
Abstract
Objectives:
Overcrowding in pediatric emergency departments negatively affects the quality of care. Investigating the characteristics of the patients admitted to PEDs will provide valuable information to increase the satisfaction of patients and healthcare staff. This research aimed to investigate the characteristics of pediatric emergency patients in a foundation university hospital in Ankara.
Methods:
This is a retrospective, descriptive, single-center, cross-sectional study, which was conducted with 6550 patients who were admitted to the pediatric emergency department of a foundation university hospital in Ankara, and got diagnosed with one of the 15 most common diseases between 1 August 2017 and 31 July 2018. The associations between the demographics and clinical features of the patients and their diagnoses were evaluated. For comparisons, frequencies, percentages, crosstabs, and chi-square tests were used.
Results:
While none of the patients had a red triage level, 19% had a yellow triage level, and 81% had a green triage level. The three most common diagnoses were fever of unknown origin, cough, and nausea and vomiting. Despite the 0–28 days of age group having the lowest admission rate of 5%, they had the highest usage rate of yellow triage level (66.5%). However, it was the opposite for the 19 months to 5 years of age group with the highest rate of admissions of 49% and the lowest usage rate of yellow triage level (12.8%).
Conclusion:
The reasons for admitting to pediatric emergency department differ according to some contextual variables. Being aware of the current situation is the first step in planning for better pediatric emergency service.
Introduction
The emergency department (ED) is an essential component of the medical services offered in any hospital. 1 Every year, EDs treat 130 million patients in the United States. 2 Compared to other countries, Turkey shows an increasing number of ED admissions by less-urgent patients. 3 This increasing trend causes doctors to spend less time with patients; moreover, it leads to a decrease in the quality of healthcare. Because their 24-hour service is a must to provide continuous care, EDs have been researched from various perspectives including design and triage models.4–6
According to the Turkish Ministry of Health, while the total number of admissions to hospitals in Turkey was approximately 296 million during the first 9 months of 2017, pediatric emergency department (PED) admissions ranked 14th with a percentage of 3% (8 million). 7 Similarly, according to the Turkish Pediatric Emergency and Intensive Care Association, pediatric patients account for 30% of all emergency admissions in 2008. 8 It was reported that 4%–10% of all ED admissions are pediatric patients in the United States. 9 How and why child and parental demographics, and their socioeconomic features including being fatherless and/or motherless, social security coverage, and having a primary care provider (PCP) were associated with increased PED use was well characterized.10–12 In addition, it was also shown that the quality of care in PCP was a key determinant of PED utilization since parents who were dissatisfied with the care of PCP are more likely to have a non-urgent ED visit.13–15 Because EDs are the first choice for admission to a hospital in many cases, ED utilization data are crucial for analysis. 16 There were previous studies with adult ED cases in Turkey, though there is a limited number of research on the characteristics of the pediatric age group.17–20
PED admissions, which account for 30% of all ED admissions, still maintain their high rate despite taking necessary measures. 8 Although the primary purpose of the service in EDs is to provide urgent care for various health problems, they serve mostly non-urgent clinical conditions.21,22 ED usage for non-urgent conditions leads to increasing overcrowding in EDs, and decrease efficiency in treating patients who have serious and “real” emergent conditions.23,24 Overcrowding in EDs can cause long waiting times for emergent cases and poor outcomes including death.22,25 Therefore, it is essential to evaluate ED data to provide a better and more scientific healthcare service. 8
Briefly, the ultimate aim of this study was to evaluate the demographics and certain clinical features of pediatric emergency patients admitted to the PED of a foundation university hospital in Ankara for 1 year. It is expected that this study would contribute to the literature about PED usage, and guide decision-makers in improving the quality of care in emergency medicine.
Methods
Study design and setting
This study is a single-center, retrospective, descriptive, and cross-sectional study in which we studied the demographics and clinical features of pediatric emergency patients. The study was conducted in a tertiary-level hospital that is affiliated with a foundation university in Ankara. The hospital, which has been serving since 1999, has 221 beds, and the ED provides a 24-h uninterrupted service. Approximately 20% of all admissions to the hospital are managed in the ED, which has an integrated radiology unit and surgical intervention room as well. While the patients aged 18 years and older are managed in the adult section of the ED, those under 18 years in the PED.
Sample size and patients
Because we intended to include all eligible patients in the study, we did not calculate an a priori sample size. Patients were evaluated for eligibility according to the inclusion criteria which are as follows: (1) admission to the ED between 1 August 2017 and 31 July 2018, (2) being under 18 years on the day of admission, and (3) diagnosing with one of the 15 most common diseases among all pediatric emergency admissions according to the International Classification of Diseases-10 (ICD-10) coding system. The frequency ranking of diseases was made overall admissions to the PED during the study period (from 1 August 2017 to 31 July 2018). We did not set any exclusion criterion, furthermore, the patients with missing data were also included in the study to obtain more accurate results.
Data and variables
The data were obtained from the electronic record system of the hospital using an electronic data sheet. Since the data collection form used in the study was not structured, no validation or pilot study of the form was conducted. The data consisted of the demographics of the patients (age and gender), date of admission, triage level, number of consultations to other clinics, need for hospitalization, need for surgery, prescriptions, and admission diagnosis codes according to ICD-10. The patients’ names were not obtained from the registration system.
The triage level was defined according to the three-level triage system of the ED, which was put into practice by the Turkish Ministry of Health in 2009. 26 These three levels are as follows: (1) green for third-degree priority, and not requiring urgent attention, (2) yellow for second-degree priority, and requiring attention within an hour, and (3) red for first-degree priority, and requiring immediate intervention.
Ethical considerations
Due to the retrospective nature of this study, it was not able to obtain written informed consent from the patients. Not only this issue but also not gathering any personal data from the patients were stated on the application form to Ufuk University Scientific Research and Publication Ethics Committee, and it was waived by the committee by its approval dated 28 December 2020 and numbered 202/54.
Statistical analysis
Statistical analyses were carried out via the IBM SPSS version 23 software. The associations between categorical variables were examined using the chi-square test. Post-hoc pairwise comparisons were done using post-hoc Z test with Bonferroni correction. 27 A p value of 0.05 was set as the statistical significance threshold.
Results
Of the 26,552 patients admitted to the ED between 1 August 2017 and 31 July 2018, 16,383 were adults, and 10,169 were pediatric emergency patients. Of those pediatric patients, 6550 who got diagnosed with one of the 15 most common diseases were included in the study. Of those 6550 patients, 46.2% (n = 3027) were female, and 53.8% (n = 3523) were male (Table 1).
Demographics of the patients.

Table 1 shows the demographics of the patients. While infants aged 0–28 days had the lowest admission rate of 5.4%, the 19 months to 5 years of age group had the highest rate of 49.1% (Table 1).
There was a statistically significant association between seasons and admission diagnoses (p < 0.05). The three most common diagnoses were fever of unknown origin (FUO), cough, and nausea and vomiting. FUO was statistically significantly diagnosed more frequently during winter and summer compared to spring (p < 0.05). Cough was most commonly diagnosed during winter (23.1%), and the least during summer (9.3%) (p < 0.05). Nausea and vomiting were statistically significantly more common during summer and fall compared to the other seasons (p < 0.05) (Table 2).
Association between season and admission diagnosis.

Chi-square = 584.14; df = 42; p = 0.001.
Season categories without statistically significant difference (Bonferroni correction).
As shown in Table 3, there was a statistically significant association between gender and diagnoses (p < 0.05). The prevalence of the three most common diagnoses, FUO, cough, and nausea and vomiting, were statistically similar between males and females (p > 0.05). However, abdominal and pelvic pain and acute tonsillitis were statistically significantly more frequent in females than males (p < 0.05). Falling and other non-infective gastroenteritis and colitis, on the contrary, were more common in males (p < 0.05).
Association between gender and admission diagnosis.
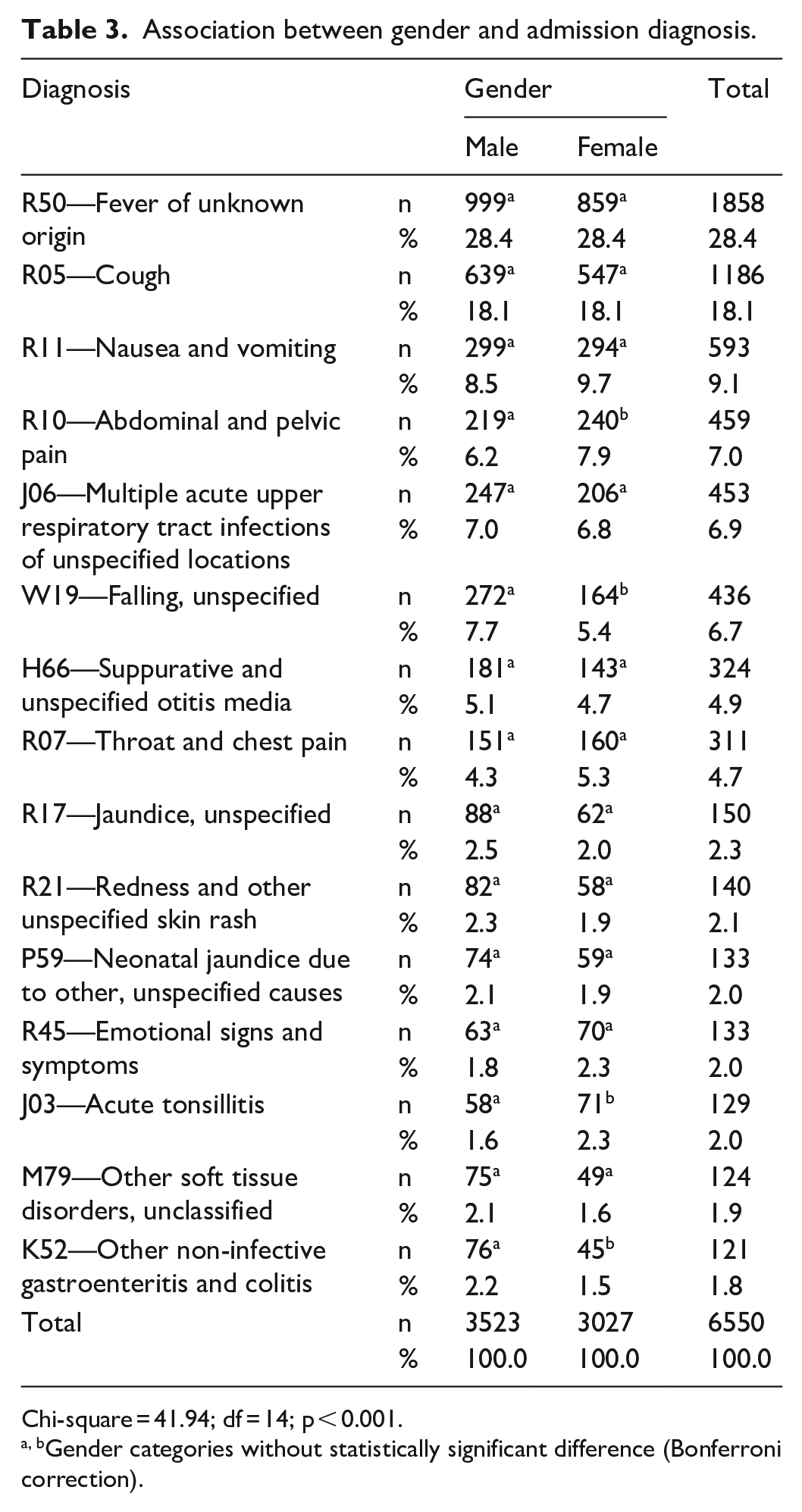
Chi-square = 41.94; df = 14; p < 0.001.
Gender categories without statistically significant difference (Bonferroni correction).
There were again some statistically significant correlations between the patients’ age groups and triage levels (p < 0.05). The yellow triage level was most common in infants 0–28 days old (66.5%), and least common in patients aged between 19 months and 5 years (12.8%) (Table 4).
Association between age and triage level.

Chi-square = 627.05; df = 4; p < 0.001
Age categories without statistically significant difference (Bonferroni correction).
Table 5 illustrates the association between age and admission diagnosis. There was a statistically significant association between age groups and diagnoses (p < 0.05). Of the three most frequent diagnoses, FUO was the most common in both 29 days to 18 months of age group, 19 months to 5 years of age group, and 6–11 years of age group (35.6%, 35.5%, and 22.5%, respectively), and cough was the second most common in those age groups (31.0%, 21.3%, and 13.9%, respectively). However, in infants aged up to 28 days, jaundice was the most frequent diagnosis (76.4%, a total of “Jaundice, unspecified” and “Neonatal jaundice due to other, unspecified causes”). In children aged between 12 and 18 years, on the contrary, abdominal and pelvic pain, and falling were the two most common diagnoses (16.8% and 16.6%, respectively).
Association between age and admission diagnosis.

Chi-square = 6354.3; df = 56; p < 0.001
Age categories without statistically significant difference (Bonferroni correction).
While a consultation with another clinic was requested once in 197 patients, twice in 12, and three times in 1, the remaining 96.8% did not receive any consultation. Although 85% of the study population (n = 5584) had a single admission diagnosis, 13.8% of them (n = 901) had two diagnoses, 0.9% (n = 58) had three, and 0.1% (n = 7) had four, concurrently. While 94.8% (n = 6211) of the patients received no prescription for a medicine, 5.2% (n = 339) had a prescription, 3.6% (n = 238) were hospitalized, and none of them underwent any surgery (Table 6).
Distribution of admissions by number of consultations, number of diagnoses, hospitalization, surgery, and prescription.

Discussion
The main objective of this study was to investigate the demographics and clinical characteristics of the pediatric patients who presented with the 15 most common diseases diagnosed in the PED of a foundation university hospital in Ankara during the study period. Patients’ data were extracted from the electronic patient records of the hospital. Although it was stated that there were deficiencies in hospital registry systems from which patient data were obtained, it is still one of the most reliable data sources.28–30
A slightly higher male ratio was reported in the studies with pediatric emergency patients in Turkey.18–20 However, it was reported that the gender distribution varies from country to country, and according to the characteristics of the society.21,31 In a systematic review, the urgent and non-urgent admission to EDs was found similar in male and female gender. 25 Polat et al. reported that soft-tissue injury (62%), poisoning (75%), and burns (63%) were more common in male patients, while foreign body aspiration (66.7%) was more common in females. However, the three most common diagnoses (FUO, cough, and nausea and vomiting) did not differ between male and female patients in our study. While abdominal and pelvic pain and acute tonsillitis were diagnosed more in females, falling, unspecified, and other non-infective gastroenteritis and colitis were more frequent in males. Although the male gender ratio was slightly higher in the published studies,18,32 further studies were needed to explain the effects of gender on admission to EDs.
Regarding the frequency of diagnoses, Polat et al. 33 reported soft-tissue injury as the most common reason for admission to a PED in Erzurum. Karakas et al., 34 on the contrary, found that fever (22%), cough (16%), and nausea-vomiting (10%) were the three most common principal diagnoses in a PED in Ankara. Similarly, in our study, the three most common diagnoses were also FUO (28%), cough (18%), and nausea and vomiting (9%). Therefore, it can be said that admission diagnoses appear to show similarities in the same region, but not in different regions.33,34
In 2015, 30 million PED visits were reported in the United States, and children younger than 5 years accounted for more than 40% of them. 35 In Turkey, Temizkan et al. 20 and Cag et al. 36 reported that the admission rate of children under 5 years was 36% and 69%, respectively. Considering the distribution of admissions by age groups, Karakas et al. 34 reported that the most common admission was in 1 month–6 years of age group (66%). In this study, the 19 months to 5 years old age group had the highest number of admissions (49.1%), which can be seen as similar to the literature.
In the United States, approximately 30 million pediatric patients applied to EDs in 2015, and the vast majority of them were “treat and release” patients. 35 Pakdemirli et al. 18 reported that 97.5% of all pediatric emergency patients, of whom 16.7% were managed in the green area, was discharged after initial examination and treatment. Anil et al. 19 emphasized that newborns constituted the majority of the hospitalized patients among all admissions to PED. In our study, patients aged 0–28 days comprised two-thirds of yellow triage-level cases, despite having the lowest admission rate. Conversely, despite having the highest admission rate of 49%, the 19 months to 5 years of age group had the lowest frequency among yellow triage-level cases. Two possible reasons for this pattern might be that parents do not take their newborn babies to an ED unless there is a need for immediate attention, and their negative experiences in EDs; but for older aged children it might be the other way around.18,19
In our study, FUO was diagnosed more during winter and summer, cough during winter, and nausea and vomiting during summer and fall. Anıl et al. 19 reported that the admissions to PEDs had increased in winter, and decreased in summer. Similarly, Temizkan et al. 20 showed the number of admission to PEDs increased during the winter months. In addition, it was demonstrated that the frequency of upper respiratory tract infection increased in the winter months, and trauma cases increased in the spring and summer months.20,25,36 In a systematic review, it was reported that the frequency of ED admission was highest in spring and lowest in winter. 25 However, the seasonal variations in childhood diseases, as opposed to adult diseases, might affect the admission diagnosis in pediatric patients. 18
Although Cevikand Tekir 29 reported a consultation rate of 0.27% among all age group emergency patients, Yüksel 6 found that 12.5% of adult emergency patients received a consultation. The higher consultation rate in adults might explain why our study population’s consultation rate was 3.2%. Polat et al. 33 reported that only 3% of their study group were hospitalized. Karakas et al. 34 highlighted that 49% of the patients were given outpatient treatment with a prescription, 48% were discharged without a prescription, and approximately 2% were hospitalized. In our study, 95% of the patients did not receive any prescription, 4% were hospitalized, and none of them underwent surgery. The hospitalization rates in our study appear to be similar to the literature.18,19
In Turkey, as in other countries, PEDs are the only healthcare settings that provide 24 h service to pediatric patients.25,36 In addition to the impossibility of receiving healthcare on weekends and holidays, and within out of hours, parents seeking fast and effective healthcare for their children lead to overcrowding of these units.18,36 The very high numbers of non-urgent admissions to EDs, most of whom can be treated in primary care or outpatient clinics, and the huge amount of discharged patients after initial basic management, address the fact that these units are used for reasons other than clinical situations that require emergency health care.21,25
Limitations
The first limitation of our study was the lack of sample size calculation. We did not calculate an a priori minimum required sample size to include more patients in the study. Because the data of this research is limited to 1-year data of a foundation university hospital in Ankara, our findings may differ in smaller cities or public hospital PEDs. It should also be considered that there may be differences in terms of pediatric emergency admissions between the COVID-19 pandemic era and past years.
Conclusion
Being aware of the current situation is the first step in planning for pediatric emergency service. The non-urgent admission to PEDs, almost all of which can be treated in primary care and outpatient clinics, is a major challenge. Therefore, decision-makers should consider not only improving the quantities but also alternative approaches including strengthening primary care, employing a referral system, and raising the awareness of parents about the proper use of PED to manage this challenge successfully.
Research Data
sj-sav-1-smo-10.1177_20503121221135401 – for Characteristics of pediatric emergency patients in a Turkish tertiary-level hospital: A 1-year cross-sectional study
sj-sav-1-smo-10.1177_20503121221135401 for Characteristics of pediatric emergency patients in a Turkish tertiary-level hospital: A 1-year cross-sectional study by Ayfer Yüksel in SAGE Open Medicine
Supplemental Material
sj-xls-2-smo-10.1177_20503121221135401 – Supplemental material for Characteristics of pediatric emergency patients in a Turkish tertiary-level hospital: A 1-year cross-sectional study
Supplemental material, sj-xls-2-smo-10.1177_20503121221135401 for Characteristics of pediatric emergency patients in a Turkish tertiary-level hospital: A 1-year cross-sectional study by Ayfer Yüksel in SAGE Open Medicine
Footnotes
Acknowledgements
The author thanks Ufuk University Dr. Rıdvan Ege Hospital administrators for their unreserved support and cooperation.
Author contributions
The whole article was prepared by A.Y.
Availability of data and materials
The data set used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Ufuk University Scientific Research and Publication Ethics Committee (dated 28 December 2020 and numbered 202/54).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Due to the retrospective nature of this study, it was not able to obtain written informed consent from the patients. Not only this issue but also not gathering any personal data from the patients were stated on the application form to Ufuk University Scientific Research and Publication Ethics Committee, and it was waived by the committee by its approval dated 28 December 2020 and numbered 202/54.
Publication ethics
The material presented in this manuscript has not been published before nor has it been submitted for publication to another scientific journal or being considered for publication elsewhere.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.