
Abstract
Objectives:
To explore self-care experience of type 1 diabetes mellitus patients at Kemisse General Hospital, North east Ethiopia.
Methods:
A phenomenological study was conducted to explore self-care experience of type 1 diabetes mellitus patients at Kemisse General Hospital from 28 February 2020 to 15 March 2020. Participants were selected using a heterogeneous type of purposive sampling technique. Data were collected using in-depth interviews and observation with the aid of an audio recorder and interview guide by the principal investigator. The thematic analysis approach was used to analyze the data. To facilitate the data analysis process, Atlas. ti software version 7 was used.
Results:
The six interconnected themes that were emerged from the analysis are: (1) physical exercise, (2) dietary practice, (3) medication adherence, (4) self-monitoring of blood sugar, (5) problem-solving skill during hypoglycemia and hyperglycemia, and (6) diabetic foot care.
Conclusion:
The study described that type 1 diabetic patients at Kemisse general hospital faced difficulty in self-care practice, which were difficulty in medication adherence; foot care was neglected diabetes self-care, did not practice diabetes recommended dietary plan and lack of regular physical exercises. In addition to this, self-monitoring of blood sugar was not practiced regularly due to the absence of glucometer machine and financial constraints to buy test strips. In addition to diabetic patient’s role to manage hyperglycemia and hypoglycemic episode, family support was crucial to managing hypoglycemia because most of the respondent’s experience loss of consciousness during a hypoglycemic attack.
Introduction
Diabetes is one of the commonest non-communicable disease (NCD) remains highly prevalent with an increasing incidence globally. It is classified under three major groups, namely, type 1 diabetes mellitus (T1DM), type 2 diabetes mellitus (T2DM), and gestational diabetes. 1
T1DM, which makes up around 5% to 10% of all instances of diabetes and has a big impact on patients’ quality of life (QOL), can occur at any age but is most frequently diagnosed in kids, teenagers, and young adults. 2 The United Kingdom Biobank study project came to the conclusion that 42% of T1DM occurred after the age of 30 years, despite the fact that it affects children and young people. 3
Patients’ long-term self-care behaviors are shaped by their lived experiences with diabetes, which also affect how they feel diabetes. In the context of their social lives, patients’ lived experiences place medication adherence, which affects how they prioritize or deprioritize self-care practices in their daily lives. 4
Therefore, diabetes is a new life experience for the individual. How the individual perceives the disease, the meaning of the disease, illness, and treatment compliance are some of the issues that need to be addressed. 5
Diabetes is a chronic disease with a considerable impact on health status and QOL, and it is considered an urgent public health issue because it has pandemic potential. Based on the projection of the World Health Organization (WHO), by 2025, NCDs will account for over 70% of all deaths globally, with 85% of these occurring in developing countries. 1
The overall increase in the incidence of T1DM is around 3% worldwide on annual basis. 6 Most of the increased number of diabetics has occurred in developing countries. 7 The International Diabetes Federation (IDF) report shows there were 2,567,900 cases of diabetes with a prevalence rate of 5.2% in 2015 in Ethiopia. 8
In 2015, diabetes was one of the leading causes of NCDs death contributing to 1.5 million deaths globally 9 and 321,100 deaths in the African region. 8 Life expectancy for individuals with T1DM is reduced on average by 20 years. 10
Currently, Ethiopia is also challenged by the growing magnitude of chronic NCDs like diabetes. 8 The common cause of diabetes complications in Ethiopia is due to non-adherence, poor attitude toward the disease, unhealthy diet, and physical inactivity. 11
To date, there have been quantitative studies done regarding T1DM in Ethiopia.12–14 However, there is a limited understanding and lack of published qualitative literature regarding the self-care experience of T1DM patients in Ethiopia to the best of our knowledge.
The purpose of this phenomenological study was to explore self-care practice of T1DM patients in everyday life in order to address the aforementioned gap in the area. Furthermore, it was aimed to give T1DM patients voice to express their individual experience and to provide a description of their lived experience. The knowledge can increase the possibility of support for them. Thus, describing self-care practice of people living with T1DM might allow healthcare professionals to recognize the unique needs and concerns of T1DM patients and thereby provide the necessary support.
Methods and materials
Study setting, design, and period
Approach and setting
A descriptive phenomenological study was conducted from February 28, 2020, to March 15, 2020. G.C. A qualitative research approach that helps in describing the lived experiences of an individual is known as phenomenological research. The phenomenological method focuses on studying the phenomena that have impacted an individual. Phenomenological research is a powerful way to understand personal experiences. We use hermeneutic type of phenomenology because it focusses on making meaning of experiences as they are lived. 15 So that, we found phenomenological approach is suitable.
The study was conducted at Kemisse General Hospital, which is found in the Amhara region, is located 325 km from Addis Ababa (the capital city of Ethiopia) and 555 km from Bahir Dar (the capital city of Amhara region). The hospital has chronic disease follow-up out-patient department (OPD) including DM and hypertension). There are 58 T1DM patients according to the report from OPD registration at Kemisse General Hospital.
Population and sample
We recruited a total of 13 T1DM patients from Kemisse General Hospital, and data saturation was maintained. The participants were eligible for the study if they had been receiving care in the study clinic for at least 6 months duration since diagnosis. Seriously ill patients who are unable to communicate at the time of data collection period were excluded from the study.
A heterogeneous type of purposive sampling strategy was used to recruit the participants. Purposeful sampling is a technique widely used in qualitative research for the selection of information-rich cases, individuals that are experienced with a phenomenon of interest. In addition, it considers the ability to communicate experiences and opinions in an articulate, expressive, and reflective manner. 15
The heterogeneous characteristics of participants were maintained by considering age, sex, marital status, educational level, and duration of diagnosis/follow-up. This was done to be able to saw the different forms of the lived experience of self-care among T1DM patients from different perspectives.
Data collection
Data were collected by the principal investigator using a semi-structured in-depth interview guide and observation. During in-depth interview audio recorder was used to collect the data. The overt type of observation was conducted during the interview period by a non-participant observer with the aid of an observational checklist.
We made a list of the characteristics (heterogeneous) that our participants should have. Then, we identified and sampled every person who meets the sample criteria. The doctors and nurses working in the follow-up clinics and admission ward at Kemisse General Hospital helped in identifying patients that fulfill the inclusion criteria of the study.
The informants then voluntarily decided to participate and verbal informed consent was obtained from each of them. For potential participants whose age less than 18 verbal informed consent was obtained from the parents in addition to assent form obtained from participants. When the participant agreed to participate in the study, a meeting was scheduled at date and time that convenient for the participant.
After taking consent, all interviews (face to face) were conducted in the Amharic language. Seven interviews were conducted in a private room at Kemisse General Hospital, one in the café, two at the nearby health facility to their living area, and three at their home. All interview sites were selected by the participant. All interviews were conducted without anyone else present besides the participants and interviewer. Each session lasted between 30 and 50 minutes. The field notes made during the interview. The process of data collection continued until it reached the point of saturation.
Data analysis
Audio-recorded interviews were transcribed verbatim and translated to English by the principal investigator, and the translated data were further checked for accuracy by another independent reader. The thematic analysis approach was used to analyze the data.
Data obtained from observation were written after completion of each fieldwork every day. Once the field notes have been written, we began to look for patterns across the notes by coding the data.
The field notes was taken as by record what the participant said, feel and what saw the researcher while investigated. The principal investigators were read and reread written field notes and the transcriptions several times, and hear the audio-taped interview repeatedly to provide a sense of integrity and understand the meaning of the experiences from the participant’s viewpoint. Each meaning unit was labeled with a code representing its content by open coding and then similar code organized into categories. Atlas. ti software version 7 was used to facilitate data analysis. Two independent coders were participated during coding. Categories were peer-reviewed and checked by the co-lead author and final categories and themes were created. Finally, the report was written based on categories and predefined themes based on objectives for presenting the discoveries of the study. Quotes were used to highlight each category and show association with each theme.
Rigor and trustworthiness of the study
This study was trustworthy based on Lincoln and Guba’s criteria of credibility, dependability, conformability, and transferability. 15
The principal investigator ensured the credibility by developed interview guide was pretested on one T1DM patient in a similar context to maximize the validity. Probing and multiple data sources (combination of in-depth interviews and observation) were employed to collect the data. Participants gave their verbal informed consent to share their data purely for scientific purposes without disclosing their true name. We also invited seven participants to review the ideas for transcription verification, which they think the investigator is going to present a true picture from their perspective. In addition, the principal investigator had at least two phone call contacts with the majority of the participants before data collection to build rapport. Moreover, at the onset of the study, bracketing the preconceptions of the investigator was employed to minimize the investigator’s bias and the risk of reactivity by the participants.
Confirmability of the study was ensured by the recording of every activity of the participants during the time of the interview. In addition, the audio-taped interviews were not destroyed which can enable others to track the process. Moreover, data analysis, interpretations, and conclusions of findings were shared with experienced qualitative researchers for peer debriefing before synthesizing the final outputs.
Dependability was attained through accurate documentation by minimizing spelling errors through frequent check, including all documents in the final report such as including the notes were written during the interview and ensure that the details of the procedures were described to allow the readers to see the basis upon which conclusions was made 16 each of which was considered at all times.
Transferability was achieved by describing the study setting, sample, and data collection procedure clearly and using qualitative expert for peer debriefing.
Results
Socio-demographic characteristics of study participant
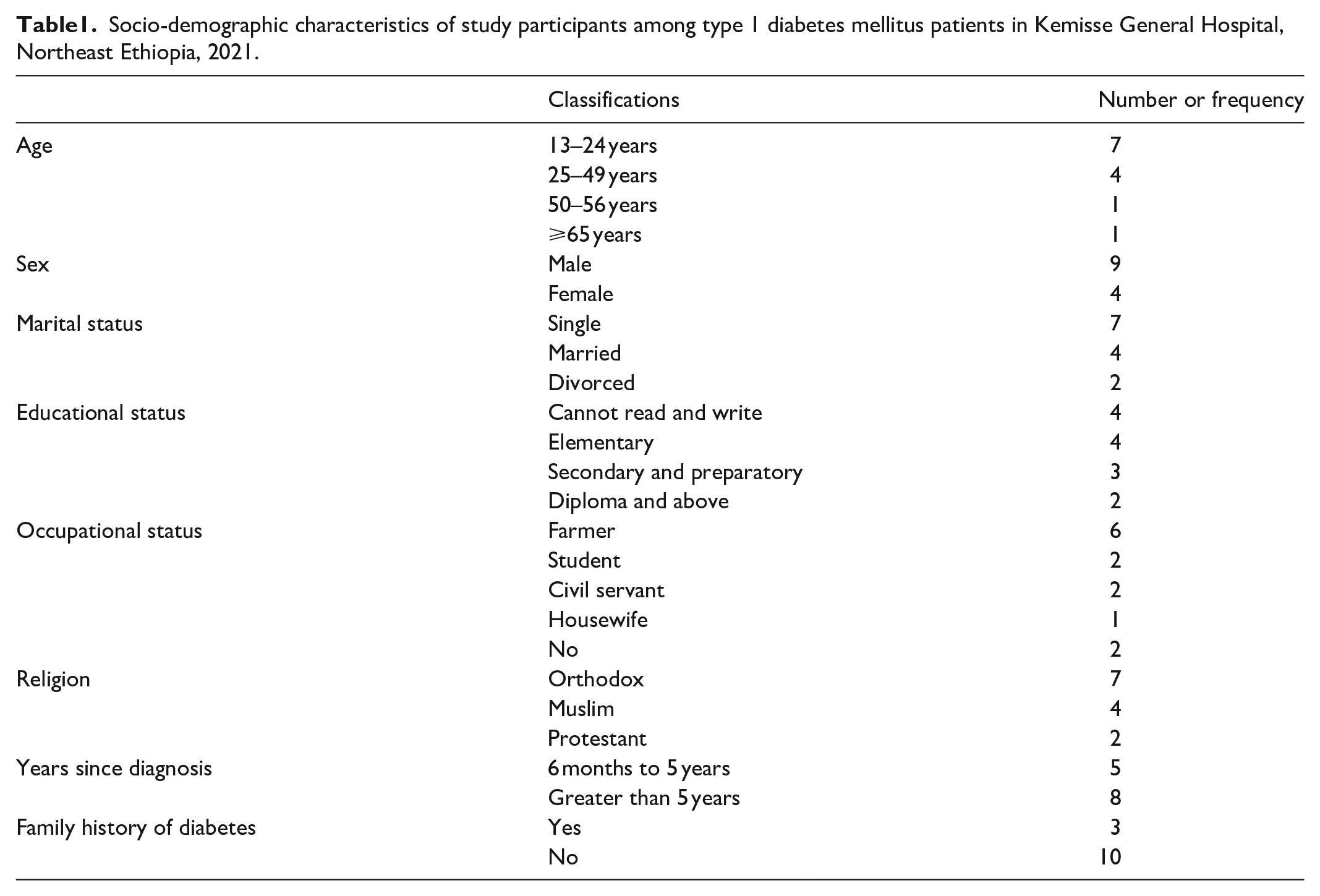
A total of 13 in-depth interviews were conducted. Of 13 participants, 4 of them were females. Their age ranged from 13 to 70 years old. In terms of marital status four were married, seven were single, and two were divorced. With regard to their educational background, seven had attended elementary school, one had attended high school, and the rest five informants could not read and write.
Regarding to religious status, nine of the informants were orthodox, three were Muslim, and one was protestant. Only three of the respondents had a family history of diabetes. Eight of the informants engaged in income-generating activities, while the rest five lived by family support. The informants lived with diabetes from 8 month to 16 years (Table 1).
Socio-demographic characteristics of study participants among type 1 diabetes mellitus patients in Kemisse General Hospital, Northeast Ethiopia, 2021.
The findings that emerged from the analysis of the in-depth interview and observation are presented and arranged as themes and categories. Data analysis has revealed six themes that express self-care experience of T1DM patients. The themes are medication adherence (with two subthemes including insulin injection–related experience and barrier for medication adherence), dietary practice, physical exercise, self-monitoring of blood sugar, problem-solving skill during hypoglycemia and hyperglycemia, and diabetic foot care.
Self-care practice
Medication adherence
Medication adherence was one of the emerged themes (with two subthemes including insulin injection–related experience and barrier for medication adherence) from self-care practice.
Insulin injection–related experience
All informants felt that taking medications is very important in the management of diabetes. They were informed about the insulin injection technique at first diagnosis. Almost all participants were totally adherent to their insulin injection in regard to the dose and time. The majority of participants took insulin injection using all possible sites (thigh, abdomen (around umbilicus), and arm). Few participants did not take the injection at their abdomen (around umbilicus) because they did not think it is the appropriate site. Few participants were afraid to take insulin injection by themselves so that caregivers gave the injection to them.
I use insulin based on hospital counseling and it has its own levels. When I check my blood sugar levels every month for example, when it is above 337, I am taking my medicine 24 in the morning, 16 in the evening, and when it is below 150, I am taking my medicine 20 in the morning and 12 at evening. I am taking an injection shot at left arm, right arm, left thigh, right thigh, and around the umbilicus (pointing those listed body parts by his right-hand finger). 32-year-old male respondent
The other participants did not adhere to their insulin injection since they were changing (increase or decrease) the medication dose, skipping dose intentionally, and changing the time of taking their medication. The desire to control blood sugar levels was a motivation for most patients to always inject insulin despite it was boring to take injections for life long. There was a patient who tried to stop taking insulin injections because she had felt her condition was well-regulated. During withdrawal, her condition got complicated. This made her realize that diabetes cannot be cured but can be controlled by taking insulin injections.
I quite the syringe (stop using insulin injection), I think the disease left me when I was eating lemons (soft laughter). When I arrived (in Ethiopia), I started eating lemons on an empty stomach, then my blood flowed through my nose and my mouse, my stomach was ulcerated and since that time I have to follow up for gastric ulcer. 23-year-old female respondent
The major side effects that were reported by some of the participants were swelling at the site of injection and hypoglycemia. This was confirmed by the observation that some participants faced small multiple swelling on their arms, but all participants faced skin color change to black at all possible sites of injection. Patients were frustrated and scared when the pain became too much especially during the first month of their diagnosis.
The side effect is that it swelled to the area where I was taking the injection and it became like stone, it bothers me a lot, but what can I do? Life is difficult (laugh while smile). When I was piercing the needle on the swollen tough skin of my body, it was very painful. What can I do because the Creator has brought it? I can live by tolerating the pain. 32-year-old male respondent
In addition, only one participant faced severe problems during insulin injection which was insulin syringe breakage inside her thigh because of inappropriate injection technique.
When I was injecting the needle in my thigh, the needle was pulled down and broken to trap inside (pointing to her left thigh by her right hand). it was broken when I took the injection because I didn’t know the injection technique . . . When they [doctors at Saudi] told me that my foot was going to be amputated because the broken needle was not able to come out, I refused and told them I would enter my country, and I came from Saudi to my country [Ethiopia]. I didn’t take anything, they [doctors at Saudi] just gave me the only option to be amputated. Then, as my thigh was swollen and exploded, the needle went out. then, it was wounded, but healed as soon. 23-year-old female respondent
Barrier for medication adherence
Even though all the participants reported that they stored the insulin drug in a cold place, only two of them had refrigerators. Most of the respondents prepared a traditional cold place which was made from sand and water with a small container that can be used for storage of insulin.
I put the medicine in a large glass which has sand and water, and at the center, it has a hole which is the site for placement of medicine. When it is dry and warm, I lose the sand with water to keep it cool. 70-year-old male respondent
During journey, some respondents carried food such as bread, candy, sugar, and water due to fear of hypoglycemia, and they carried medicine with self-prepared cold storage, but some participants said that they missed their doses when they traveled away from home. They carried insulin without cold storage even if they knew it was warm.
When I travel by car, I carry food to eat and I carry sugar in my pocket because no one is there if I am getting hungry, it will drop me. Unfortunately, If I don’t catch food, I will not take my medicine until finish my journey because there is no food there, so I am afraid it will be difficult for me if it drops me while taking the medicine. When I get to where I was thinking, I am going to take my medicine because I get food. Even if I know I shouldn’t have to miss the medicine hour, I do . . . 32-year-old male respondent
The barriers for adherence of the participants to their insulin injection include fear of hypoglycemia, workload throughout the day and substitute it with herbal medicine while four participants did not mention any barrier to medication adherence. Although patients would averagely adhere to inject their insulin, few respondents had taken herbal medicines to get cure from diabetes, but they did not get any relief as compared from insulin.
Now, I am giving up to leave it, but I have anything to try and I spent a lot of money when they saying they would cure me with traditional medicine. I myself have been drinking by preparing remedy from many kinds of herbs starting from the leaf of the (shiferawu) [moringa]. 32-year-old male respondent
Moreover, fear of taking insulin injection with the presence of other people since they felt ashamed of and performed religious activities like fasting and going at prayer for holy water were other challenges for medication adherence. During fasting, a few of the participants missed morning doses due to fear of the side effects insulin injection has. Some of the participants attended religious activities at monasteries to cure diabetes by holy water. Although some of the governors of the monastery allow taking insulin injection besides holy water, some of the other governors forbid using insulin injection at the spiritual place. The following are illustrative quotes: I didn’t take my insulin medication in front of someone else and in a crowded place because my family didn’t let me take it in this situation and they prefer to stay alone since I am a rural girl, I am ashamed to inject insulin in front of someone else. 17-year-old female respondent I went to holy water for praying. When I went . . . (skip the name of the monastery) monastery, they prevented me from taking the medicine. Then, I left it for 8 days. The food was wheat [wheat bread], and it burned my heart and I was nothing else . . . I did not experience falling, but I did not fast . . . 23-year-old female respondent
Dietary practice
The dietary practice was an essential care practice for people with diabetes which was reported by all informants, but they did not follow their specific diet plan which is recommended for diabetes patients to maintain a balance between carbohydrate, protein, and fatty foods. All participants had no idea of the approximate number of proteins, carbohydrates, and fats recommended for people with diabetes.
I eat what I have, but I don’t eat balanced nourishing foods purposely to maintain the food that has energy [carbohydrate] and building body [protein]. There is nothing to eat that I think about to balance my nourishment. 23-year-old female respondent
All participants reported their usual diet consisted of Injera (a staple food in most parts of Ethiopia which is made of a locally grown grain ‘teff’, ‘other cereals’, and ‘mixture of teff with other cereals’) every day. The majority of respondents reported that they did not eat frequently like other diabetic people. They keep regular feeding habit which is breakfast, lunch, and dinner as like other normal people follow. In contrast, there are some respondents who eat frequently because diabetes makes them hunger.
I eat only injera bewet, but did not eat vegetarian food very much because I live at rural area. I didn’t wait a specific time to eat food, there is a time when the medicine makes me like hyena [very hungry]. Of course, I didn’t care if I didn’t eat for 24 hours before, now this time my family was scared that I will fall due to hunger. 32-year-old male respondent
The majority of enrolled participants reported that they wanted to decrease their carbohydrate intake to control their diabetes through avoidance (maximum reduction) of soft drinks, spaghetti, macaroni, sweet potato, wheat bread, and avoidance of sweets such as sugarcane, cakes, candy, chewing gum, juice, honey, and table sugar is necessary for controlling blood glucose levels. They reduced taking salty foods and alcohol drinking like beer, ouzo and from local drinks like arekie (local ouzo), tella, and Teji. Moreover, most participants mentioned that fat consumption should be reduced through the consumption of red meat instead of white type and reduction of oily or greasy foods. Meanwhile, one participant mentioned that he should increase vegetable intake.
. . . I eat small bread, but I want to avoid the bread at all because wheat is not allowed to persons with sugar [diabetes]. I try to struggle to eat vegetables and it is good for me. I avoid drinking soft drinks that I liked before the illness. When I am rarely foolish to drink soft drinks, at that time I frequently urinate due to this . . . 55-year-old male respondent
Preparing separate meals for a diabetic person in a family is practical only in the time of holiday. Almost all participants agreed with the family to help them comply with eating healthy food through preparing special foods during the holiday because they must adhere to their regular feeding habits. They did not eat foods which were prepared for other people during the holiday because it is too salty, oily, and fatty nature.
I used to eat with my family on holiday, but now I stop eating with them because the food that prepared was either too salty or too greasy and fatty which was not suitable for my pain [diabetes] and they are preparing food for me according to my needs. 22-year-old male respondent
The majority of respondents reported having trouble handling the social aspects of meals, which were more difficult during events like weddings, religious celebrations like mahber, and holiday invitations. Even though Ethiopians view sharing food at social gatherings as a way to show one another their respect and affection and view refusing to eat from a communal dish as unacceptable, the majority of respondents said they would not share the foods and drinks served at those special ceremonies because they had diabetes.
When I go to a wedding, I don’t eat greasy and salty food, I don’t drink Tella [local drink] because it has barley, I just go to wedding ceremony only for play. 19-year-old male respondent
Moreover, the reported barriers for non-adherence to the healthy eating include personal sweet preference, feeling hungry while no other choice, eating outside home, and taking meals with the other person.
If I need to eat, I don’t wait for people to eat because I eat alone to save my life. If I am in a place where there is no food for me, I eat with another person, and if the food is sweet, I will leave by taking two (gursha) a little (wesfaten lememeles) [to return my hunger], then I will go home and eat as I want. 22-year-old male respondent
Practices with regard to regular physical exercise
Physical exercise was not practiced by nearly half of the respondents. Most of them believed that it was necessary, but the reported reasons for not doing regular physical exercise were physical constraints like surgical steel on leg and back pain, getting tired, lack of time, absence of convenient place, being old age, and a busy work schedule. Moreover, respondents said that they did not like wake up early in the morning and did not have anyone to work with.
I do homework every day, but I didn’t do sport because it was not fun to do it now [old age] for me (laughter with a smile), but it creates fun when our kids did it. 42-year-old female respondent
From those who work physical exercise, only some participants did regularly. Besides this, the majority of respondents reported that they performed daily routine activities since physical inactivity has an influence on diabetic control.
I work out the physical exercise to control my diabetes. When I go to a rural area, I work [physical exercise] because the compound is large. I move because of work [routine activity]. I do rope jumping outside of my daily routine. I only do rope jumping and I have not a lot of mobility because my back is too dry to move and I have back pain so much. If I have no other work at home, I can work jumping rope for at least 5 days per week. I take 30 minutes per day to work, and I am working by regulating the time which takes to complete it. 23-year-old female respondent
During physical exercise, some of the respondents experienced preventing hypoglycemia by taking actions like doing exercise until they got sweaty, decreasing the time for exercise, taking some sugar, reducing the dose of insulin, and eating some food.
When I do physical exercise, I reduce the number of workouts to keep my sugar level not decrease below normal. Then I reduce the dose of the drug for sugar [diabetes], which I am going to take the injection. When it decreases [blood sugar level], I didn’t perform the activity but just sit after taking the needle [insulin injection]. When I feel tired while working out, I left it to prevent a decrease (blood sugar levels). I was working by checking the watch. 17-year-old female respondent
Self-monitoring of blood glucose
Majority of the study, participants reported that they checked their blood sugar level only during their follow-up visits to the hospital every 1 month. They felt that it was usually very difficult to have a glucometer machine at home because of financial constraints, even they did not know whether it can be sold or not and they did not know the procedure. Those who did not own the glucometer machine at home went to the nearby health facility in addition to monthly hospital-based checkups when they felt only ill.
I don’t have the equipment to automatically measure sugar levels. I don’t have the ability to buy it, I don’t know where it lives, but they [health professionals] measure my sugar levels at a health facility when I go for a monthly checkup. 17-year-old male respondent
Even patients who had their own glucometer machine at home-reported testing their blood sugar when they suspect high or low blood sugar level through symptoms of hypoglycemia and hyperglycemia. They did not test their blood sugar level regularly because of financial constraints to buy test strip as well as non-availability of the test strips at the pharmaceutical shop.
I have equipment for measuring sugar [blood sugar level]. When I suspect my sugar level is high or low, I was forced to use the instrument. I suspect my blood sugar level is low when I feel easily fatigability and sometimes faint. I can’t check my blood sugar level frequently because I bought 50 test strips with 450 Ethiopian birrs since it was very expensive. 55-year-old male respondent
Diabetic foot care
Foot care was neglected diabetic self-care practice among the majority of study participants. The reasons behind this were thinking that foot care was unnecessary, lack of knowledge, lack of foot ulcer, lack of assistance to do care, and negligence. Although some of them reported foot injury as one of the common health problems for them, they did not practice foot care even if they were told to do care from health professionals.
I have never taken care of my foot because I have no ulcer and I don’t think that care must be taken. 16-year-old male respondent
Few participants practiced foot care and they gave more attention to choose appropriate footwear. Some participants had experience of foot wound, but all of they recovered from it quickly. The finding from observation revealed that all informants did not have an ulcer in their foot and no one amputated, but some of them had scars which show experience of the previous wound on leg and one of them travel with the aid of left-hand crunch to support his left leg due to a car accident.
I take care of my feet. I don’t walk barefoot and wear shoes. When I have to keep my feet from getting wound, I have to go straight, I don’t break wood, nor do I fetch water. I do not want to be dirty. I can bathe every day and see if my leg hurt or not and then I wear my clothes cleanly. I don’t wash it in hot water rather in cold water. 17-year-old female respondent
Problem-solving skills during hypoglycemia and hyperglycemia
The most common problems that are faced by all participants in their life include hypoglycemia and hyperglycemia. Some of the respondents reported that living with diabetes was hard since they were struggling to correct their blood sugar level in order to prevent hyperglycemia and hypoglycemia. There are four problem-solving strategies used by T1DM patients during hypoglycemia and hyperglycemia such as family support, support from health professionals, carbohydrate consumption, and self-adjusting insulin dose.
Living with diabetes is just like when a person protects the grain from wild animals such as hogs and monkeys, I live in suspiciously if the disease either make me dope or comes other complication . . . 70-year-old male respondent
The reported symptoms of hypoglycemia from the majority of informants include tremor, dizziness, sweating, hunger, blurred vision, weakness, and coma. To control hypoglycemia, majority of participants manage it by carbohydrate consumption through eating or drinking sweets like sugar, candy, and ‘mirinda’ without checking their blood glucose levels at home. If they were in a coma, their families assist them to manage it by feeding them sweet foods and taking them at a nearby health facility if the hypoglycemic attack not reverses to normal condition through home treatment. Most of the respondents mentioned that family’s support could also have great role to control diabetes.
When the pain starts to fall me to the ground, it shakes me like a person who has epilepsy or malaria . . . (by showing shaking his hand). Then people take me to the hospital and then they [health professionals] gave me medicine and my health is restored. If I felt the pain when I was conscious, I would eat some food, but when I could fall asleep at night and unconscious to feel the pain, my family who knew about my condition at that time would give me a drink like tea or Mirinda and took me to the health facility if my health condition did not return. My blood sugar levels increase again when my family gave me sugar . . . 17-year-old male respondent
The reported symptoms of hyperglycemia from the majority of informants include easy fatigability, excessive urination, excessive thirst, and excessive hunger. To control hyperglycemia most respondents went to the health facility to seek support from health professionals in order to manage it, but some of the participants tried to manage it by taking some actions like fasting and doing some physical activities. In addition to this, few participants took their own decision to take high-dose insulin without the order of health professionals.
My sugar level had got increased. I didn’t know when they were taking me to the health facility because I was at loss of consciousness . . . . In another time when it was increased, I pierced the needle [insulin injection] by myself [without the order of doctors] to control it. At some point I got 600 sugars [blood sugar level], I was taking an injection twice with a dose of fully 100. Then, when I measured after injection, it turned to 478, and then I calmed myself. 23-year-old female respondent
Moreover, some of the respondents carry food like sugar, candy, and water in their pocket or bag at all times which helped them to manage hypoglycemic episodes. Few of them were feeling happy by carrying those things which they consider as lifesavers or guardians.
I have sugar in my pocket. Using sugar in my pocket feels like guardians. Without it, I have no guardian. Now if it drops me here, you will not save me, but the sugar rather saves me. I know when the symptom comes such as while my eyes are dark to close my eye when my ear made me deaf. If I will not suspect quickly to take sugar (he showed me festal-wrapped sugar out of his pocket), I don’t move for a short distance. If other people don’t reach for me, I will die. 70-year-old male respondent
Discussion
In this study, self-care practices were poor since patients did not strictly adhere in routine self-monitoring of blood sugar did not follow recommended dietary the plan did not do diabetic foot care and did not do regular physical activity. However, studies conducted in Ireland, 17 Netherland, 18 United Kingdom, 19 and Sunderland 20 revealed the opposite result, which was many patients described rigidly adhering to a rigorous routine of testing, eating, develop new skill on the inspections of feet, and activity to avoid seriously complications of diabetes and to keep themselves alive. The reason of difference might be from the study settings (community or institution and rural or urban), educational statues and socio-economic backgrounds status so difference among the studies’ participants. This might be due to a proper understanding of the importance of diabetes self-care practice and the devastating consequences of diabetes by persons with diabetes in developed countries. Those Europe countries health education interventions focus more on life style modification, that is, the main reason why they have better achievement as compared to Ethiopia. The other possible explanation is not having access to blood glucose monitoring a daily basis is a main obstacle in Ethiopia.
Physical exercise was not practiced regularly by most participants in this study. In contrast, a study conducted at British 21 revealed that young people felt that exercising helped them to manage their diabetes and had a beneficial psychological and physical impact on their bodies. This difference might be due to the presence of convenient working area for physical exercises like the gym in British and the study involved only young diabetic patients who may be energetic to do physical exercise in contrast to this study, which involved patients with a variety of different age groups including old age. 21
On the contrary, patients faced many problems like non-availability of the refrigerator for storage of insulin and very difficult to maintain timing with food during traveling which was a similar result in the study conducted at West Bengal, 22 taking wrong dosages of insulin and avoiding taking insulin which also similar result within the study conducted at Zambia; 23 in which non-adherence behaviors of diabetes patients such as taking wrong dosages of insulin, avoiding taking insulin, and not attending clinical appointments. This implies that there is a tendency to skip doses or postpone injections during traveling and taking the wrong dosage of insulin besides the self-dose adjustment without the order of health professionals leads to both acute and chronic complications of diabetes.
In this the study, self-care experience of T1DM patients was explored in detail from patients’ perspectives in their own words; since the study took a phenomenological approach. The findings of this study considered the heterogeneous characteristics of the research participants which allowed the principal investigator to saw the data from a different perspective. The limitation of the study was the inability to generalize the findings of this phenomenological study. No matter the phenomenon being investigated, the conclusions derived by the principal investigator apply only to that aspect of reality that was perceived by all participants. The characteristics of the sample of participants place additional limitations to the possibility of generalizing the findings of an investigation. Although diversity should be a goal of the sampling process, it may never be fully achieved.
Conclusion
The study described that T1DM patients at Kemisse General Hospital faced difficulty in self-care practice, which were difficulty in medication adherence; foot care was neglected diabetes self-care, did not practice diabetes recommended dietary plan, and lack of regular physical exercises. Most of these problems linked with the context related to study settings, educational statues and socio-economic backgrounds status. In addition to this, self-monitoring of blood sugar was not practiced regularly due to the absence of a glucometer machine and financial constraints to buy test strips.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221126862 – Supplemental material for Self-care practice, lived experience of type 1 diabetes mellitus patients at Kemisse General Hospital, North Eastern Ethiopia: Phenomenological study
Supplemental material, sj-docx-1-smo-10.1177_20503121221126862 for Self-care practice, lived experience of type 1 diabetes mellitus patients at Kemisse General Hospital, North Eastern Ethiopia: Phenomenological study by Eyob Ketema Bogale, Habtamu Wondiye, Yamrot Debela, Tadele Fentabil Anagaw, Lelisa Worku and Natnael Kebede in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to give their special thanks to Amhara Regional Health Bureau for funding this research project study participants for their contributions to this study, Kemisse General Hospital staff for their assistance with patient recruitment, Demisawu Assefa for checking the accuracy of the translated data, and Tsegaye Mekasha for checking the grammatical error of the report, and Eyob Getachew for peer-reviewing.
Authors contribution
EK, HW and YD, participated in the conception and design of the study. EK carried out data collection. EK, HW, YD, TF and NK participated in the data analysis and interpretation. EK, TF and NK drafted the manuscript, HW and YD reviewed and edited the manuscript. All authors read and approved the final manuscript
Authors information
E.K., H.W., Y.D. & T.F.:—School of Medicine and Health Sciences, Health Promotion and Behavioral Sciences, Bahir Dar University, Bahir Dar, Ethiopia.
N.K.:—Health Promotion and Behavioral Sciences Department, Wollo University, Dessie, Ethiopia.
L.W.:—Hailu Worku Medium clinics, Tafo, Oromia, Ethiopia EK, HW (Assistant Professor), TF and NK:—credential was Mph in Health Promotion.
Y.D.:—credential was Mph in Health Promotion (Assistant Professor) and PHD fellow.
L.W.:—credential was Mph in Public Health Nutrition.
All researchers are male except Y.D.
Consent for publication
The authors declare that they have agreed to publish on this journal.
Availability of data and materials
The data sets generated and analyzed during this study are not publicly available due to the sensitive nature of this research. However, some aspects of the data sets are available from the corresponding author on reasonable request
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical approval was obtained from the Instructional Review Board (IRB) of Bahir Dar University College of medicine and health sciences with reference number of CHMS 008/02/2020. The Institutional Review Board of College of Medicine and Health Sciences, Bahir Dar University decided and approved that verbal informed consent obtained from each study participant could be enough to be ethically assured of the research process. This was because unless the name and the participants’ medical registration number (MRN) were used during data collection, there is no ethical issue that will be raised. For participants <18 years, caretakers were asked to provide consent for their child’s participation, approval, and consent to participate. Permission to undertake the study was performed at all levels. Caretakers were given detailed information about the purpose of the study, data collection procedures, and possible risks/discomforts and benefits of participating in the study through the consent process. Verbal informed consent was obtained from all caretakers whose children participated in the study. In this case, the families were presented as caretakers. A child was included in the study only if the caretakers agreed with the child. Despite the caretakers, consent, a child’s decision not to participate in the study was respected.
The data collector has read the consent form to participants who could not read and write, so they are aware of all conditions. Verbal informed consent was obtained from each study participant before the commencement of data collection. Confidentiality of information was received from the study participants maintained by using codes rather than the name of participants during data collection procedures. Participants also gave their verbal informed consent to share their data purely for scientific purposes without disclosing their true name. Participants were informed that participation was voluntary.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.