
Abstract
Background:
Birth weight is one of the major determinants of perinatal survival, infant morbidity, and mortality. There are only few published reports on assessment of low birth weight in Ethiopia and the determinants of low birth weight have not been well characterized.
Objective:
The aim of this study was to assess determinants of low birth weight among live birth newborns delivered at public hospitals in Gamo Gofa Zone, South Ethiopia.
Methods:
Institution-based case control study was conducted from February 25 to April 25, 2018 and consecutively selected 60 cases and 240 controls were enrolled in this study. The data were collected using face-to-face interview and review of medical records. Moreover, we have measured the newborns’ birth weight using a standard weight scale and mother’s mid-upper arm circumference using a standard World Health Organization mid-upper arm circumference measuring tape. Statistical analysis of the data was done using SPSS version 21.
Results:
A total of 300 newborns were included in the study. Late antenatal care booking (adjusted odds ratio = 1.87, confidence interval = [1.32–2.6]), birth interval <2 years (adjusted odds ratio = 0.385, confidence interval = [0.176–0.83]), anemia (adjusted odds ratio = 4.4, confidence interval = [1.84–10.5]), mid-upper arm circumference <23 cm (adjusted odds ratio = 7.99, confidence interval = [3.5–20.3]), nutritional counseling (adjusted odds ratio = 5.85, confidence interval = [2.14–14.8]), and husband smoking (adjusted odds ratio = 4.73; confidence interval = [1.42–15.7]) were found to be determinant factors of low birth weight.
Conclusion:
Most of the determining factors of low birth weight were preventable. Therefore, clinical and public health interventions should target on those determinant factors to prevent its adverse effects.
Introduction
Birth weight is the first weight of the newborn obtained after birth. It is one of the major determinants of perinatal survival, infant morbidity, and mortality as well as the risk of developmental disabilities and illnesses in future.1,2 Low birth weight (LBW) has been defined by the World Health Organization (WHO) as weight at birth of less than 2500 g (5.5 pounds). Annually, more than 20 million infants are born with LBW in the world. The prevalence of LBW in developing countries (16.5%) is more than twice the prevalence in developed regions (7%).3,4
Africa is a continent that has high rates of children born with LBW and most recent studies have shown a high rate of child mortality. It is expected that in sub-Saharan Africa, LBW represents 14.3% that is approximately twice the rate of LBW in European country. 5
In Ethiopia, according to Federal Minster of Health National New Born and Child Survival Strategy Summary report, the prevalence of LBW was found to be 20%. 6 Studies conducted in different parts of the country found different prevalence rates of LBW. Accordingly, studies conducted in Addis Ababa, Gondar, and Tigray showed that the prevalence of LBW was 8.8%, 11.2%, and 14.6%, respectively.7–9
Several studies have shown that LBW was significantly associated with maternal residence, marital status, age at first pregnancy, bad obstetrics history, maternal nutritional status, inter-pregnancy interval, antenatal care (ANC) follow-up, pregnancy-induced hypertension, anemia at pregnancy, chat chewing, and cigarette smoking.10–12
Study on determinant factors of LBW is important for planning child health care services and to improve the survival of LBW babies. However, there are only few published studies in Ethiopia on the assessment of LBW 13 and there is paucity of information related to the determining factors of LBW. Even the available studies did not address the broader determinants of LBW.13,14 Factors like maternal nutritional status, maternal chronic diabetes, and Rh factor of the mothers have been well explained by the majority of available studies.13,15–18 Possible determinants of LBW will vary across the geographical location. 18 Thus, the aim of this study was to assess determinants of LBW among live birth newborns delivered at public hospitals in Gamo Gofa Zone, South Ethiopia.
Materials and methods
This study was conducted in Gamo Gofa Zone, South Ethiopia. The capital city of Gamo Gofa Zone is Arba Minch, which is located 505 km away from Addis Ababa and 275 km South West of Hawassa, capital city of South Ethiopia. According to 2007 National Census, the total population of Gamo Gofa zone is 2,019,687. 19 Estimated number of women of reproductive age (15–49 years) is 470,587, estimated number of live birth is 69,881, and the skilled delivery rate is 51.2%. In this zone, there are two general hospitals, four primary hospitals, 73 health centers, and 471 health posts. 19 The study was conducted from February 25 to April 25, 2018.
A hospital-based case control study design was conducted in selected hospitals of Gamo Gofa zone, South Ethiopia. Sixty LBW babies (cases), who were delivered in the three hospitals during the study period were selected consecutively and a total of 240 babies with normal birth weight (controls) were also selected. Cases which occurred in the selected hospitals were included in the sample until the necessary number has been reached. However, following each case four controls were selected on the same day. When there were more than four eligible controls after each case, only four controls were selected randomly. Moreover, when there were multiple birth cases or controls, one of the cases or controls was selected randomly. Congenital anomalies, still birth, and mothers who were not volunteered to participate in the study were excluded from this study.
The number of cases and controls was calculated using Epi Info Version 7 by taking power at 80%, odds ratio of 2.9, two-sided significant level at 0.05, and proportion of controls with exposure as 11.6. 20 Two general and one primary hospital were selected based on the availability of pregnant women from all parts of the zone. The total samples were allocated to the selected hospitals proportionally using the hospitals’ number of live birth in the last quarter of the preceding year as reference. Accordingly, 50 (10 cases and 40 controls) participants from Chencha primary Hospital, 150 (30 cases and 120 controls) participants from Arba Minch General Hospital, and 100 (20 cases and 80 controls) participants from Sawula General Hospital were selected.
The data were collected using pretested structured questionnaire by trained midwives and nurses. Data extraction sheet and questionnaire related to sociodemographic characteristics, obstetrics-related factors, medical history, and nutritional status were prepared after reviewing differently related literatures20–24 (refer “Supplemental material”). Questionnaire related to behavioral factors were adapted and customized from the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST). 25 Data on behavioral and sociodemographic factors of the participants were collected by face-to-face interview. Information on medical and obstetrics history were extracted from medical records using data extraction sheet. Measurement of maternal mid-upper arm circumference (MUAC) was made without clothes using a standard WHO MUAC measuring tape. The new born weight was measured within 1 h after birth using a standard weighing scale by trained personnel. Based on the birth weight, a new born with weight less than 2500 g is considered as LBW. 26
ANC visit was classified on the basis of minimum recommended visits as having four or more visits and less than four visits. Inter-pregnancy interval was collected and classified as <2 years and ⩾2 years based on WHO recommendations. 27
Mothers who got any advice related to nutrition and diet by health professionals during pregnancy was taken as “yes” for nutritional counseling question. Maternal iron and folic acid intake was assessed by asking the mothers whether or not she had taken it for at least 3 months. Mid-upper circumference was categorized as <23 and ⩾23 cm using Food and Nutrition Technical Assistance III (FANTA III) cut of point. 28 Chronic medical illness was defined as a pre-existing medical illness of the mother that was documented in hospital medical records with an onset prior to the current pregnancy. Maternal anemia was diagnosed when hemoglobin level was below 11 g/dL. 29 Mothers who ever used cigarettes, chat, and alcohol (beer, wine, tella, areke, etc.), and husbands who ever smoked cigarettes at least weekly was considered as “yes” for the purpose of this study. 30
To assure data quality, 1-day training was given on data collection process for all data collectors and supervisors. The collected data were checked for completeness by principal investigator and supervisors each day. Pretest was done on 5% of the sample that were not included in the main study. Then, necessary modifications of the questionnaire and data extraction sheet were undertaken.
Data were entered into EPI info version 7 and exported in to SPSS version 21 for analysis. Descriptive statistics was computed to present sociodemographic and other characteristics of the study participants. Binary logistic regression analysis was also performed to identify associated factors of LBW. Variables with p value <0.25 in the bivariate analysis were further tested using multivariate logistic regression analysis. The results of the analysis were presented with texts and tables. A p value <0.05 was considered as statistically significant.
Ethical clearance was obtained from Institutional Review Board (IRB) of Arba Minch University. The IRB had reviewed the study protocol and approved with ethical approval reference number IRB/81/2010. Then, permission letter to conduct the study was obtained from the hospital administration office. The respondents were informed about the purpose of the study and data were collected after obtaining written informed consent from the study participants. Confidentiality of the information was maintained throughout the study.
Results
Sociodemographic characteristics
A total of 300 (60 cases and 240 controls) newborns were included in this study with 100% response rate. The mean (± SD) weight of the newborn was 2076 g ± 308.16 g for cases and 3264.17 g ± 513.47 g for controls. Among the mothers of the newborns, majority of the cases (68.3%) and controls (73.3%) were within the age range of 20–34 years. The mean age of the mothers was 28 ± 7 years for both groups. Majority of the cases (60%) and controls (62.1%) were urban residents (Table 1).
Sociodemographic and obstetric characteristics of mother who gave birth at the selected hospitals of Gamo Gofa Zone, South Ethiopia, 2018.

ETB: Ethiopian Birr; ANC: antenatal care; Rh: Rhesus factor.
N = 36 for cases and N = 206 for control.
N = 32 for cases and N = 152 for control.
Obstetrics-related characteristics
Majority of cases (53.3%) and controls (63.3%) were multipara, 18.3% of cases and 7.8% of controls had history of still birth, 21.7% of cases and 7.1% of controls had history of preterm birth, and 10% of cases and 11.3% of controls had history of abortion. Regarding to the Rh factor of the mothers, 26.7% of cases and 5.8% of controls had negative Rh factor. About 60% of cases and 85.8% of controls had ANC follow up (Table 1).
Medical- and behavioral-related characteristics
In this study, 15% of cases and 7.5% of controls had history of chronic diseases, 28.7% of cases and 15% of controls had drunk alcohols, 16.7% of cases’ husband and 5.4% of controls’ husband used cigarette (Table 2).
Medical, behavioral, and nutritional profiles of mothers who gave birth at the selected hospitals of Gamo Gofa Zone, South Ethiopia, 2018.

MUAC: mid-upper arm circumference.
Nutrition-related factors
Regarding to the nutritional status, 55% of cases and majority of controls (86.7%) had got nutritional counseling. About 53.3% of cases and 88.7% of controls had MUAC ⩾ 23 cm (Table 2).
Factors associated with LBW
Variables like marital status, monthly income, parity, history of preterm birth, maternal Rh factor, ANC visit, time start ANC visit, number of ANC visit, gestational age, types of gestation, birth interval, nutritional counseling, iron and folic acid supplementation, MUAC, anemia, history of chronic illness, maternal smoking status, chat chewing, alcohol drinking, and husband smoking status had a value of p < 0.25 and were included in multivariable analysis (Table 3). After adjusting for those variables in multivariable analysis; late ANC booking (adjusted odds ratio (aOR) = 1.87, confidence interval (CI) = [1.32–2.6]), birth interval < 2 years (aOR = 0.385, CI = [0.176–0.83]), anemia (aOR = 4.4, CI = [1.84–10.5]), MUAC < 23 cm (aOR = 7.99, CI = [3.5–20.3]), nutritional counseling (aOR = 5.85, CI = [2.14–14.8]), and husband smoking (aOR = 4.73; CI = [1.42–15.7]) were independent determinants of LBW (Table 4).
Bivariable logistic regression results of mothers who gave birth at the selected hospitals of Gamo Gofa Zone, South Ethiopia, 2018.

ETB: Ethiopian Birr; COR: crude odds ratio; CI: confidence interval; ANC: antenatal care; Rh: Rhesus factor; Ref.: reference category; MUAC: mid upper arm circumference.
Factors associated with low birth weight among mothers who delivered at the selected hospitals of Gamo Gofa Zone, South Ethiopia, 2018 (n = 300).
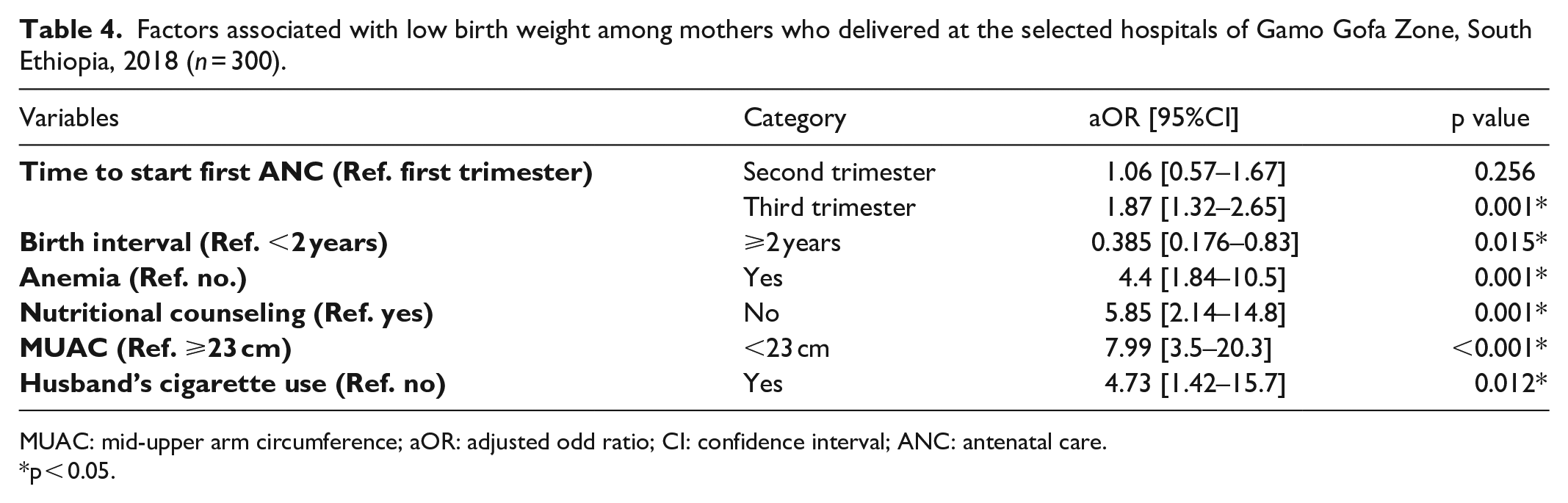
MUAC: mid-upper arm circumference; aOR: adjusted odd ratio; CI: confidence interval; ANC: antenatal care.
p < 0.05.
Discussion
The odds of LBW was 1.87 times higher for newborns from mothers who had late antenatal booking as compared to newborns from mothers who had ANC booking early. This finding is supported by the study conducted in Nepal and Addis Ababa, Ethiopia.8,25,31 This might be due to the fact that early antenatal booking enables early prevention, detection, and management of different risk factors for adverse pregnancy outcome like LBW.
Newborns from mothers who had birth interval of 2 or more years were less likely to be LBW as compared to their counterpart. This finding is in concurrent with another study conducted in India, Bale, and Addis Ababa, Ethiopia.20,30,32 This might be due to short inter-pregnancy interval that do not provide a mother with sufficient time to recover from the nutritional burden and stress of the previous pregnancy. This leads to maternal nutrition depletion. It also associated with maternal iron and folic acid depletion which compromises the mother’s ability to support fetal growth and development which in turn increases the risks of preterm birth, growth restriction, and LBW in the subsequent pregnancies.33–35
The odds of LBW was 4.4 times higher in newborns from anemic mothers as compared to newborns from none anemic mothers. This finding is supported by the study conducted in India and Debre Markos, Ethiopia.12,32 Anemia could impair oxygen and nutrient delivery to the fetus and delay normal intra-uterine growth and also influencing placental angiogenesis.36,37 However, the current finding is in contrast to the study conducted in Debre Birhan. 18 This discrepancy may be due to difference in data collection techniques and study population. Our study techniques was both prospective and retrospective whereas the study conducted in Debre Birhan was used only card review. Also our study tried to address diverse population from different geographic areas. On the contrary, the study in Debre Birhan was conducted in a single urban hospital.
The odd of LBW was 5.85 times higher for newborns from mothers who didn’t get nutritional counseling than newborns from mothers who were counseled for nutrition. This finding is in agreement with the study conducted in Bahir Dar, Dessie, and Japan.21,38,39 Nutritional requirement increases in quality as well as in quantity during pregnancy. 40 Thus, nutritional counseling and support during pregnancy have paramount importance for better pregnancy outcomes.
The odds of LBW among newborns from mothers who had MUAC < 23 cm were higher compared to those newborns from mothers who had MUAC ⩾ 23 cm. This finding was consistent with other study conducted in Indonesia and Bahir Dar.33,35 This could be due to the fact that fetal development in uterus directly depends on the level of maternal nutritional condition. When mothers had nutritional deficiency, intra-uterine growth of the fetus will be restricted and leads to LBW.41,42
The odds of LBW for newborns from mothers who had smoker husband were 4.73 times higher as compared to newborns from mothers who had non-smoker husband. This result was supported by study conducted in Pakistan and Addis Ababa.30,43 This is due to the fact that smoking has adverse effects on the developing fetus by increasing level of nicotine and carbon monoxide in the blood which result in deficiency of oxygen and nutrient delivery to the growing fetus.44–46
This study assesses the determinants of LBW among live birth newborns delivered at hospitals. However, the present study still had some limitations. Information on some maternal factors like pre-pregnancy BMI, weight gain, data on dietary intake, and wealth index was not included. We tried to explore behavioral factors with self-reporting. The respondent may not give the correct answer due to fear, shame, and feeling of guilt. This may lead to information bias and it may results in underestimation of the hypothesized relationship between exposure and outcome. Also, this study is hospital based and hence further large-scale community based studies are needed to explore other determinant factors of LBW.
Conclusion
Many studies confirm that LBW remains a major public health problem in developing countries. This study also evidence that, time to start first ANC visit, birth spacing, anemia, nutritional counseling, and MUAC and husband history of cigarette use were significantly associated with LBW. Most of the factors are modifiable and the risk of LBW can be prevented by targeting clinical and public health interventions on those determinant factors. As a recommendation, further large-scale community-based study is needed to explore other determinant factors of LBW.
Supplemental Material
Questionnaire – Supplemental material for Determinants of low birth weight among live birth newborns delivered at public hospitals in Gamo Gofa Zone, South Ethiopia: Unmatched case control study
Supplemental material, Questionnaire for Determinants of low birth weight among live birth newborns delivered at public hospitals in Gamo Gofa Zone, South Ethiopia: Unmatched case control study by Alemu Basazin Mingude, Woiynshet Gebretsadik, Dresilgn Misker and Gashaw Garedew Woldeamanuel in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all data collectors for their cooperation in data collection and all the women who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Arba Minch University. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical approval
Ethical approval for this study was obtained from Institutional Review Board (IRB) of ArbaMinch University, ArbaMinch, Ethiopia with approval reference number IRB/81/2010.
Informed consent
The written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.