
Abstract
Objectives:
The study determined the prevalence of malaria infection and its association with socio-demographics, environmental, housing, and co-morbid ailment factors.
Methods:
The study was a cross-sectional of 330 consented adult febrile patients who were recruited at a tertiary health facility in rural Southwestern Nigeria. The standardized interviewer-administered questionnaire sought information on their socio-demographics, environmental, housing, and co-morbid ailment factors. Venous blood samples were collected and processed for malaria parasite detection, retroviral screening, glycated hemoglobin, and hemoglobinopathy. Data were analyzed using SPSS version 20. The strength of the association between independent and dependent variables was measured using odds ratio and 95% confidence interval with a significant level (p value <0.05).
Results:
The prevalence of malaria parasitemia was 63.3% (95% confidence interval: 57.9%–68.5%). Being a farmer (p = 0.002), lack of formal education (p = 0.043), low-income earners (p = 0.031), presence of bushes (p = 0.048), stagnant water (p = 0.042), not sleeping under long-lasting insecticide-treated nets (p < 0.001), and sickle cell disease (p = 0.041) were significantly associated with malaria infection.
Conclusion:
The study revealed that there is a high prevalence of malaria infection in rural Southwestern Nigeria. There may be a need to pay greater attention to adult populations in rural areas for malaria intervention and control programs.
Introduction
Malaria infection remains a global public health problem and a leading cause of morbidity worldwide.1,2 Malaria infection is spread through the bites of an infected female mosquito of the Anopheles. 2 Plasmodium falciparum is considered the most prevalent of all plasmodia in sub-Sahara Africa (SSA).2,3 Other malaria parasites causing disease in humans include Plasmodium vivax, Plasmodium malariae, and Plasmodium ovale. 3 Recent reports showed that globally, approximately 214 million cases of malaria occur per year and 3.2 billion people are at risk of the infection.1,2 Further reports also showed that in 2017, there were 438,000 deaths due to malaria globally. Out of these figures, about 93% occur in World Health Organization (WHO) African region, with Nigeria accounting for the highest burden of 19%.2,4 In Africa, malaria is responsible for about 20%–30% of hospital admissions and about 30%–50% of outpatient consultations. 5 Previous studies have documented a high prevalence of malaria throughout Nigeria.6,7 This devastating disease affects the country’s economic productivity, resulting in an estimated monetary loss of approximately 132 billion Naira (approximately US$700 million) in treatment costs, prevention, and other indirect costs. 8
The major clinical features of uncomplicated malaria include severe headache, fever, vomiting, loss of appetite, and generalized body weakness, while severe anemia, hypoxia, and cerebral malaria constitute the common complications in severe malaria. 9 Some of these clinical features are common in some patients with co-morbidities such as diabetes mellitus, uncontrolled hypertension, malignancies, HIV infection, hemoglobinopathy, and chronic kidney disease. 9
Although studies have shown that clinical immunity to malaria develops after exposure to parasites, at one stage in life, this immunity is only partial and may be influenced by some variations such as endemicity and other disease burdens.7,9 Evidence suggests that some co-morbidities exert a reasonable impact on a person’s immunity; therefore, factors that result in the development of partial immunity may not be adequate enough to guarantee such immunity against malaria infection.7,9
The major associated factors contributing to malaria transmission in SSA may include temperature, humidity, and rainfall.5–7 Other factors include socio-demographics (such as age, gender, education, occupation, income level, and location), environmental factors (such as presence of bushes and unblocking stagnant water channels) which may enhance mosquito breeding, and housing factors (such as bricks or mud houses, absence of window nets, and not sleeping under long-lasting insecticide nets (LLINs)).2,6 These factors have been well documented particularly in urban and semiurban communities in previous studies.2,10,11
In Southwestern and other parts of Nigeria, there are several approaches that have been recommended for the prevention and control of malaria in their localities.12,13 These include the use of LLINs, insecticide sprays, mosquito repellent creams, and window nets. In pregnant women, the use of intermittent preventive treatment and prompt access to effective case management have been included.13,14 Furthermore, community awareness, which is recognized as the cardinal tool currently used for malaria prevention strategy, is generally poor at preventing malaria cases in rural Nigeria. 14 However, education, behavioral change, and active practices regarding malaria prevention and control are well-documented and proven interventions.14,15 Behavioral change campaigns can increase demand among the families to use and hang their nets regularly and can improve malaria prevention and control, especially in rural settings.14–16
Since 2000 when Nigeria adopted some of these measures against malaria, several researchers have reported the low utilization of these strategies.12,13 A study in Southwestern Nigeria regarding the practice of malaria control in a specific area showed that the majority of respondents had household members who failed to use the control method appropriately.13,16 Available literature on the utilization and effectiveness of malaria prevention methods in health institutions in Nigeria has been restricted to urban settings.13–15 However, the effects of co-morbid conditions with regard to malaria transmission are rarely examined. Identifying key risk factors by socio-demographic context and incorporating the effect of preventive measures and co-morbid conditions are crucial for the effective implementation of prevention and health intervention programs. 17
Most efforts toward malaria prevention, management, and control are targeted under five children, pregnant women, and their unborn babies. Those in the older age groups are not adequately considered in most of these programs, amounting to some kind of obvious neglect in those of older age groups. To the best of our knowledge, there is an observed paucity of data on these factors and malaria parasite prevalence among adult patients in rural Southwestern Nigeria. This study is aimed to determine the prevalence of malaria infection and to investigate its association with socio-demographics, environmental, housing, and co-morbid ailment factors among adult febrile patients who presented to a tertiary health care facility in rural Southwestern Nigeria. This is with a view to designing and implementing appropriate effective control measures that would contribute to the global elimination of malaria infection in rural Southwestern Nigeria. Furthermore, a better understanding of the relationship between malaria infection and socio-demographic factors related to poverty is needed because the financial protection necessary to combat this menace is a major challenge for people in rural Southwestern Nigeria.12,14,18
Materials and methods
Study area: The study was carried out from May to July 2021 at the institution’s family medicine clinic. The study site is in a tropical rain forest in rural Southwestern with climatic and environmental conditions that support malaria transmission throughout the year. It has a total land area of 332 km2, and as of the last population census of 2006, it had a total population of 159,114 with an annual growth rate of 3.2%. 19 The inhabitants of the area are engaged majorly in farming and trading activities while few others in the formal sector are the working population and retirees. In the study area, malaria transmission occurs throughout the year. However, malaria peak season occurs during the wet season with P. falciparum being the major causative agent. 12 The institution offers secondary and tertiary care to the people in the locality and its neighborhood states. The institution was accredited for the training of resident doctors in family medicine and other core clinical specialties.
Study design: This was a hospital-based descriptive cross-sectional that was carried out from May to July 2021.
Study population: This comprised adult febrile patients aged 20 years and above and who presented to a family medicine clinic.
Inclusion criteria: This included consented adult febrile patients (with an axillary temperature ⩾37.5°C) and other clinical symptoms of malaria, whose ages were 20 years and above.
Exclusion criteria: Respondents who required urgent treatment or have a major psychiatric illness and could not follow the study protocol. Also, those currently on treatment for malaria or had just been treated for malaria within 3 weeks prior to the recruitment of this study.
Sample size determination: This was determined using the Araoye formula 20
where n = minimum sample size when the population (N) of the participants in the study area was greater than 10,000 over a period of 1 year and nf is the minimum sample size when the population (N) of the participants was less than 10,000. From the medical records of febrile patients with malaria, N was 3900 in 2019 and Z = 1.96%. Therefore, the minimum sample size nf was 314. To allow for unexpected data losses, an attrition of 5% was added and the sample size was 330.
Sampling technique: A systematic random sampling technique was used to recruit the 330 respondents who fulfilled the inclusion criteria. The medical record of patients with malaria parasitemia at the family medicine clinic showed that in the year 2019, an average of 15 patients were seen daily. This translated to 75 patients per week (Monday–Friday) and 975 (sample frame) patients over a period of 3 months (13 weeks) that the study was conducted. Using the formula, k = N/n, where k is the sample interval, N is the sample frame (975), and n represented the minimum sample size of 330. Therefore, k was approximately 3. The first respondent on each clinic day was chosen by simple random sampling and thereafter, every third respondent was chosen by systematic random sampling until the sample size of 330 is attained. A sticker was placed on each of the selected folder to avoid re-sampling at the subsequent clinics.
Ethical clearance and considerations
The Ethics and Research Committee of the institution approved the study (ERC/2020/08/25/402A). Information about the objectives and the procedure of the study was duly explained to the respondents after which they were made to sign a written informed consent. This was either by appending signature or thumb printing. An independent interpreter who served as legal guidance assisted those respondents who could not read or write to translate the questionnaire from English language to their local languages. Back translation to English language was subsequently done to maintain response consistency. The respondents were told that they were free to refuse or disengage participation at any time without losing any benefit of care or favor to those that participated. Confidentiality and privacy were ensured throughout the study. The study was at no cost to the respondents. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 22 All patients’ details have been de-identified.
Recruitment procedure: The data were collected using a pretested standardized semistructured interviewer-administered questionnaire which was developed by the researchers. The questionnaire was pretested on 25 adult febrile patients, who presented at the family medicine clinic of a tertiary hospital which is located at about 30 km from the study center. The pretesting that lasted 3 days was to show how applicable the questionnaire was and its feasibility. The questionnaire was modified to address the challenge(s) that were observed in the pretest and validity assessment. The time taken to complete the questionnaire was about 10 min.
Data collection instruments: Data were collected using the standardized interviewer-administered questionnaire and a data collection form. The questionnaire sought information about the respondents’ socio-demographic characteristics (such as age, gender, education, occupation, income level, and location), environmental factors (such as the presence of bushes and unblocking stagnant water channels), and housing factors (such as bricks or mud houses, use of window nets, and sleeping under the LLINs). Other data were collected through screening for the following co-morbidities; hypertension, diabetes mellitus, hemoglobin type abnormality, and human immunodeficiency virus (HIV 1 and 2).
Clinical parameters of the respondents
(a) Blood pressure (BP): Using a good Accosson brand of mercury sphygmomanometer, a senior resident doctor in the department measured the blood pressure of the respondents twice after about 5 min apart. The mean BP of ⩾140/90 mmHg was considered as hypertension or self-reported treatment of hypertension with antihypertensive medication taken in the previous 2 weeks. 23
(b) Sample collection: By means of the intravenous route, about 10 mL of blood samples of the respondents was obtained with the assistance of a hospital phlebotomist. The blood samples were transferred into an ethylenediaminetetraacetic acid (EDTA) bottle to prevent blood coagulation.
Microscopy: The blood films (thin and thick) for malaria parasitemia were prepared on clean, dry microscope glass slides and were allowed to dry. The thin smear was fixed in methanol and both smears were stained with 2% Giemsa BDH Laboratory supplies; Poole BH 15 ITD England. 24 The microscopy was used to view the slides at 100× magnification. The staining, counting, and grading of the parasite density were done in accordance with the authorized standard operating procedure for thin and thick films. 24 A senior scientist was recruited to examine the slide for quality control. 24
Glycated hemoglobin (HbAIc): Using a sample of blood collected, HbAIc was determined immunochemically on DCA 2000; HbAIc autoanalyzer using kits supplied by the Boehringer Mannheim (Germany) autoanalyzer. 25 Accuracy of the test result was ensured using commercially prepared standards and control samples. HbAIc ⩾6.5% was recorded as undiagnosed diabetes mellitus. 26
HIV screening: Two-step algorithms were used in performing the HIV screening test. DetermineTM (Abbott Laboratories, IL, USA) HIV reagent was used to screen all specimens. Non-reactive samples were reported as HIV negative. Reactive samples were confirmed using STAT PAKTM 1 and 2 test kit (Chembio Diagnostic System Inc., USA), and specimens in the STAT PAKTM test were reported as positive for HIV 1, HIV 2, or both. 27 Specimen positive in DetermineTM and negative in STAT PAKTM were reported as discordant. The true sero-status of each of these samples was determined using Enzyme-Linked Immuno-Sorbent Assay (ELISA) and Polymerase Chain Reaction (PCR) at the laboratory department.
Determination of abnormal genotype: The genotype of each respondent was determined as described by Ochei and Kolhatkar. 28 About 1 ml of blood samples were withdrawn from the EDTA bottle and centrifuged at 2500 r/min for 5 min. The supernatant was then discarded and packed cells were washed with normal saline three times. The red cells were lysed by adding an equal volume of distilled water and one-quarter (1/4) of toluene followed by a drop of 3% KCN after the final wash. It was then mixed properly. The respondents who had abnormal hemoglobin genotype (SS or SC) were recorded as having co-morbidity.
Treatment of the respondents
All malaria-positive individuals were arranged to see their clinician where they were treated with the standard medication according to the national malaria drug policy. Also, respondents identified with co-morbidity were counseled by a principal investigator, a physician, on lifestyle modification and treatment compliance. They were thereafter scheduled for follow-up in line with the hospital protocols on the management of co-morbid ailments
Some definitions
For the definition of socio-demographic, environmental, and housing factors, see our supplementary material.29,30
Statistical analysis: Data collected were checked, cleaned, and entered into EPI Info Version 7.0 and were exported to SPSS version 22.0 for analysis. Bivariate analysis was conducted to ascertain the prevalence of malaria compared to socio-demographic factors, the prevention methods, and the co-morbid conditions of the respondents. The chi-square test of independence at p value < 0.05 was explored to assess any significant association between malaria parasitemia test results and socio-demographics, prevention methods, and co-morbid conditions in terms of p value. Based on significant association with the results, variables were chosen for the multivariate analysis. 31 The multiple logistic regression model was chosen to identify the significant determinants for malaria, and the results were presented in terms of adjusted odds ratios (AORs) that controlled for multiple confounders (with 95% confidence interval). A multiple logistic regression was explored in the analysis of these data because the outcome variable has a binary response of malaria positive or negative results. This outcome variable was re-coded as “0” for respondents who did not have malaria and “1” for those who had malaria. Both AORs and p value <0.05 were considered for finding the single and covariates effects in the model. 17
Results
A total of 330 respondents were screened during the study period. The distribution according to socio-demographic characteristics showed that the majority of the respondents 130 (39.4%) were young adults within the ages of 21–40 years. The mean age of the respondents was 45.9 ± 19.9 years (range: 21–88 years). There were more males (201, 60.9%) than females (129, 39.1%). Many of the respondents were farmers 90 (27.3%), and the majority had formal education 298 (90.3%), were rural dwellers 196 (59.4%), and were of low-income earners 196 (59.4%), Table 1.
Socio-demographic characteristics of respondents.

The prevalence of malaria parasitemia was 63.3% (Table 2).
Prevalence of malaria parasitemia the respondents.

There was no statistically significant association between the respondents’ ages and malaria infection. The results showed that the majority 88 (67.7%) of respondents who tested positive for malaria infection were young adults between the ages of 20 and 39 years (Chi-square (χ2) = 2.388; p = 0.303). However, a statistically significant association was observed between malaria infection and the occupation of respondents (χ2 = 76.734, p < 0.001). The results showed that those who were unemployed had the highest prevalence (96.0%). Also, the majority of the respondents who had no formal education 27 (84.4%) tested positive for malaria and a significant association was found between malaria parasitemia and level of education (χ2 = 6.756; p = 0.009). Furthermore, a significant association was found between malaria infection and respondents’ level of income (χ2 = 19.445; p < 0.001). The results showed that respondents with low income had the highest percentage (176, 69.8%; Table 3).
Association between socio-demographic characteristics and malaria parasitemia in the respondents (N = 330).

In the same vein, a significant association was found between malaria infection and the vegetation around the respondent houses (χ2 = 9.089; p < 0.003). The results showed that the respondents whose houses were surrounded by bushes had the highest prevalence (72.5%). Similarly, there was a statistically significant difference between malaria infection and having stagnant water around the respondents’ houses (χ2 = 5.561; p < 0.018). The results showed that respondents whose houses were surrounded by stagnant water had the highest prevalence (70.3%). Also, there was a statistically significant difference between malaria infection and the respondents’ attitude to the use of LLINs (χ2 = 34.803, p < 0.001). The results showed that respondents who did not sleep under LLINs had the highest prevalence (72.9%) (Table 4).
Association between environmental/home factors and malaria parasitemia in respondents (N = 330).

ITNs: insecticide-treated nets.
Similarly, among the 330 respondents who were screened, 66 (20.0%) had co-morbidity. There was a statistically significant difference between the prevalence of malaria infection and the type of co-morbid ailments in the respondents, (χ2 = 8.493, p = 0. 037). The results showed that respondents who harbored HIV/AIDS and sickle cell disease were observed to have higher prevalence of 64.3% and 66.7%, respectively. Table 5.
Association between co-morbid ailments and malaria parasitemia in the respondents (N = 330).

The multivariate logistic regression model showed that the respondents who were farmers were 5.009 times more likely to have malaria infection as compared to the respondents who were civil servants (AOR = 5.009; p = 0.002). The analysis of odds ratios also verified that the respondents who had no formal education (AOR = 3.179; p = 0.043) were more prone to have malaria than those with formal education. Similarly, the respondents who were of lower income were 2.311 times more likely to have malaria infection (AOR = 2.311; p = 0.031) than those with higher income. With regard to prevention against malaria infection, the respondents whose houses were surrounded by bushes (AOR = 2.848; p = 0.048) and stagnant water (AOR = 2.986; p = 0.042) were more susceptible to malaria compared to their counterparts whose houses were not surrounded by bushes and stagnant water, respectively. It was also found that the probability of having malaria was more likely among the respondents who did not sleep under LLINs (AOR = 3.697; p < 0.001), as compared to the respondents who slept under LLINs. Furthermore, the results also showed that the respondents who had sickle cell disease (AOR = 8.00; p = 0.041) were more prone to have malaria compared to the respondents who were hypertension (Table 6).
Multivariate logistic regression model for factors that were significantly associated with malaria parasitemia.
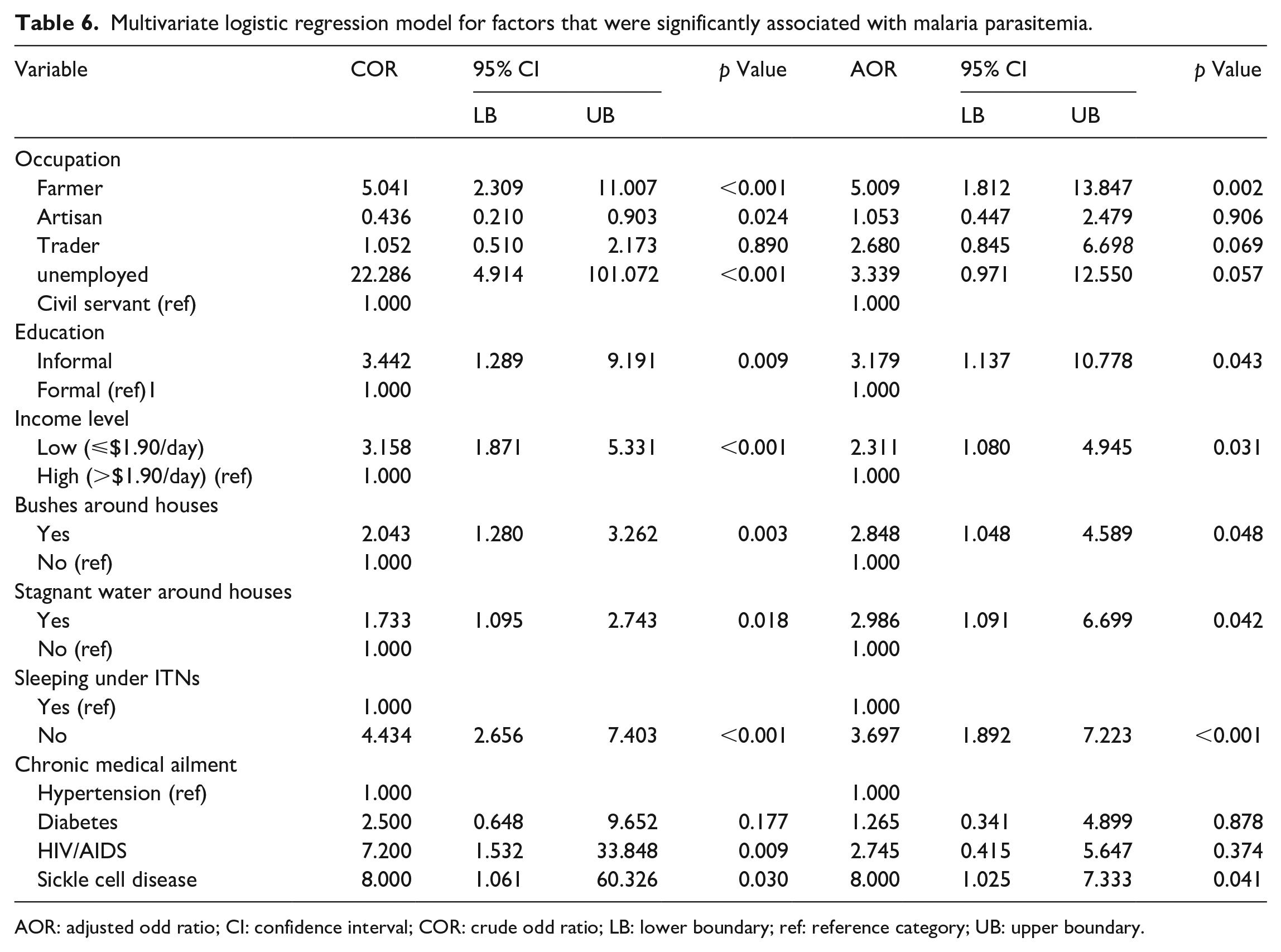
AOR: adjusted odd ratio; CI: confidence interval; COR: crude odd ratio; LB: lower boundary; ref: reference category; UB: upper boundary.
Discussion
The study revealed an overall prevalence of 63.3% of malaria infections among adult febrile patients attending a tertiary health care facility in rural Southwestern Nigeria. This is consistent with previous studies conducted in other parts of rural Nigeria.21,32 The relatively high prevalence of malaria infection reported in this study might relate to the prevailing study duration, climatic, and environmental conditions that support the breeding of the vector of the parasite. This study was conducted during the peaks of wet season. Our finding was higher than the reported prevalence of 35.7% found among patients in Kaduna, Northwestern Nigeria, and 36.6% found among patients in Plateau, Northern-central Nigeria.33,34 However, a study carried out across the six geopolitical regions of the country in 2010 concluded that the prevalence of malaria was higher in Southwestern Nigeria compared to Northern Nigeria. 35 This variation may be due to differences in locations, climatic conditions, and environmental factors. 21 The finding in this study showed that the prevalence of malaria infection across the different age groups is of major concern, though, not statistically significant. The results suggest that if the retirement age within the study location is set at 60 years, then, at any given time, the majority (67.7% for ages 21–40 and 58.4% for ages 41–60) of the active workforce suffers from malaria infection. The overall effect may result in reducing their efficiency and contributing to their low productivity. These findings revealed that malaria continues to be a leading cause of morbidity and mortality in rural settings. Therefore, innovative and effective interventions to control malaria should be identified and implemented in this community. 21
The findings in this study revealed that farming increased the odds of malaria infection among the studied population. This is consistent with the reports of other studies.10,36 This could be due to the fact that farming enhances human-vector contact.10,36 Besides, many farmers have keyed into some water-related projects involving the creation of reservoirs for the purpose of irrigating farms to improve their yields. Despite the economic significance of these projects, these reservoirs also serve as a breeding ground for mosquitoes to thrive. 36
The lack of formal education was found to contribute to a higher risk of malaria among the studied population. This is consistent with previous reports in Nigeria that showed that malaria is more common among people with low literacy.17,37 This may be due to lack of information and ignorance of the preventive measures among these sets of patients. Even, when they are aware of the preventive measures and their interventions, they may be unable to implement and manage them appropriately.17,37 The lack of education may also influence other variables like income and occupation which were also associated with malaria risk.
In the same vein, low-income earners doubled the odds of malaria among this population. This is consistent with previous reports from other studies in Nigeria that showed that malaria is more common among people of lower socio-economic status.21,38 Malaria and poverty are mutually inclusive as malaria is reported to be common in developing countries.21,38,39 This may be due to their poor housing and environmental factors that increase their exposure to frequent mosquito bites.21,38 Other studies have attributed low socioeconomic factors to poor access to quality health care services for prevention, diagnosis, and treatment.21,40 Despite the high LLINs distribution, low socioeconomic factor at both the community and household levels was a significant risk factor for malaria infection in rural Northwestern Tanzania. 39
Higher prevalence was also found among the respondents whose houses were surrounded by bushes and stagnant water. These findings were consistent with data obtained from various studies in Nigeria and other SSA.10,21,38 The bushes and stagnant water have been found in previous studies to be reservoirs of breeding grounds for mosquitoes, thereby enhancing human–vector contact.10,36 These findings suggest that effective environmental sanitation, geared toward the clearing of bushes and gutters should be intensified. This intervention may reduce the spread of mosquitoes, thereby reducing the incidence of malaria in rural settings.21,38
Similar to other studies, this study also revealed that failure to use LLINs was found to be associated with increased malaria infection. This is consistent with previous studies in Nigeria.21,41 The use of LLINs is considered one of the most cost-effective interventions against malaria in endemic areas and is associated with a significant reduction in malaria morbidity and mortality. 10 Despite the high number of respondents in this study who possessed LLINs (57.0%), only half of the respondents (27.3%) stated that they used them. This poor utilization is consistent with previous studies in Nigeria10,21,42 and other SSA countries.17,43 A report from a national study in Nigeria revealed an observed gap between ownership and use of LLINs and revealed that only 28.7% of the population had one LLIN in the household. 44 Considering the role of LLINs against the spread of malaria infection in endemic areas, the findings of this study call for regular and sustained distribution of free LLINs in this rural community to reduce the incidence of malaria infection.
In this study, HIV/AIDS has no significant association with malaria infection. This finding was opposite to the reports of other studies that found a significant association between HIV/AIDS and malaria infection.45,46 Therefore, further research is recommended to identify the magnitude of association between malaria infection and HIV/AIDS in SSA to fully understand the relevance and cause of these findings.
In addition, hemoglobin sickle cell disease respondents were found to be significantly associated with malaria infection in this study. This is consistent with reports of other studies.6,47 The increased odds of malaria infection among these respondents may be due to their weak immunity and improper use of recommended interventions against malaria. 42 However, a study by Suchdev et al. in Kenya found no significant association between malaria infection and respondents with sickle cell diseases. 48
Finally, in view of the above findings on factors that were significantly associated with the risk of malaria infection in this study, the government should provide awareness to rural dwellers on how to identify and remove mosquito-breeding sites within their locations from time to time. Also, government should make available the distribution of additional free mosquito bed nets and fumigation while also enforcing the available law on frequent public sanitation.
Limitations
First, the cross-sectional nature of the study design does not allow ascertaining the causal association between the outcome variables and potential contributing factors. Multivariate analysis cannot exclude unmeasured confounders, and association does not mean causality. Information collected from the respondents was self-reported and might be subjective by recall bias when highlighting the association between malaria infection and socio-demographics and preventive methods adopted. Also, exposure to malaria infection might still have differed among the studied population considering the endemic malaria transmission in rural Southwestern Nigeria. Therefore, ultimate corroboration would need a prospective longitudinal study controlling for exposure. Despite these limitations, the study generates distinctive information regarding factors that were significantly associated with malaria infection in rural Southwestern Nigeria. These findings may be helpful to formulate further strategies for malaria intervention.
Conclusion
The study revealed that there is a high prevalence of malaria infection in rural Southwestern Nigeria. Being a farmer, lack of formal education, presence of bushes and stagnant water around the houses, low-income earners, not sleeping under LLINs, and genotype SS were the significant factors associated with malaria infection in this study. There may be a need to pay greater attention to the adult population living in rural areas for malaria intervention and control programs. The findings of this study would assist the stakeholders in decision-making toward improved malaria preventions and control.
Supplemental Material
sj-doc-2-smo-10.1177_20503121221117853 – Supplemental material for Malaria infection and its association with socio-demographics, preventive measures, and co-morbid ailments among adult febrile patients in rural Southwestern Nigeria: A cross-sectional study
Supplemental material, sj-doc-2-smo-10.1177_20503121221117853 for Malaria infection and its association with socio-demographics, preventive measures, and co-morbid ailments among adult febrile patients in rural Southwestern Nigeria: A cross-sectional study by Azeez Oyemomi Ibrahim, Ibrahim Sebutu Bello, Olabode Muftau Shabi, Adejumoke Oluwatosin Omonijo, Abayomi Ayodapo and Babatunde Adeola Afolabi in SAGE Open Medicine
Supplemental Material
sj-docx-1-smo-10.1177_20503121221117853 – Supplemental material for Malaria infection and its association with socio-demographics, preventive measures, and co-morbid ailments among adult febrile patients in rural Southwestern Nigeria: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221117853 for Malaria infection and its association with socio-demographics, preventive measures, and co-morbid ailments among adult febrile patients in rural Southwestern Nigeria: A cross-sectional study by Azeez Oyemomi Ibrahim, Ibrahim Sebutu Bello, Olabode Muftau Shabi, Adejumoke Oluwatosin Omonijo, Abayomi Ayodapo and Babatunde Adeola Afolabi in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to appreciate nurses and resident doctors of family medicine department and the management of institution where the study was conducted.
Authors’ contribution
A.O.I.—Conceived and designed the study, data acquisition, processing, coding, and interpretation of findings.
I.S.B.—Data processing, analysis, and review of manuscript for intellectual content.
O.M.S.—Prepared the manuscript, data analysis, and interpretation of findings.
A.O.O.—Literature review and data curation.
B.A.A.—Data acquisition and review of the manuscript for intellectual content.
A.A.—Data processing, literature review, and review of the manuscript for intellectual context.
All authors have read and approved the final version of the manuscript prior to submission.
Availability of data and materials
The datasets for this study would be made available from the correspondence author on a reasonable request
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval/patient consent
Ethical approval for the study was received from the Ethics and Research Committee of Federal Teaching Hospital Ido-Ekiti (ERC/2020/08/25/402A). All consented patients were thoroughly informed about the risks and advantages of the procedures. Written informed consent for the procedure and treatment was obtained from each respondent, and participation was fully based on their willingness. Confidentiality and privacy were ensured throughout the study. The study was at no cost to the respondents. The reporting of this study conforms to the Strengthening the Reporting of observational Study Studies in Epidemiology (STROBE) statement. All patients’ details have been de-identified.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.