
Abstract
Introduction:
Globally, hypertension is an important risk factor for cardiovascular diseases and all-cause mortality. Despite this high public health burden, no community-based evidence regarding the magnitude and related factors of hypertension has been reported in the study area.
Objective:
The aim of this study was to determine the prevalence and associated factors of undiagnosed hypertension in Debre Markos town, North-West Ethiopia, 2020.
Method:
A community-based cross- sectional study design was conducted from January to March 2020. Socio-demographic and behavioral characteristics of the participants were collected using interviewer-administered semi-structured questionnaires. Physical measurements including body mass index, waist circumference, and blood pressure were collected using standardized measuring instruments. Statistical analysis was collected using SPSS version 21 software. Univariate logistic regression model was used to present the results. The p value less than 0.05 in a multivariable analysis was considered statistically significant at 95% confidence interval.
Results:
From a total of 630 samples, 600 participants, 270 (45%) males and 330 (55%) females with a mean age of 36.32 ± 12.48 years, were participated giving a response rate of 95.2%. The prevalence of undiagnosed hypertension among adults was 12.7%. Of these, 5.5% were males and 7.2% were females. Factors including age (above 60 years) (adjusted odds ratio = 2.92, 95% confidence interval (1.05, 8.06), p = 0.03), body mass index (overweight and obese) (adjusted odds ratio = 3.85, 95% confidence interval (2.16, 6.87), p < 0.01), fatty diet consumption (adjusted odds ratio = 1.88, 95% confidence interval (1.03, 3.42), p = 0.04), family history of hypertension (adjusted odds ratio = 2.21, 95% confidence interval (1.04, 4.69), p = 0.04) were significantly associated with hypertension.
Conclusion:
The prevalence of undiagnosed hypertension among adults was found to be remarkable. Therefore, a community-based health education and hypertension screening strategies are needed to prevent the problem early in life in Debre Markos town and the nation at large.
Introduction
Non-communicable diseases (NCDs) are globally recognized as the threats to socioeconomic developments. 1 NCDs accounted for 72.3% of the global deaths in 2016, of which more than 50% of the deaths were attributed by the cardiovascular problems. 2 NCDs are the new priorities and additional burdens on health in low- and middle-income countries, where urbanization and lifestyle changes are advancing rapidly. 3 Undiagnosed hypertension, which is one component of NCD, is defined as individuals who were hypertensive but did not report having been told by a health professional that they have hypertension. It is an important risk factor for the development of chronic kidney disease, cardiovascular disease, and all-cause mortality. 4 Hypertension is a major cardiovascular risk factor that is closely associated with lethal complications like coronary artery disease, cerebrovascular accidents, heart, and renal failure. 5 There is a declining trend of cardiovascular diseases in developed world due to the effective intervention strategies but the burden is rising in the developing countries. 6 According to World Health Organization (WHO), 2017 report, 40 million deaths were reported due to NCD. Of this, 28 million deaths were in low- and middle-income countries. Globally blood pressure (BP) is the leading metabolic risk factor in terms of attributable deaths accounting for 18%, followed by overweight and obesity and raised blood glucose. 7 About 62% of cerebrovascular diseases and 49% of ischemic heart disease were attributable to elevated BP that could have been reduced by antihypertensive drug therapy. 8
Undiagnosed hypertension increases the risk of complications such as renal failure, myocardial infarction, heart failure, stroke, and premature death. 9 About 75% of people with hypertension live in low- and middle-income countries. People in such settings often have low awareness related to hypertension, its treatment, and control measures. 10 This may lead to low healthcare-seeking behavior, which in turn results in a high prevalence of undiagnosed hypertension in these populations. In sub-Saharan Africa, the prevalence of undiagnosed hypertension was 30%. Of those with hypertension, 73% were unaware of their hypertension; only 18% received treatment and 7% had a controlled BP measurement. 11 Studies indicated that the disease has become a significant public health problem especially in the major cities of Ethiopia. Study conducted in Southern Ethiopia indicating that the prevalence of undiagnosed hypertension was 12.3%. 12 In Gulele Sub-city, Addis Ababa, Ethiopia, the prevalence was 13.3%. 13 Study conducted in Gondar, Northern Ethiopia, indicate that, among people with hypertension, 37.0% did not know that they had the diseases. 14 Therefore, in order to alleviate such catastrophic public health burden among the community members, providing epidemiological data about the prevalence and associated factors of undiagnosed hypertension is very crucial. This will pave the way for the responsible stockholders to prevent the burden early in life. So, this community-based study was conducted to determine the magnitude and associated factors of undiagnosed hypertension among adults in Debre Markos town, North-West Ethiopia, 2020.
Methods
Study setting
The study was conducted in Debre Marko town, North-West Ethiopia from January to March 2020. Debre Markos town is the capital city of East Gojjam Administrative Zone which is located 300 km form Addis Ababa, the capital city of Ethiopia and 265 km Southwest of Bahir Dar, the capital city of Amhara Regional State.
Study design and population
A community-based cross-sectional study design with a random sampling technique was employed. All adult population living in the study area were the source population, while those with the age range of 18 to 70 years who have been living in the study area for at least 6 months and above were the study population. Those with known chronic diseases, mental illness, seriously ill, and pregnant women were excluded from the study. The sample size was calculated using single population proportion formula by considering the prevalence of undiagnosed hypertension in Bahir Dar, 4 P = 24.8%, margin of error = 5% with a design effect of 2

where n = sample size; P = prevalence of undiagnosed hypertension; d = margin of error; Za/2 = 1.96 (CI).
By adding 10% non-response rate, the final sample size was determined to be 630.
Data collection tools and procedures
After determining the sample size, a multistage random sampling technique was employed to recruit the study participants. Among 11 kebeles in the town, 3 were selected randomly. Then the total sample size was distributed to each selected kebele based on the number of households. After that households were selected from the kebeles by employing a systematic random sampling technique using the household folder located at the health center as a sampling frame. Finally, after determining the number of households, one eligible family member from the household was selected using a lottery method. Six health extension workers were participated in the data collection process and two BSc degree public health officers were supervising the data collection process. The survey instrument was adapted from WHO STEP-wise approach surveillance instrument (version 3). Socio-demographic characteristics (age, sex, educational status, marital status, income) and behavioral characteristics (cigarette smoking, alcohol drinking, and khat consumption) were assessed using the survey instruments. First, the tools were prepared in English language and then translated into Amharic version (the Country’s national language) for easy understanding and retranslated to English for analysis. The tools were pretested before undergoing the actual data collection. Then interviewer-administered face-to-face interview process was conducted to collect the data. After completing the interview, body mass index (BMI) (weight, height) waist circumference and BP were measured using standardized and calibrated measuring instruments. The instrument was checked and adjusted to zero levels for each measurement. Weight was measured using an electronic scale (balance). Height was measured in the standing position. BP was measured two times in a sitting position using a standard mercury sphygmomanometer. Five minutes of rest was given for the participants between the consecutive measurements of BP. The measurement was taken after confirming that the study participant had not smoked or drunk any caffeinated beverage within 30 min before measuring the BP. The average of the two BP measurements was calculated to determine the BP of each study participants.
Statistical analysis
Data entry and analysis were performed using SPSS version 21 software. Descriptive statistics were computed to present frequency distributions. Univariate logistic regression analysis was carried out to identify candidate variables for multivariable logistic regression analysis. All factors with a p value of ⩽0.25 in a univariate logistic regression analysis were included in the multivariable model. A multivariable logistic regression model was used to identify the independent predictors of undiagnosed hypertension. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated. A p value less than 0.05 was considered statistically significant at 95% CI level.
Operational definition
Undiagnosed hypertension: a person having a systolic blood pressure (SBP) of at least 140 mm Hg and/or diastolic pressure (DBP) of at least 90 mm Hg, which was not diagnosed.
Khat chewing: regular chewing of khat for at least 1 year before we conducted the survey.
“Current alcohol users”: who drink alcohol within 30 days preceding the study. 15
Heavy episodic drinking: consumption of ⩾6 drinks and ⩾4 drinks on a single occasion in men and women, respectively. 15
Results
In this study, the overall prevalence of undiagnosed hypertension among adults was 12.7%. Of these, 7.2% were females and 5.5% of them were males.
Socio-demographic characteristics
Out of 630 samples, 600 participants had participated in this study giving a response rate of 95.2%. Of these, 330 (55%) were females and 270 (45%) of them were males. The mean age of the participants was 36.32 ± 12.48 SD years. Majority of them, 439 (73.2%), were below 41 years. Regarding the marital status, most of them, 364 (60.7%), were married individuals. The detailed socio-demographic characteristics of the study participants are indicated in Table 1.
Socio-demographic characteristics among 600 adults in Debre Markos town, North-West Ethiopia, 2020.
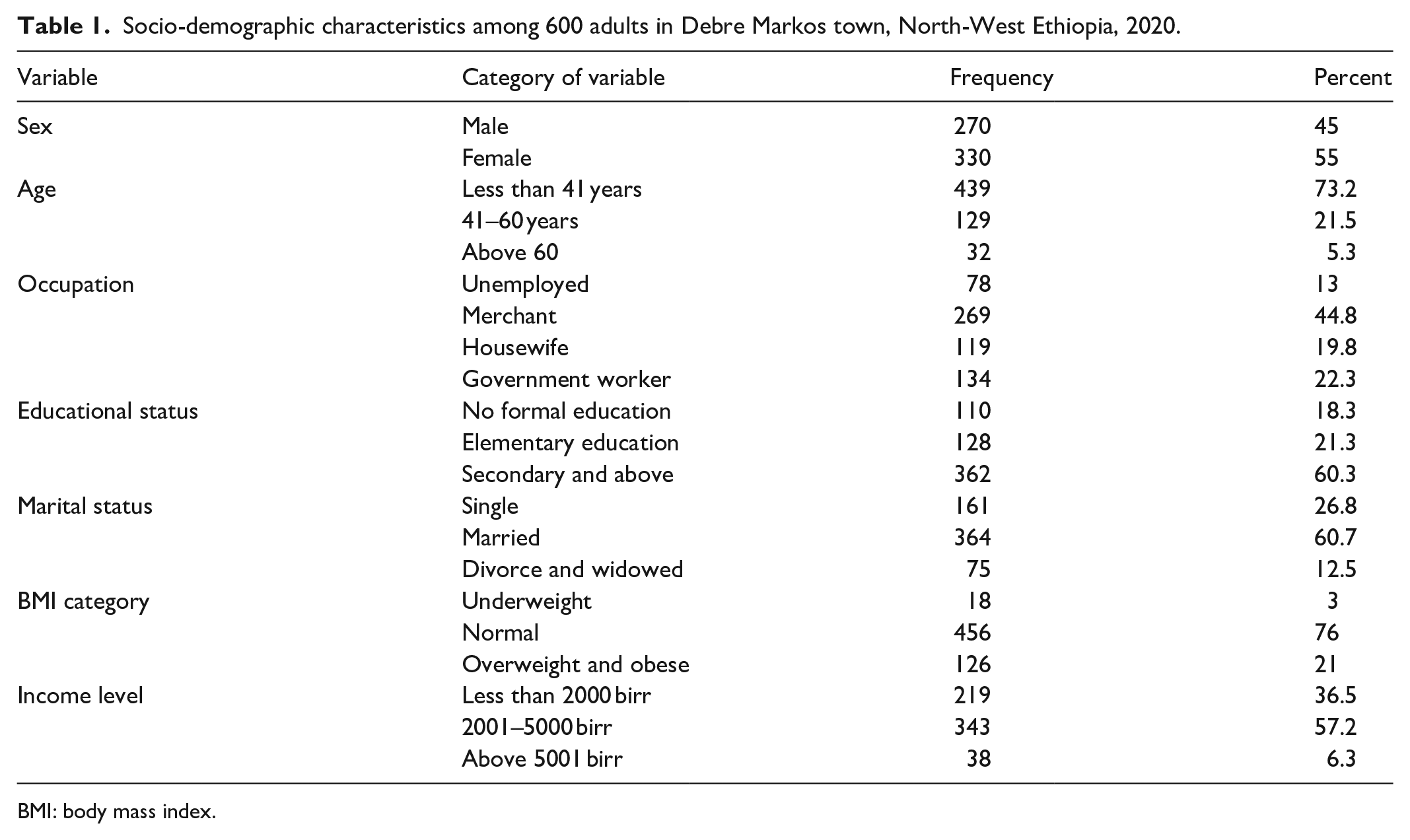
BMI: body mass index.
Behavioral factors
Behavioral factors including alcohol intake, cigarette smoking, trend of BP checkup, khat consumption, and BMI status were assessed. Based on this, majority of the participants, 345 (57.5%) consumed alcohol sometimes, about 100 (16.7%) had a history of regular BP checkup; majority of them, 567 (94.7%), had no regular physical exercise, 110 (18.3%) were overweight, and 16 (2.7%) were obese participants. The detailed behavioral information of the participants is indicated in Table 2.
Frequency distributions of behavioral and other related factors among 600 adults in Debre Markos town, North-West Ethiopia, 2020.

DM: diabetes mellitus.
Factors associated with hypertension
Factors in univariate analysis with a p value of
Bivariate analysis multivariate analysis of factors associated with hypertension among 600 adults in Debre Markos Town, North-West Ethiopia, 2020.

COR: crude odds ratio; AOR: adjusted odds ratio; LCL: lower confidence level; UCL: upper confidence level; BMI: body mass index.
Significant at 95% CI; **highly significant at 95% CI.
Discussion
The overall prevalence of undiagnosed hypertension among adults in this study was 12.7%. This was similar to the study conducted in Hawassa, Southern Ethiopia, 12.3%. 12 But the prevalence of our study was relatively higher than study done in Hosanna, Southern Ethiopia, 10.2%; 16 in India, 10.1%; 17 in Iran, 4.8%; 18 and in Saudi Arabia, 2.8%. 19 This may be due to the lack of community-based hypertension screening and prevention strategies in our study area so that the burden of hypertension remained remarkable. The prevalence of this study was lower than study done in Addis Ababa, Ethiopia, 13.25%; 13 in Bahir Dar, North-West Ethiopia, 4.8%; 4 South-West Ethiopia 21.2%; 20 in Sudan 38.2%; 21 and in Saudi Arabia 57.8%. 22 This might be due to the difference in the study settings and sociocultural difference. For example, in Addis Ababa and Bahir Dar City, since the two cities are more developed and civilized, the communities are exposed to sedentary lifestyles with limited physical activity. This may contribute for developing hypertension among the community members. The prevalence in our study was significantly lower than in Sudan. This may be due to the socioeconomic and sociocultural difference which contributes a significant role in hypertension development.
Our study revealed that more females were affected by undiagnosed hypertension than males which was supported by a study done in Saudi Arabia. 22 However, this study was in contrast to the study conducted in Bahir Dar, Ethiopia, in which males were more likely to have undiagnosed hypertension than females. 4 So, we highly recommend more research to be conducted to prove these discrepancies. Factors including age (above 60 years), BMI (overweight and obese), frequent consumption of fatty diet, and family history of hypertension were significantly associated with hypertension in multivariable analysis. Participants above 60 years were 2.92 times more likely to develop hypertension than those with the age below 41 years (AOR = 2.92, 95% CI (1.05, 8.06), p = 0.03). Similar study was conducted in Bahir Dar, in which age was one risk factor for hypertension and increasing age is significantly associated with hypertension development. 4 BMI as a risk factor, overweight and obese individuals, had 3.85 times more chance of developing hypertension than underweight or normal individuals (AOR = 3.85, 95% CI (2.16, 6.87), p < 0.01). This was similar to studies conducted in India and Bangladesh in which the occurrence of newly diagnosed hypertension is directly related to an increasing BMI.23,24 This might be due to increasing access to high-calorie, refined energy-dense food, and economic growth may explain the clustering of overweight and obesity compared to others which may contribute a newonset hypertension. In this study, participants who frequently consumed fatty diet were 1.88 times more likely to develop hypertension than non-consumers or those individuals who sometimes consume fat (AOR = 1.88, 95% CI (1.03, 3.42), p = 0.04), which was in line with a meta-analysis study which indicated that high fat consumption was significantly associated with the increased risk of developing hypertension. 25 Participants with a family history of hypertension had 2.2 times more chance of developing hypertension than their counterparts (AOR = 2.21, 95% CI (1.04, 4.69), p = 0.04). This was in line with the study conducted in Sri Lanka which indicated that the prevalence of hypertension was significantly higher in patients with a family history of hypertension. 26
Limitation of the study
One of the limitations of our study was the study design which was cross-sectional in which data were collected at a point of time so that identification of the risk factors is relatively weak for these chronic diseases. Reporting bias from the participants might be the other limitation of our study. Due to time and resource limitations, all possible factors responsible for hypertension were not collected and analyzed.
Conclusion
The prevalence of undiagnosed hypertension in this study among adults was remarkable. Factors including age, BMI, family history, and fatty diet consumption were significantly associated with the development of hypertension. This finding was an alarm to the government and the responsible stockholders to design a kind of public health intervention like community-based screening and education programs.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221094223 – Supplemental material for Undiagnosed hypertension and associated factors among adults in Debre Markos town, North-West Ethiopia: A community-based cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221094223 for Undiagnosed hypertension and associated factors among adults in Debre Markos town, North-West Ethiopia: A community-based cross-sectional study by Enatnesh Essa, Dessalegn Shitie, Mesenbet Terefe Yirsaw and Mengistu Zelalem Wale in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge Debre Markos University for sponsoring to conduct this study. We would also like to thank all the study participants for their voluntary participation. Finally, we would like to thank all the co-authors for their active and incredible participation starting from data collection up to the write-up of the manuscript.
Author contributions
EE involved in data collection. MZW, MTY, EE, and DS involved in conceptualization and data curation. MZW and MTY involved in methodology development and formal analysis. EE, DS, and MZW involved in writing the original draft of the manuscript.
Data availability
All the important information regarding the article is included in the submission process. If you need further information, we can provide the data without restriction.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical consideration
Ethical clearance was obtained from ethical review committee of School of Medicine, Debre Markos University, and official permission was obtained from Debre Markos town administration office. The results of this study were kept confidential and used only for research purpose. There was no any harm or discomfort to the participants. After exampling the purpose of the study, verbal informed consent was obtained.
Ethical approval
Ethical clearance was obtained from Ethical Review Committee of Debre Markos University School of Medicine with an approval number of
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was sponsored by Debre Markos University, Ethiopia.
Informed consent
After information was provided about the objectives and importance of the study, verbal informed consent was obtained from the participants. Since the study was conducted using questionnaires/no any clinical trial was involved/only verbal informed consent was obtained. All these procedures were approved by the review committee of School of Medicine, Debre Markos University. No minor subjects were involved in our study so that written consent was not applicable from legally authorized representatives.
Trial registration
Trial registration was not applicable for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.