
Abstract
Objectives:
The COVID-19 pandemic has significantly impacted individual health, potentially increasing the demand for home medicine storage. However, inappropriate household medicine storage can lead to drug waste and unnecessary hazards. This study aimed to explore the prevalence of and identify the factors that predict medicine storage in Vietnamese households.
Methods:
A community-based cross-sectional study was conducted with 800 households in Danang, Vietnam. A multi-stage sampling method was applied in this study. The data collection tool was modified from previous studies and consisted of three sections: household head characteristics, household characteristics, and medicine storage practice. Bivariable and multivariable binary logistic regression analyses were used to identify the factors influencing medicine storage at a p-value of less than 0.05.
Results:
Among 800 households surveyed, 71.6% stored medicine. Analgesics-antipyretics were the most common type of medicine stored (80.8%). 90.1% of households obtained their medicines from private pharmacies, 68.1% of households stored medicine for future use and 58.8% had a home medicine cabinet. 9.4% of households did not store medicine in the appropriate packaging and 19.4% of households did not check the expiry date of their medicine. Educational level (AOR = 2.74; 95% CI = 1.84–4.06), income (AOR = 11.38; 95% CI = 1.46–88.79), presence of chronic illnesses (AOR = 12.44; 95% CI = 7.20–21.21), presence of children (AOR = 2.36; 95% CI = 1.56–3.58), presence of healthcare professionals (AOR = 2.14; 95% CI = 1.28–3.56) were predictors of the medicine storage.
Conclusions:
The current study found a high prevalence of household medication storage and some inappropriate storage behaviors. Therefore, attention should be given to develop effective interventions and policies to promote safe and appropriate storage practices.
Introduction
Worldwide, most households store medicines to treat various illnesses, including acute and chronic diseases. 1 A recent systematic review found that 77% of households globally store medications, with analgesics and antibiotics being the most common types. 1 These medications may be prescribed by healthcare professionals or purchased over-the-counter. 2
Households store medicines at home for various reasons, including emergency cases, future use, treatment changes, non-adherence, misunderstanding of drug use, and high drug costs.3,4 The COVID-19 pandemic has also led to an increase in household medicine storage, as people have become more concerned about having access to essential drugs. 5 Easy access to medications can increase the potential risks of community drug storage in developing countries. The presence of medicines in the household might have negative impacts, including an increase in the risk of self-medication, improper drug use, side effects, and a decrease in the treatment efficacy.6,7
A notable issue is that some households store medicines in unsuitable conditions, such as improper storage temperature and humidity.4,8,9 This can increase the risk of drug deterioration and expiration, leading to medication toxicity. 10 It is crucial to store medications out of reach of children, in locked cabinets or drawers, and in their original packaging with clear labels to prevent confusion or accidental ingestion. Controlling where drugs are kept at home is essential, especially for unintentional users such as children. However, drug poisoning is still common among children due to parental negligence. 7 Additionally, having drugs in the home increases the chance that people will share them with friends, family, and the community, which can lead to improper drug use and a higher risk of developing drug resistance. 2
In Vietnam, while there is a government-run healthcare system, many people choose to forego it in favor of buying their medications from private pharmacies because it is more convenient and accessible. 11 This results in a significant fraction of residents self-medicating without a prescription. As a result, many drugs are potentially stored in the community.6,12 However, the issue of household drug storage has not yet been adequately addressed, especially in the context of COVID-19, which has influenced people’s medication usage. 13 Therefore, this study was conducted to understand the prevalence of medicine storage and identify the factors that predict medicine storage in Vietnamese households. The results of this study are essential for policymakers to develop effective interventions to eliminate inappropriate drug storage behaviors in the community.
Methods
Study design and settings
A community-based cross-sectional study was conducted in Da Nang, Vietnam, to assess the prevalence of medicine storage and the factors that predict medicine storage in Vietnamese households. Data were collected through face-to-face interviews using a structured questionnaire. Da Nang is the largest city in Central Vietnam, with an area of 1284.9 square kilometers and a population of 1,220,287 people. It is an important economic hub in the region and is administratively divided into seven districts: Thanh Khe, Hai Chau, Son Tra, Ngu Hanh Son, Cam Le, Hoa Vang, and Lien Chieu. The city also has 56 wards and 2784 residential areas.
Sample and sampling
The sample size was calculated using the single population proportion formula, considering a 95% confidence interval, a margin of error of 5%, an estimated participation rate of 50%, and a design effect of 2. The estimated sample size was 769 households, rounded up to 800 households.
The formula for calculating the sample size for a single population proportion is:

where:
● n is the sample size
● Z is the z-score for the desired confidence level (1.96 for a 95% confidence interval)
● q is the estimated proportion of the population without the characteristic of interest (50% in this study)
● d is the margin of error (5% in this study)
● deff is the design effect of the study
The design effect is a correction factor that accounts for the varying likelihood of different population members being selected for the sample. In this study, the design effect was 2, which is common for multistage sampling designs. The estimated sample size of 769 households was rounded off to 800 households.
To recruit households, a multistage sampling method was employed. First, four districts were randomly selected from Danang’s seven districts. Next, two wards were randomly selected from each chosen district. Then, five residential areas were randomly selected from each chosen ward. Finally, 20 households were randomly selected from each residential area to participate in the study. Simple random sampling was used at all stages, and the Research Randomizer website (https://www.randomizer.org) generated the random numbers (Figure 1).
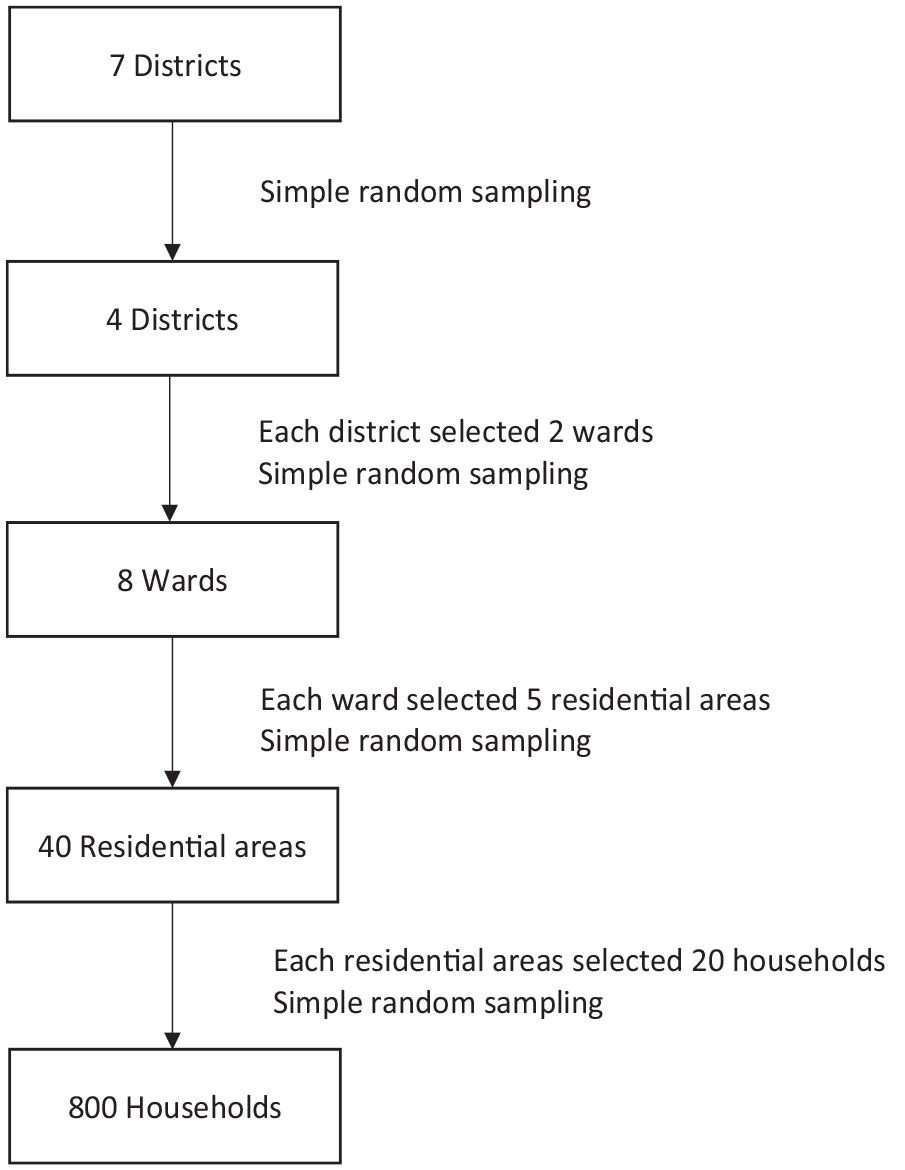
Diagram illustrating the sampling procedure of the study.
Study participants
Data collection within households was conducted with the head of household, who typically holds the final decision-making authority regarding health matters for household members. The inclusion criteria were being at least 18 years old and possess the ability to read and write. The exclusion criteria, on the other hand, were having a history of cognitive impairment and being unable or refusing to participate in the interview. A mini-mental state examination (MMSE) was used to screen the cognitive impairment of older people. Those who had MMSE scores less than 24 were excluded from the study.
Study instrument
A structured questionnaire was developed by modifying previously published studies.5,14 The questionnaire consisted of three sections: (1) household head characteristics, (2) household characteristics, and (3) medicine storage practices. The first section included questions on household head characteristics such as age, gender, marital status, educational level, employment status, and income. The second section collected information about household characteristics such as the number of members, the presence of children 6 years old or younger, the presence of older people (⩾60 years old), the presence of chronic illnesses, and the presence of health professionals. The third section collected information about medicine storage practices, including the purpose of storage, the type of stored medicine, the number of medicine categories, sources of medicine, places of storage, storage in separate packages, and checking the expiration dates.
The third section of the survey collected information about the context of medicine storage at home. The dependent variable was medicine storage practice, which was assessed by asking respondents whether or not they stored medicines at home. The independent variables included age, gender, marital status, educational level, employment status, income, number of household members, presence of chronic illnesses, presence of children 6 years old or younger, presence of older people (60 years old or older), and presence of health professionals in the household. These independent variables were included in the model to identify factors that predict medicine storage practice.
The questionnaire was sent to five experts to assess its content validity. Each expert was chosen based on their expertise in the field of study that the questionnaire was designed to measure. The experts reviewed the questionnaire and provided feedback on the clarity, relevance, and comprehensiveness of the items. They rated each item on a 5-point scale, with 1 being “not relevant” and 5 being “very relevant.” The content validity ratio (CVR) is the average of the ratings for each item. The CVR for each item ranged from 0.6 to 1, indicating that all of the items were considered to be at least somewhat relevant to the construct being measured. The content validity index (CVI) is the average of the CVRs for all of the items. The CVI of the whole questionnaire was 0.98, indicating that the questionnaire has high content validity.
A pilot test was conducted with 30 respondents to assess the clarity and comprehensibility of the questionnaire. Pilot test participants were asked to complete the questionnaire and provide feedback on any items they found unclear or difficult to understand. Based on the feedback from the experts and the pilot test participants, a few minor changes were made to the questionnaire to improve its clarity. The data from the pilot test were not used in the final study analysis.
Data collection
Data were collected via face-to-face interviews using a structured questionnaire from November 2022 to March 2023. Based on a list of recruited households, researchers set up appointments with the heads of households, then visited the households to collect data. Before the interviews, participants were informed of the purpose of the survey and their right to withdraw at any time without consequence. Written informed consent was obtained from all participants before data collection. Face-to-face interviews were conducted only if participants agreed and signed the consent form. Interviews were conducted in participants’ homes and lasted for about 15–20 min. For the questions “What kind of medicines do you store?” and “How many types of medicines do you store?” the collectors asked participants to show the medications they had at home. Collected data were kept confidential and anonymous to protect participants’ privacy.
Data analysis
Data were entered and analyzed using SPSS version 22. Descriptive statistics, such as frequencies and percentages, were used to describe the data. Bivariate binary logistic regression was used to identify variables associated with medication storage practices. Variables that were found to be associated with medication storage practices were then entered into a multivariable binary logistic regression model to control for confounding factors. The final model included variables with adjusted odds ratios (AORs) that were statistically significant (p < 0.05) with 95% confidence intervals (CIs). Model fitness was assessed using the Hosmer-Lemeshow goodness-of-fit test, which yielded a p-value of 0.29, indicating that the model was a good fit for the data.
Ethical considerations
The study was approved by Research and Ethics Committee at the Danang University of Medical Technology and Pharmacy, No. 34/CT-HDDD. Additionally, local district authorities had granted permission to collect data on communities. The study was conducted according to the ethical guidelines of the Declaration of Helsinki. Written informed consent was obtained from all subjects before the study.
Results
Socio-demographic characteristics of respondents and households
Of the 800 households visited, 218 (27.2%) respondents were older people. 441 (55.1%) respondents were female. The majority of respondents (84.1%) were married. 329 (41.1%) respondents had undergraduate or higher education. A high proportion of respondents (70.1%) were employed. 383 (47.9%) respondents had an income of less than 5 million Vietnamese Dongs (VND) (Table 1).
Socio-demographic characteristics of respondents and households (n = 800).

As presented in Table 1, 450 (56.3%) households had less than five members. Three hundred eight (38.5%) households had a member with a chronic illness. Around one-third of households had children 6 years old or younger (35.6%) and people aged 60 years old or older (39.6%). One hundred sixty-six (20.7%) of households had a member working as a healthcare professional (Table 1).
Medicine storage in households
Out of 800 households, 573 (71.6%) households stored medicines at home (Chart 1). Analgesics-antipyretics (463/573, 80.8%) were the most common drugs stored, followed by gastrointestinal drugs (182/573, 31.8%), cardiovascular drugs (179/573, 31.2%), dermatological drugs (147/573, 25.7%), respiratory drugs (112/573, 19.5%), endocrine drugs (68/573, 11.9%), and antibiotics (59/573, 10.3%) (Chart 2). Nearly one-third of households (185/573, 32.3%) stored three or more types of medication (Chart 3).

Percentage of households stored medicine (n = 800).
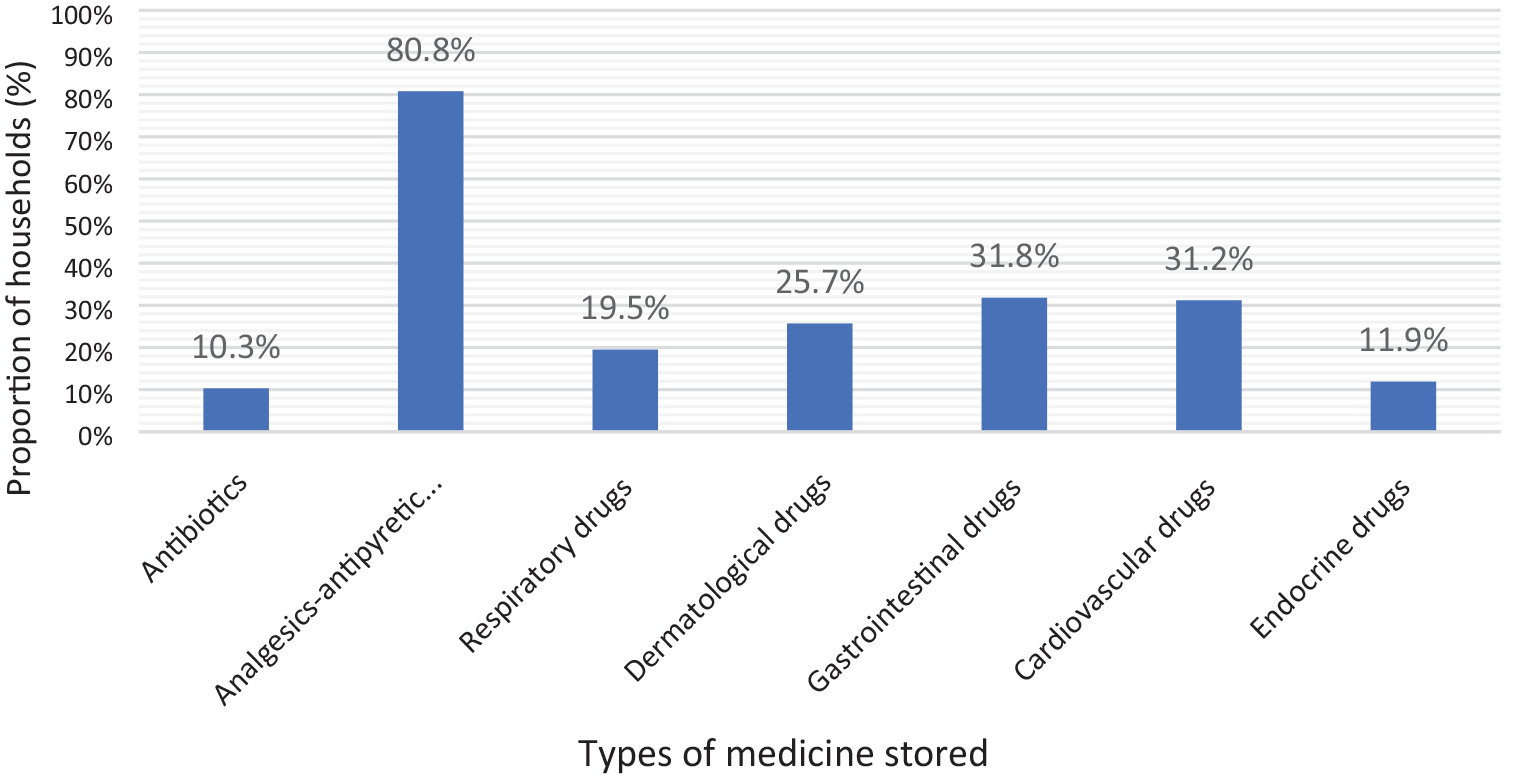
Percentage distribution of medicine types stored in households (n = 573).
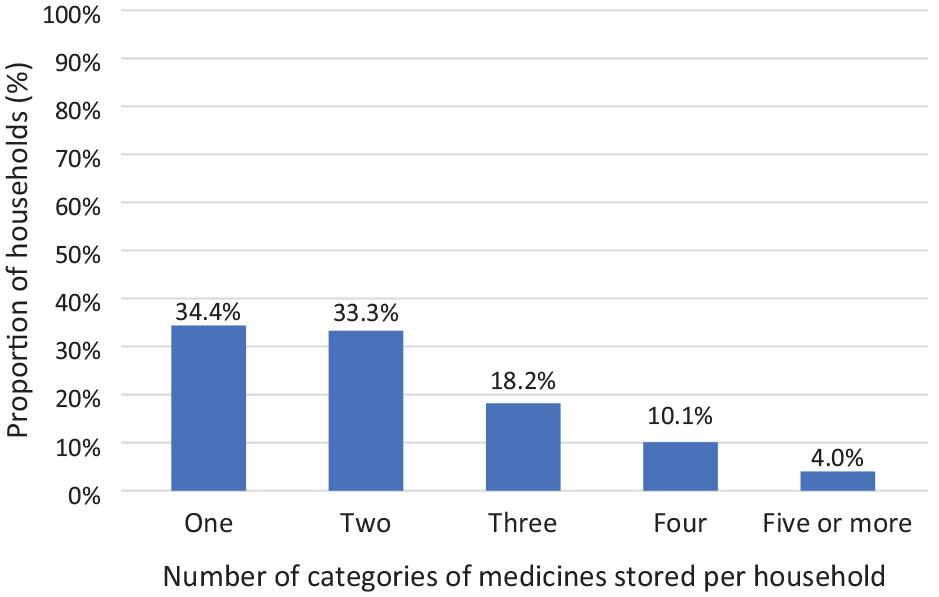
Percentage distribution of the number of medicine types stored in households (n = 573).
Of the 573 households that stored medicines, 516 (90.1%) obtained medicines from private pharmacies and 390 (68.1%) stored medicines for future use. More than half (58.8%) had a medicine cabinet at home. The kitchen (201/573, 35.1%) and living room (205/573, 35.8%) were the most common places to store medicines. Fifty-four (9.4%) households did not store medicines in their original packaging. One hundred eleven households (19.4%) did not check the expiration dates of their drugs regularly (Table 2).
Characteristics of medicine storage at households (n = 573).

Predictors of medicine storage in the households
A multivariate logistic regression model was used to predict the likelihood of household medication storage. The model explained 33.8% of the variance in the data and correctly predicted 77% of the cases. The five significant factors that predicted household medication storage were education level, income, the presence of chronic illness, children 6 years old or younger, and healthcare professionals in households. The odds of household medication storage were 2.74 times higher among respondents with undergraduate and higher education when compared with the other respondents (AOR = 2.74; 95% CI = 1.84–4.06). The respondents with an income of 15 million VND per month or more were 11.38 times more likely to store medicines at home compared to those with an income of less than 5 million VND per month (AOR = 11.38; 95% CI = 1.46–88.79). Households with a family member who had chronic illnesses were 12.44 times more likely to store medicines at home than households without a family member with a chronic illness (AOR = 12.44; 95% CI = 7.20–21.21). Families with children 6 years old or younger were 2.36 times more likely to store medicines at home than households without these children (AOR = 2.36; 95% CI = 1.56–3.58). Drug storage was 2.14 times more likely in households with relatives working in the healthcare profession than in households without these members (AOR = 2.14; 95% CI = 1.28–3.56) (Table 3).
Bivariable and multivariable binary logistic regression for predictors of medicine storage in households, Vietnam (n = 800).

COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval; VND: Vietnamese dongs.
Hosmer-Lemeshow goodness-of-fit test: Chi-square = 9.668, df (8), p = 0.289.
p < 0.05; Nagelkerke R2 = 0.338; Cox and Snell R2 = 0.236;
Discussion
The study aimed to assess medicine storage and its predictors among households in Vietnam. The study revealed that a significant proportion (71.6%) of households kept medicine at home. The prevalence of home medicine storage in this study was higher than that reported in studies done in Uganda and Ethiopia (29%–48%).5,14–16 However, this finding was lower than that of studies done in Iraq, the United States of America, Qatar, Iran, and Ireland (>80%).4,10,17–19 This discrepancy may be due to variations in national economies, healthcare systems, insurance regimes, and individual drug usage patterns. Furthermore, cultural factors and access to healthcare services may also contribute to the differences in home medicine storage rates across countries. It is important to consider these factors when interpreting and comparing findings from different studies on this topic.
In line with other studies,5,15,20 analgesics and antipyretics were the most common drugs stored at home. Common analgesics are widely available and can be purchased without a prescription at pharmacies in Vietnam. In addition, the COVID-19 pandemic also prompted individuals to store analgesics at home as a precaution. The perception that analgesics can provide relief for various common illnesses might also influence their popularity as a stored drug at home. 21 These issues could explain the popularity of analgesics stored in households.
In this study, about one-third of households stored three or more types of medications. In addition, around two-thirds of households kept medicines for future use. Moreover, private pharmacies were the most common sources of medications, and about one in five households did not check the expiration dates of their drugs regularly. These findings are consistent with previous studies.5,14 It highlighted the potential risks of improper drug usage behaviors such as storing multiple types of medications and self-medication, which can lead to an increased risk of drug resistance and drug poisoning. These findings emphasize the importance of educating households about proper medication storage practices to mitigate these risks. Furthermore, further research is needed to explore the factors contributing to these behaviors and develop targeted interventions to promote safe medication practices in households.
This study corroborated the findings of a previous study, 8 which revealed that only 58.8% of households possessed medicine cabinets. Common storage locations included the kitchen, living room, and bedroom. The storage environment plays a crucial role in maintaining drug quality and ensuring treatment compliance. If medications are stored in conditions where light, temperature, and humidity are not controlled, there is an increased risk of drug degradation, potential health hazards, and reduced treatment efficacy.22,23 This study demonstrated that a substantial proportion of households stored medications in inappropriate locations, such as kitchens, living rooms, and bedrooms, putting children at risk of accidental ingestion. The study also found that some households did not store medications in separate packaging. WHO guidelines recommend storing medications in a locked cabinet out of children’s reach, in a cool, dry environment, to address these issues effectively. 24
Consistent with other studies,5,14 the practice of medicine storage in households was significantly influenced by household income and the presence of members with chronic illnesses. Households with a member earning over 15 million VND per month were 11.38 times more likely to store medications than those with members earning less than 5 million VND. Individuals with higher incomes tend to purchase prophylactic and supplementary medications. Conversely, those with lower incomes may purchase medications in smaller quantities and only when necessary due to financial constraints. Regarding chronic illnesses, households with members suffering from chronic diseases were 12.44 times more likely to store medications at home than those without such members. This may be because individuals with chronic illnesses often require multiple medications for extended periods.
Notably, the odds ratios for the association between income, chronic illnesses, and household medication storage were quite high, suggesting a strong association between these factors and medication storage practices. However, the possibility of confounding variables influencing the observed associations cannot be ruled out. Future research should explore potential confounding factors such as access to healthcare services or health insurance coverage. Additionally, investigating the role of cultural beliefs and attitudes toward medication storage may provide further insights into the observed associations.
Among subjects with varying levels of education, there was a difference in medication storage practices. Households with respondents enrolled in undergraduate or higher education were 2.74 times more likely to store medications than those with lower levels of education. This may be because individuals with higher education levels are more likely to be confident in their ability to learn and understand medication information independently. Consequently, these individuals may be more inclined to self-medicate, leading to higher rates of medication storage compared to those with lower education levels. 25 Additionally, previous studies have shown that households with educated parents are more likely to keep medications on hand for future use. 8
In line with previous research, 8 households with children 6 years old or younger were 2.36 times more likely to store medications at home than those without such children. This outcome might stem from self-medication behaviour, misconceptions about drugs and drug abuse by Vietnamese parents toward young children. 26 However, this practice poses a high risk of accidental ingestion if medications are not stored securely out of children’s reach and sight.
The present study found that households with family members working in the medical sector were 2.14 times more likely to store medications at home than those without such relatives. This finding aligns with previous research. 5 This may be because individuals working in the healthcare sector have a greater understanding of medications and tend to self-medicate for themselves and their families for minor ailments. Consequently, these households are more likely to store medications at home compared to those without relatives in the medical field.
Strengths and limitations of the study
The study has several strengths. First, the large sample size (n = 800) ensures the validity of the data and increases the statistical power of the study. Moreover, the multistage sampling technique improves the representativeness of the population. However, the study was conducted in only one region, so the findings cannot be generalized to the entire population.
Conclusions
The findings of this study highlight the importance of promoting safe medication storage practices in households. It is crucial to educate families about the potential risks of storing medications in unsafe places and encourage them to invest in proper medicine cabinets or storage solutions. This study also identifies the factors that influence medication storage, namely income and the presence of chronic conditions, which significantly contribute to the need for readily available medications. Understanding the characteristics and influencing factors of medication storage practices in the Vietnamese community can help regulatory agencies and policymakers develop targeted interventions to improve medication safety and accessibility. This study can also inform the development of educational programs to raise awareness of safe medication storage practices among the Vietnamese population.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241227371 – Supplemental material for Prevalence and determinants of household medicine storage in Vietnam: A community-based cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121241227371 for Prevalence and determinants of household medicine storage in Vietnam: A community-based cross-sectional study by Thi Tieu Mai Diep, Quynh Nhu Nguyen, Thi Thuy Le, Van Nho Le and Thanh Quang Nguyen in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank all the study participants for their willingness to participate in this study.
Author contributions
Concept: TQN, TTMD, TTL, and VNL; Design: TQN and TTMD; Resources: TTL, VNL, QNN, TTMD, and TQN; Materials: QNN, TTMD, and TQN; Data Collection: TTL, VNL, QNN, TQN, and TTMD; Analysis and Interpretation: TTMD and QNN; Literature Search: TTMD, QNN, and TQN; Writing Manuscript: TTMD and TQN; Critical Review: TTL and VNL.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.