
Abstract
Objective:
Drug–drug interactions are of major concern due to links to untoward drug effects, hospitalizations, and serious health impacts. Elderly patients are more predisposed to drug interactions than younger patients. The present study aimed to find out the prevalence of drug–drug interactions at North West Ethiopian compressive specialized hospitals’ Internal Medicine wards.
Methods:
From 30 April to 30 July 2021 GC, a multicenter prospective observational study was conducted at north Ethiopian specialized hospitals. Data was collected by using a structured questionnaire adapted from different literature and medical records at the North West Ethiopian Comprehensive Specialized Hospitals’ Internal Medicine wards during the study period. Thereafter checked the completeness of the collected data was checked drug–drug interactions by using Medscape. Epi data version 4.6.2 software was used as data clearance and STATA version 14.1 was used for further data analysis.
Result:
A total of 389 subjects participated in the study of which more than half (55.53%) of them were female with a mean (SD) age of 68.9 ± 7.46 years. A total of 641 drug–drug interactions were detected in this investigation of which, 225(35.1%) were major, 299(46.6%) were significant interactions, and 117(18.3%) were minor interactions. Hospital stay (AOR = 5.95 CI: 3.49–10.12), retire (AOR = 6.71 CI: 1.26–35.78), 5–9 drugs (AOR = 5.30 CI: 2.91–9.67) and more than 10 drugs (AOR = 8.03 CI: 2.47–26.07) were important risk factors for drug–drug interactions.
Conclusion:
The findings of this study suggest that drug–drug interactions were high among hospitalized elderly patients. The presence of polypharmacy, to be retired, and hospital stayed were all found to be strongly linked with drug–drug interactions.
Introduction
Interactions between prescribed medications are a bigger and more serious health problem that the healthcare industry is grappling with. When the effect of one drug is altered by a co-administered drug, undesirable side effects might occur as a result of synergistic, additive, or antagonistic actions. When two drugs are given simultaneously, they have the potential to interact.1,2 DDIs are a form of adverse drug event (ADE) that occurs when one drug’s effect is influenced by another drug due to polypharmacy. It usually results in a qualitative or quantitative shift in pharmacological activity.2,3
Pharmacokinetic and pharmacodynamic drug interactions are the two major forms of DDIs. Kinetic drug interactions affect the drug’s absorption, distribution, metabolism, and excretion, whereas dynamic interactions affect the drug’s physiological and therapeutic effects when drugs are given concomitantly.1,4 On the other hand, when chemically incompatible medications are mixed outside of the body, such as phenobarbital and opioid analgesics in the same syringe, the condition pertains to pharmaceutical drug interaction. 1
Although taking many medications at the same time can improve therapeutic effectiveness, some combinations can cause harmful untoward effects. 1 The negative effects of DDIs might be induced by an increase in the drug’s toxicity or a decrease in its efficacy. However, drug interactions do not always have negative repercussions; in certain situations, they might even result in beneficial effects in the case of synergism, addition, and potentiating effects.4,5
Due to the lack of new clinical signs and symptoms, plus the fact that most interactions worsen existing problems, most interactions go unreported by clinicians. 5 Besides, due to a lack of information and training, as well as a lack of drive and a poor attitude, DDIs can go undetected. Different factors, such as the use of any concomitant medications, the existence of comorbidity, and advanced age, can all influence the likelihood of developing DDIs. 6
Elderly patients are more predisposed to drug interactions than younger patients, due to age-related physiologic changes, an increased risk for the burden of patients with multiple disease states associated with aging, and the increase in medication use,7,8 and consequently increased prevalence of associated morbidity and mortality. Along with age-related gradual changes, the pharmacodynamics and pharmacokinetics of drugs in the elderly are altered. These changes affect how medicines are handled, including alterations in drug absorption, volumes of distribution, metabolism, and clearance, which can make longer half-life, augment the potential for drug toxicity, and the possibility of ADRs because of a failure to maintain homeostasis under conditions of physiological stress.9,10
Drug interactions are a considerable cause of doses too low, doses too high, ADR and hospital admission, and increased poor treatment outcomes and health costs. DDI-related ADRs in the elderly have been 4.5%–6.5%; 11 approximately 0.05% of the emergency department visits, 0.6% of hospital admissions, and 0.1% of the re-hospitalizations are caused by ADRs due to DDIs. 12 Prudent drug selection assisted by a clinical pharmacist is needed to reduce irrational polypharmacy and minimize the risk of DDIs.
Although the involvement of many practitioners in patient care enhances treatment quality through collaboration, multiple separate prescriptions increase the likelihood of unsuitable drug combinations. 13 There is a dearth of knowledge regarding drug interactions in Ethiopian clinical settings among the elderly. Therefore, studies on DDIs have never been conducted in northwest Ethiopia in comprehensive specialized hospitals, including Debre Tabor Comprehensive Specialized Hospital (DTCSH), University of Gondar Comprehensive Specialized Hospital (UoGCSH), Felege Hiwot Comprehensive Specialized Hospital (FHCSH), Tibebe Ghion Comprehensive Specialized Hospital (TGCSH), and Debre Markos Comprehensive Specialized Hospitals (DMCSH). It is reasonable to assume that DDIs will be common in the inpatient settings, especially in the internal medicine ward, where the majority of patients with a variety of disease conditions are admitted. Therefore, the purpose of this study was to determine the frequency of DDIs in the internal medicine wards of northwest Ethiopia’s comprehensive specialized hospitals.
Methods
Study setting and period
The study was conducted at northwest Ethiopia’s comprehensive specialized hospitals; DTCSH, UoGCSH, FHCSH, TGCSH, and DMCSH from 30 April 2021 to 30 July 2021.
University of Gondar hospital is found in Gondar town, which is located 727 km from the capital city of the country, Addis Ababa. Currently, the hospital serves around seven million people, both outpatients and inpatients. The medical ward serves an average of 210 patients per month, with an estimated 25%–35% of them being elderly.
Debre Tabor hospital is located in Debre Tabor town, the capital city of the South Gondar Zone. It was about 666 km from Addis Ababa. The hospital has served more than three million people, both outpatients and inpatients. The medical ward serves around 180 patients per month with an estimated 25%–35% of them being elderly.
Felege Hiwot and Tibebe Ghion hospitals are found in the capital city of Amhara regional state, Bahir Dar, which is 565 km away from the capital city of Ethiopia, Addis Ababa. The hospital provides different clinical services for 7 million people in the catchment area. The medical ward serves an average of 225 patients per month. Of those, an estimated 25%–35% are elderly. Tibebe Ghion hospital serves more than seven million people in the catchment area. The ward has served an average of 160 per month from those 25%–35% of them being elderly.
Debre Markos hospital is located in East Gojjam, which is located 300 km and 265 km from Addis Ababa and Bahar Dar, the capitals of Ethiopia and the Amhara regional state, respectively. The hospital has served more than 3.5 million people, both outpatients, and inpatients. The medical ward serves 190 patients per month, of which an estimated 25%–35% are elderly.
Study design
A multicenter prospective observational study was conducted through patient interviews and medical chart reviews at UoGCSH, DTCSH, FHCSH, TGCSH, and DMCSH.
Population
All patients aged 60 and up were admitted to the medical wards of the comprehensive specialized hospitals in Northwest Ethiopia.
Study population
All elderly patients aged 60 years and above were admitted to the medical ward of the northwest Ethiopian comprehensive specialized hospital during the data collection period.
Inclusion criteria and exclusion criteria
Inclusion criteria
Patients of age 60 years and above who were admitted to the medical ward took at least two medications and could participate in the study.
Exclusion criteria
Those who have incompletely documented data, patients with hearing and speaking problems, patients who were discharged before the collected data were cross-checked, and patients who came for the procedure only.
Sample size and sampling technique
The number of patients to be involved in the study was determined by using the single population proportion formula:

Where:
Based on a cross-sectional study at Ayder Referral Hospital, Northern Ethiopia, the prevalence of DDIs was 62.2%. Therefore, the p value was 0.622. Zα/2 = 1.96 and d = 0.05
As a result, N = 361
After adding a 10% contingency for non-respondents and patients who refused to participate in the study, provided the sample size was 397. Final analysis was performed on 389 individuals after eight patients were eliminated from the study (three very ill, three unwilling to participate, and two discharged before cross-check).
There are five comprehensive specialized hospitals in Northwest Ethiopia. The sample was allocated based on the patients’ flow and the bed number of the hospital. Proportional allocation was used to select study subjects based on the number of patients that the respective hospitals contained in their medical wards.
The source population and the samples were N = 888 and n = 389, respectively.
The interval size “K”
K = N/n = 888/389 = 2.28 ~ 2
Sample of each hospital = patient follow each hospital ward*sample size/source of population.
UGCSH = 196*389/888 = 85.86~86
DTCSH = 167*389/888 = 73
FHCSH = 209*389/888 = 91.56~92
TGCSH = 145*389/888 = 63
DMCSH = 171*389/888 = 74.9~75
Systematic random sampling was used to select the study participants until the required sample was reached between April 30, 2021 and July 30, 2021. The first patient was selected randomly, and then every other patient was selected from the patient registration list until the required sample was reached.
Variables of the study
Dependent variable
Drug–drug interaction among elderly patients.
Independent variables
Socio-demographic variables (age, sex, education status, marital status, religion, occupational status, and place of residence).
BMI, and GFR.
Source of drug.
Social drug use (alcohol, khat, and smoking).
Class and number of prescribed drugs.
Class of medical condition.
Number of comorbidities.
Length of hospitalization.
Data collection process and management
The data were collected by using a structured questionnaire adapted from different literature and medical records.12,14–16 The data collectors were five clinical pharmacists (B.Pharm), and the supervisors were four senior clinical pharmacists (two MSC and two B.Pharm). The principal investigator and supervisors checked the collected data for completeness during data collection.
Medscape was used to check DDIs. A pretest was done on 20 patients before the actual data collection, and some modification (e.g., income) was considered based on the result of the pretest.
Data quality assurance
The data collection tool was assessed by two senior clinical pharmacists who are academicians and researchers for face validity, completeness, clarity of its contents, and approval was obtained. The data collectors and supervisors were trained for two days regarding the technique and data collection process before starting data collection. A pretest was done on 20 patients who were admitted to TGCSH before the actual data collection and some modification was considered based on the result of the pretest. Frequent and timely supervision of data collectors was undertaken by the supervisors and principal investigator. The data collectors were five clinical pharmacists (B.Pharm), and the supervisors were four senior clinical pharmacists (two MSc and two B.Pharm). The principal investigator and supervisors checked the collected data for completeness during data collection.
Statistical analysis
The data was cleaned, coded, and entered into Epidata version 4.6.2 software before being exported to STATA version 14.1 for further analysis. Categorical variables were described by frequencies and percentages, and continuous variables were described by mean, standard deviation, and median after checking the normality of the data. Data were expressed in the form of tables, graphs, charts, and texts described based on the characteristics of the data. Binary logistic regression was conducted for each independent variable with the dependent variable as a candidate for multivariable analysis. Variables that passed bivariable logistic regression at 95% confidence intervals with a p value of less than 0.25 were selected for multivariable logistic regression constructed to investigate the associations between these variables and the presence of DDIs. Those variables with a p value < 0.05 were considered statistically significant in the multivariate analysis. Final results were reported as odds ratios (ORs) with 95% confidence intervals for each variable, along with the corresponding p value to show the strength of association. Final results were reported as odds ratios (ORs) with 95% CIs.
Operational definitions
Result
The flow of study participants
Between April 30 and July 30, 2021, 398 patients who met the previously described inclusion criteria were selected by systematic random sampling after providing consent. Of them, 389 (97.74%) completed the study and participated in the final analysis. Consequently, a 2.26% attrition rate was found (Figure 1).

Flow diagram of elderly patients admitted to the medical ward of UoGCSH, DTCSH, FHCSH, TGCSH, and DMCSH, Northwest, Ethiopia.
Socio-demographic characteristics
From the total of 389 study participants, more than half (55.53%) of the patients were female. The mean (SD) age of the study participants was 68.9 ± 7.46 years. Around half (53.98%) of the patients were married. Nearly two-thirds (67.9%) of the patients were farmers and came from rural areas 69.15% (Table 1).
Socio-demographic characteristics of elderly patients admitted to the medical ward of UoGCSH, DTCSH, FHCSH, TGCSH, and DMCSH, Northwest, Ethiopia, 2021 (n = 389).

UoGCSH: University of Gondar Comprehensive Specialized Hospital; DTCSH: Debre Tabor Comprehensive Specialized Hospital; FHCSH: Felege Hiwot Comprehensive Specialized Hospital; TGCSH: Tibebe Ghion Comprehensive Specialized Hospital; DMCSH: Debre Markos Comprehensive Specialized Hospitals; LOH: length of hospitalization; GFR: glomerular filtration rate; BMI: body mass index.
Disease characteristics
From the study period, the most common encountered disease was circulatory 65.8%, followed by respiratory 48.3%, infection and parasite 26.7%, and digestive system 19% (Table 2).
Diagnosis of elderly patients admitted to the medical ward of UoGCSH, DTCSH, FHCSH, TGCSH, and DMCSH, Northwest, Ethiopia, 2021.

UoGCSH: University of Gondar Comprehensive Specialized Hospital; DTCSH: Debre Tabor Comprehensive Specialized Hospital; FHCSH: Felege Hiwot Comprehensive Specialized Hospital; TGCSH: Tibebe Ghion Comprehensive Specialized Hospital; DMCSH: Debre Markos Comprehensive Specialized Hospitals; ICD-10: International Classification of Diseases, tenth edition.
The pattern of drug use
In the study period from eligible 389 patients, 2191 medications were used, with the average number of drugs per patient being 5.63 (5.39–5.87). The most prescribed medications were antibiotics 256 (65.81%), diuretics 164 (42.16%), anticoagulant 134 (34.45%), analgesic115 (29.56%), and statins 107(27.51%) (Table 3).
Medications pattern of elderly patients admitted with UoGCSH, DTCSH, FHCSH, TGCSH, and DMCSH, Northwest, Ethiopia, 2021.

UoGCSH: University of Gondar Comprehensive Specialized Hospital; DTCSH: Debre Tabor Comprehensive Specialized Hospital; FHCSH: Felege Hiwot Comprehensive Specialized Hospital; TGCSH: Tibebe Ghion Comprehensive Specialized Hospital; DMCSH: Debre Markos Comprehensive Specialized Hospitals.
Others*: antifungal (2), phosphodiesterase (2), hemophilia (1), antidepressant (3), tetanus hemoglobin (3), anthelmintics (6), antiviral (5), a vasodilator (7), antithyroid (7).
Drug–drug interaction
There were 641 DDIs discovered in this investigation. Among these, 225 (35.1%) were major DDI, 299 (46.6%) were significant interactions and 117 (18.3%) of minor interactions. A total of 226 (58.10%) of patients who had faced DDIs, with 53 (23.45%) having one, 61 (26.99%) having two, 44 (19.47%) having three, 32 (14.16%) having four, 17 (7.52%) having five, 15 (6.64%) having six, 1 (0.44%) having seven, and 3 (1.33%) having eight. From this study 134 (59.8%) patients had major interaction, 198 (88.4%) patients had significant interaction, and 70 (30.4%) had minor interaction (Figure 2).

Level of drug–drug interactions identified from elder patients admitted at North West Ethiopia Comprehensive Specialized Hospitals.
Individual drug–drug interactions
In this study, 641 DDIs were assessed. The most prevalence DDIs were ceftriaxone + heparin, digoxin + furosemide, ceftriaxone + furosemide, and spironolactone + warfarin (Table 4).
Severity and mechanism of drug–drug interaction identified from elder patients admitted at North West Ethiopia Comprehensive Specialized Hospitals.
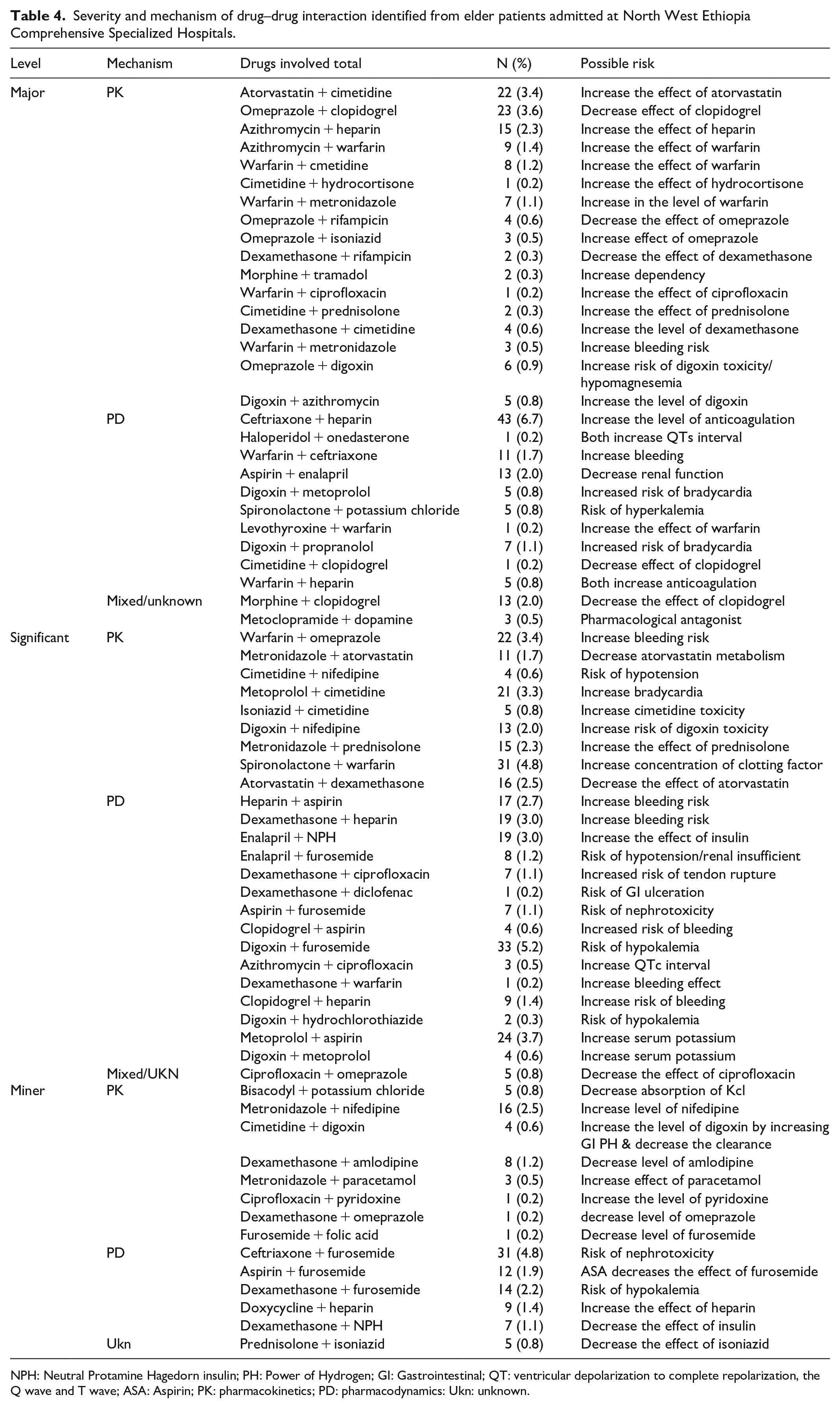
NPH: Neutral Protamine Hagedorn insulin; PH: Power of Hydrogen; GI: Gastrointestinal; QT: ventricular depolarization to complete repolarization, the Q wave and T wave; ASA: Aspirin; PK: pharmacokinetics; PD: pharmacodynamics: Ukn: unknown.
Factors for the occurrence of DDIs
Generally recognized from socio-demographic and clinical factors variables with a p value of < 0.25 in the bivariable logistic regression analysis were further analyzed by multivariable logistic regression. Sex, age, marital status, occupational status, number of diseases, number of drugs, and length of hospitalization have fulfilled the criteria for multivariable binary logistic regression. Factors significantly associated with the occurrence of DDIs in the logistic regression analysis were occupational status with retirement, number of comorbidities, number of drugs, and length of hospitalization.
According to multivariable logistic analysis, patients who were on occupational status with retirement had (AOR = 6.71 CI: 1.26–35.78) times more likely to develop DDIs when compared with those employed. Patients who stayed seven and more days at the hospital had increased the probability of developing DDIs by the odds of 5.95 (AOR = 5.95 CI: 3.49–10.12) times as compared to less than seven days. The odds of DDIs were 5.30 (AOR = 5.30 CI: 2.91–9.67) times higher among patients who took an average of five to nine drugs, and in patients who took more than 10 drugs, the odds of DDIs were 8.03 (AOR = 8.03 CI: 2.47–26.07) times more likely to develop DDI compared to patients who took less than five drugs (Table 5).
Bivariable and Multivariable logistic regression analysis results of factors associated with DDIs among elderly patients admitted to the medical ward of UoGCSH, DTCSH, FHCSH, TGCSH, and DMCSH, Northwest, Ethiopia, 2021.

DDI: drug–drug interactions; UoGCSH: University of Gondar Comprehensive Specialized Hospital; DTCSH: Debre Tabor Comprehensive Specialized Hospital; FHCSH: Felege Hiwot Comprehensive Specialized Hospital; TGCSH: Tibebe Ghion Comprehensive Specialized Hospital; DMCSH: Debre Markos Comprehensive Specialized Hospitals; LOH: length of hospitalization; COR: crude odd ratio; CI: confidence interval; AOR: adjusted odd ratio.
p value < 0.05,
Bold indicates a values which are significant associate with DDIs.
Discussion
Comorbidities are common among elderly individuals, leading to the prescription of many drugs. Multiple medication use may raise the risk of DDIs. 18 Other physiological alterations in the body increase the likelihood of developing DDIs in the elderly. 19 In light of this, the current study was conducted to evaluate the DDIs. Ceftriaxone, heparin, furosemide, warfarin, omeprazole, atorvastatin, and cimetidine in combination with each other or with other medicines were the most commonly noticed DDIs.
The mean number of medications prescribed in this study was 5.6, which is comparable to data from earlier studies in Northern Ethiopia (6 drugs per patient) and Taiwan (5.8 drugs per patient).15,20 The current mean number of drugs prescribed per patient was higher than data from previous studies in southern Brazil (4.4 drugs per patient), Gujarat, India (4.3 drugs per patient), and Germany (3.7 drugs per patient),2,21,22 but lower than data from India (9.2 drugs per patient), South Africa (7.7 drugs per patient), and Puducherry (7.6 drugs per patient).23–25 The greatest number of medications prescribed per patient was 11, which is close to the findings of similar studies conducted in Nigeria and southern Brazil, which found that the maximum number of medications prescribed per patient was 8 and 11 correspondingly.2,26 Various variations could be attributable to changes in study design, health insurance policies, comorbidity load, and medication usage patterns in these locations.
In the literature, there is no single definition of polypharmacy. Many authors describe “polypharmacy” as excessive and unnecessary drug use, while others define it as the number of medications prescribed.27,28 Polypharmacy (prescription of 5–9 medicines) was found in 214 (55.01%) patients, whereas hyper polypharmacy (prescription of ⩾10 medicines) was found in 36 (9.25%) patients. Polypharmacy was found to be more common in this study (55.01%) than in studies conducted in Gujarat, India (22.93%) and southern Brazil (43.1%).2,21 In Japan and India, polypharmacy was shown to be more common, with rates of 80.7% and 66.2%, respectively, compared to the current study.29,30
The prevalence of DDIs in this study was 58.10%, which is greater than.21,23 This is because of the prescriber’s experience and polypharmacy. Major DDIs (225, 35.1%), moderate DDIs (299, 46.6%), and minor DDIs (117, 18.3%) were recognized as different forms of DDIs based on their severity. Other studies in India and Puducherry21,25 reported a similar trend of minor DDIs. All of this research implies that the prevalence of DDIs varies depending on the patient. The majority of interactions found were significant in nature and pharmacodynamics in mechanism, which is consistent with previous findings.2,8,16,31
The most prevalent drug combinations with significant interactions were warfarin + omeprazole, heparin + aspirin, atorvastatin + dexamethasone, metronidazole + prednisolone, and digoxin + nifedipine. These combinations, however, are occasionally unavoidable and may be indicated. Close monitoring and an assessment of the risk of drug interactions, as well as the advantages of maintaining both medications, are required for such interactions. When these medicines must be used together, laboratory data such as the international normalized ratio and bleeding signs and symptoms should be closely monitored. In the current study, co-administration of a potassium-sparing diuretic (spironolactone) with potassium chloride was observed. When these drugs are taken together, the risk of hyperkalemia rises, and the elderly are more susceptible to this side effect. Other studies 7,11,14,15,32,33 reported these combinations as one of the clinically relevant DDIs.
In the case of polypharmacy, there is a higher likelihood of one or more superfluous medicines being included in a prescription, potentially increasing the risk of avoidable DDIs. According to one study, approximately half of all elderly patients were provided with at least one medically unnecessary medicine. 34 Polypharmacy, on the other hand, does not always imply inappropriate use in the elderly. The drugs are administered for a variety of conditions and goals, including achieving synergy, reducing resistance, and combating adverse drug responses induced by other drugs. Because many drugs are unavoidable in the elderly due to their comorbidities, it is critical not to discard crucial drugs due to the possibility of drug interactions. Many drug interactions can be minimized by taking other drugs, but those that cannot be avoided necessitate awareness of the interaction to ensure adequate management and dose adjustment. In truth, we need to know more than just DDIs; we also need a broad awareness of how to administer different drugs safely to our patients.
Though the number of actual DDIs is lower than the number of potential DDIs, several studies have revealed that the elderly have as many as 25%–47% of clinically significant DDIs.15,35,36
The presence of certain risk factors such as comorbidities, polypharmacy, age, therapeutic range, and drug dosage affects the occurrence of clinically relevant interactions. 37 Studies have found a strong relationship between polypharmacy and DDIs.34,38 The prevalence of DDIs was not significantly associated with age and gender in this investigation, which is consistent with prior studies in different settings.2,16 In this study, polypharmacy was significantly associated with the occurrence of DDIs. This finding is in line with several other studies11,21,36,39,40 which show multiple medications are significant predictors of DDIs in the elderly population. As there is an increase in the number of prescribed medications, there is an increase in the risk of DDIs, which has been proven in one of the studies from Brazil. They reported that the risk of potential DDIs were 39%, 88.8%, and 100% when patients were taking 2–3, 4–5, and 6–7 medications, respectively. 41
Close patient monitoring or the use of alternative drugs can prevent many DDIs in the elderly. However, clinicians may have difficulty recalling the thousands of DDIs and their clinical significance. 42 A clinical pharmacist can assist in the detection and monitoring of DDIs, as well as make any dosage or therapy adjustments. Overall, there were improvements in prescribing quality and the use of appropriate polypharmacy, resulting in lower DDIs.34,43 Decision support systems and information technologies are increasingly being used to avert serious DDIs these days. Even though alert fatigue has been identified as a major drawback to adopting these technologies, clinical pharmacist-assisted computerized decision support systems have been demonstrated to be effective in detecting DDIs. 44
In a resource-constrained situation like ours, the current study sheds light on the occurrence of DDIs in elderly inpatients. The study, however, has some limitations. Because this was a cross-sectional study with only one-time points, it was unable to see the outcome of the DDIs or the actual incidence of the interactions from a clinical standpoint. Another limitation is the absence of information on herbals and dietary supplements.
Conclusion
The results of this study show that the existence of comorbidities puts elderly people at risk of prescription polypharmacy. DDIs were found to be significantly associated with polypharmacy, retired status, and hospital stays. In high-risk populations, such as elderly people, rational prescribing combined with the use of information technology can help to improve medication safety. Detecting and preventing harmful DDIs is an important part of a pharmacist’s mission, and the clinical pharmacist must stay on top of suspected DDIs and make appropriate dosage or therapy adjustments.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the study participants as well as the hospital administration for their cooperation during the study.
Author contributions
Study concept and design: S.B., T.Y., T.G., M.M., and G.B.; acquisition of data and analysis: S.B., T.Y., M.M., S.A., E.A., G.T., and G.B.; interpretation of data: all authors; drafting the article: S.B., T.Y., T.G., S.A., E.A., and G.T.; revising the article: all authors; and final approval of the article: all authors.
Data availability statement
The data set used to support the findings of this investigation is given in the article and the supplementary files.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The ethical approval for this study was obtained from the University of Gondar ethical review committee of the Department of Clinical Pharmacy with approval number (SOP/137/2021). The verbal informed consent was also approved by this committee. Since most of the study participants are illiterate they cannot read; this is why we have used oral informed consent. The individual’s medication profiles were assessed following verbal consent from each participant. Before getting consent, participants were given information about the study’s goals, benefits, and risks. Participants were also assured of the confidentiality of the data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.