual dysfunction among diabetes patients. The Mettu Karl Compressive Specialized Hospital, Mettu Town, and Oromia Region served as the study’s locations. The hospital only offers one clinic for diabetic care.
Study participants and eligibility criteria
Incomplete medical records, critically ill patients with diabetic ketoacidosis or hyperosmolar hyperglycemic state, confused, or in septicemia as in an infected diabetic foot were excluded. Male diabetic patients at MKCSH with age 18 years, duration of diabetes 1 year, and willingness to participate were included. A total of 307 diabetic mellitus patients were included using a conscequative sampling technique by considering the magnitude of the ED from the previous study which was 60.4%. 11
Data collection process and management
The data was gathered using a semi-structured data gathering method. A clinical pharmacist was appointed to oversee the data gathering procedure while two nurses, one medical doctor, and one other person were hired for the task. Prior to conducting regular data gathering, the data collecting tool underwent pretesting at the adjacent Bedele General Hospital to ensure consistency. According to the STROCSS (Strengthening of the Reporting of Cohort Studies in Surgery) guidelines, the work has been reported. 12 To ensure the consistency of the data, 5% of the questionnaire was pretested.
Statistical analysis
The data were entered into a computer using EPI-data version 3.1. The principal investigators had daily checked and cleaned the data. The data were then exported to Statistical Package for Social Sciences (SPSS) 24.0 for analysis . Multivariable logistic regression was used to analyze the variable by using crude odds ratio and adjusted odds ratio (AOR) with 95% confidence interval (CI). All variables associated with the ED at a p-value ⩽0.25 on the bivariate analysis were entered into a multivariable logistic regression analysis to control for confounders. Finally, the predictors of ED were declared if a p-value was ⩽0.05.
Ethics approval and consent-to-participate
The Mettu University’s Research Ethics Review Committee (RERC), with reference number MEU/CHS/RERC101/2022, granted ethical permission. Written informed consent was obtained from patients. For subjects with no formal education, written consent was taken from their legally authorized representatives. The study protocol was carried out in conformity with the Helsinki Declaration. With the unique reference number “researchregistry 8096,” the study was registered on researchregistry.com.
Operational definitions
• ED: Explained by a total score of ⩽21 from 5 items of ED questionnaire. 11
• Sever ED: International Index Erectile Function (IIEF) scoring less than 1–7.
• Moderate ED: IIEF scoring between 8 and 11.
• Mild ED: IIEF scoring above 12–21.
• Comorbid illness: Existence of additional chronic illnesses, including hypertension, cardiac disease, dyslipidemia, psychosis, renal disease, HIV, cancer, asthma, and multiple sclerosis.
• Poor glycemic control: Current fasting blood glucose level greater than 130 mg/dl.
• Physical activity: Patients with diabetes who participated in at least 30 min of physical activity daily or participated in a specific exercise session were considered to have adequate physical activity; otherwise, the patient was classified as having inadequate physical activity.
• Social drug use: The lifestyle of the patients was assessed during the patient interview. If the patients responded “Yes” to the smoking cigarette, drinking alcohol and chewing a khat, the patients were recorded as smoker, alcohol drinker, and khat chewer, respectively.
Results
Sociodemographic characteristics of male diabetic patients
Of the study participants about two-thirds 214 (69.5%) of them were greater than 45 years and about half 154 (50.2%) of them were from rural areas. Regarding their marital status about two-thirds 200 (65.5%) of them were married. About one-third 104 (33.9%) of them were college and above by their educational level. In relation to their occupation, about one-fourth 77 (25.1%) of them were farmer and government employee, respectively (Table 1).
Sociodemographic characteristics of male DM patients attending MKCSH from April 6, 2022 to May 6, 2022.

Others include daily labor and housewife.
Clinical characteristics of male diabetic patients
Among the study partcipants, 257 (83.7%) have normal Body Mass Index (BMI) index whereas 250 (81.4%) of them were patients with type 2 DM. Regarding their medications, about two-thirds, 199 (64.8%) of them were on insulin injection. Of the diabetic patients, about two-thirds, 194 (63.3%) of them had good glycemic control. The presence of a comorbidity was reported among 205 (66.8%) patients (Table 2).
Clinical characteristics of male DM patients.

Others include arrhythmia and epilepsy.
Social drug use and lifestyle characteristics of the DM patients
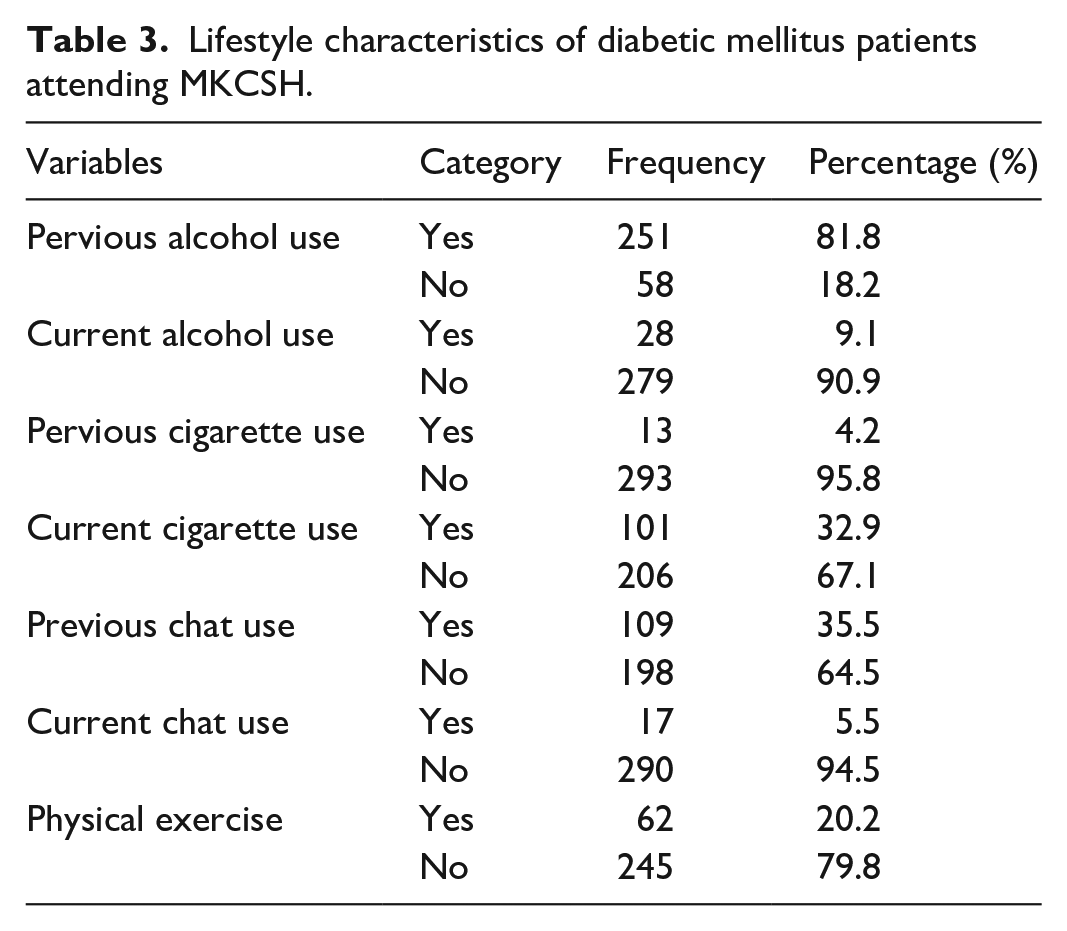
Among the participants, 279 (90.9%) were never-drink-alcohol currently and, about one-third of them, 101 (32.9%) were currently a smoker, and 17 (5.5%) of them were chat chewert (Table 3). Regarding to their physical exercise, about three-fourths of them were physically inactive 245 (79.8%).
Lifestyle characteristics of diabetic mellitus patients attending MKCSH.
Prevalence of ED among male diabetic patients
From the total of study participants, 252 (82.1%) were found to have had the ED and 55 (17.9%) are not. In relation to their severity, 92 (30%) were in mild state, 118 (38.4%) were in moderate, and 43 (14.6%) were in severe ED. About half of them, 148 (48.2%) had difficulties of penetration after erection of their penis and about 122 (39.7%) of them were never satisfied with sexual intercourse (Table 4).
The ED characteristics among male diabetic patients attending MKCSH.

The predictors of ED among male diabetic patients
In binary logistic regression analysis, variables like penis injury, physical exercise, area of the residence, presence of diabetic complication, smoking cigarettes were not entered to multivariable logistic regression analysis because their p-values are greater than 0.25. The results of multivariable logistic regression analysis revealed that patients whose age was >40 years was 4.8 times more likely to have ED than age <40 years (AOR: 4.8 (1.27–18.32), 95% CI, p = 0.023). Similarly patients who had a type 2 DM were 5.8 more likely to develop ED (AOR: 5.8 (1.96–17.73), 95% CI, p = 0.001). Finally diabetic male patients that had two or more disease were two times more riskier to have had ED than who did not have (AOR: 3.425 (1.608–7.295), 95% CI, p = 0.001) (Table 5).
Binary and multivariable logistic regression analysis showing the factors associated with ED among patients of diabetic mellitus in MKCSH, 2022.
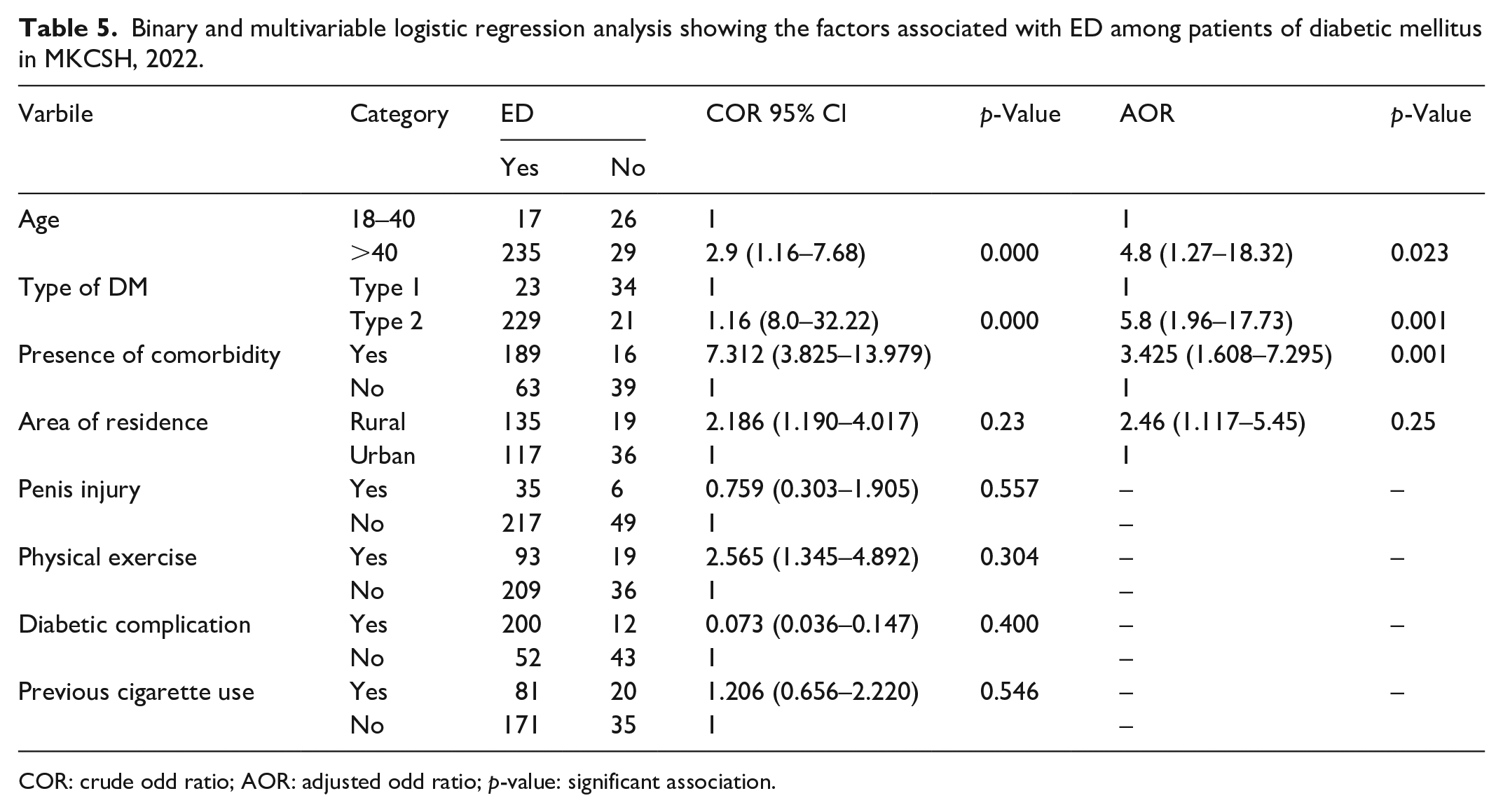
COR: crude odd ratio; AOR: adjusted odd ratio; p-value: significant association.
Discussion
The study revealed that the prevalence of sexual dysfunction among DM patients was 82.1%. This was higher than previous studies done in Jamaica (64%), 13 the Northwest Amhara region (69.5%), Dessie (58.5%), and Jimma (60.4%).11,14,15 This may be due to variation in study period, study method, lifestyle, and sociodemographic characteristics of the participants.
The results of the current study show that age was significantly associated with sexual dysfunction; 4.8 times more likely than those under 40 to have sexual dysfunction (AOR: 4.8 (1.27–18.32), 95% CI). This is in line with studies done in Tanzania, Jamaica, and Southeast Ethiopia.16–18
This can be explained by age-related physiological changes in the testicles and declining sex hormones in older men. Among diabetic patients, indeed, as age increases, the risk of developing peripheral neuropathy, hypertension, and impotency would also increase, which might be the reason for the increased odds of ED.
The current study shows that patients having a comorbidity were three times more likely to develop ED (AOR: 3.425 (1.608–7.295), 95% Cl) than their counterparts. The finding was congruent with the study of Jimma, Jamaica, and Tanzania that showed patients with other concomitant medical conditions increase the risk of developing ED.11,13,16
This might be because different comorbid illnesses could solely alter the sexual function of individuals, for instance, renal disease results in significant endocrine disturbances, including hypo-gonadsim due to reduced renal clearance, the drugs used to manage those comorbid illnesses have a proven side effect on sexual function, for instance, antihypertensive drugs reduce blood flow to the reproductive organs of men that ultimately affects the penile erection capacity and the psychological impact of having a chronic illness.
The current study shows that with reference to Type 1 Diabetes Miletus, the odds of sexual dysfunction among Type 2 Diabetes Miletus patients were 5.8 times higher (AOR: 5.8 (1.946–17.73)). This finding is in line with a study conducted in Tanzania, Jamaica, and southwestern Ethiopia.16–18 As ED and type II diabetes share similar risk factors like aging, obesity, and high blood pressure, ED might be a common clinical entity among type II diabetes patients, which could explain the observed variation. Regarding surgical therapy, inflatable penile prosthesis placement, scratch technique, and postoperative vacuum therapy are as a combined approach to definitive treatment of ED. 19
Strength and limitation of the study
As the strength, the social drug use was assessed and, as the limitation, Fasting blood sugar (FBS) was used instead of HbAIC to assess the glycemic control.
Conclusion
This study showed that the magnitude of ED is found to be high; majority of DM patients experienced moderate ED. Age, type of DM, and the presence of the comorbidity were factors associated with ED. Therefore, assessment and management of ED in the diabetic clinic should be part of routine medical care during follow-up visits with diabetic patients. Besides this, health-care providers should emphasize on screening and treating older patients, type 2 DM patients, and patients presented with a concomitant disease like hypertension and renal disease.
Research Data
sj-docx-1-smo-10.1177_20503121221141803 – for Men’s sexual desire, and why women often don’t recognize it? Prevalence of erectile dysfunction and associated factors among diabetes mellitus patients attending Mettu Karl Comprehensive Specialized Hospital: A cross-sectional study
sj-docx-1-smo-10.1177_20503121221141803 for Men’s sexual desire, and why women often don’t recognize it? Prevalence of erectile dysfunction and associated factors among diabetes mellitus patients attending Mettu Karl Comprehensive Specialized Hospital: A cross-sectional study by Firomsa Bekele, Lelise Fantahun, Bayisa Garbessa and Fili Dekosa in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221141803 – Supplemental material for Men’s sexual desire, and why women often don’t recognize it? Prevalence of erectile dysfunction and associated factors among diabetes mellitus patients attending Mettu Karl Comprehensive Specialized Hospital: A cross-sectional study
Supplemental material, sj-docx-2-smo-10.1177_20503121221141803 for Men’s sexual desire, and why women often don’t recognize it? Prevalence of erectile dysfunction and associated factors among diabetes mellitus patients attending Mettu Karl Comprehensive Specialized Hospital: A cross-sectional study by Firomsa Bekele, Lelise Fantahun, Bayisa Garbessa and Fili Dekosa in SAGE Open Medicine
Footnotes
Acknowledgements
We thank Mattu University for providing the chance to conduct this study. Lastly, we acknowledge the hospital administrators, data collectors, and study participants for extending their helpful hands toward our study.
Author contributions
FB contributes in the preparation of proposal, methodology, and statistical analysis. LF was participated in preparing the first draft of the manuscript. BG and FD contributed to the editing of the manuscript. All authors checked and confirmed the final version of the manuscript.
Availability of data and materials
The materials used while conducting this study are obtained from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was obtained from the Mattu University’s Research Ethics Review Committee (RERC), with reference number MEU/CHS/RERC101/2022. The participants’ parents provided their parents with written, fully informed consent. The study protocol was carried out in conformity with the Helsinki Declaration.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Informed consent
Written informed consent was obtained from patients. For subjects with no formal education, written consent was taken from their legally authorized representatives.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.