
Abstract
Objectives:
The main objectives of this article were to answer (1) what is the trend of under-5 mortality from 2000 to 2016 Ethiopian Demographic and Health Survey? (2) What are the correlates that contribute to under-5 mortality in Ethiopia?
Methods:
The data used in this study were obtained from 2000, 2005, 2011, and 2016 Ethiopian Demographic and Health Survey data. We used multivariable three-level logistic regression model to predict under-5 mortality, with sex of a child, preceding birth interval, birth order, place of delivery, weight of child at birth, and plurality as first-level variables; mother’s education level, wealth index, mother’s age at first birth, and sex of household head as second-level variables; and residence and survey time as third-level variables.
Results:
The under-5 mortality declined from 166 deaths per 1000 live birth in 2000 to 67 deaths per 1000 live births in 2016. The odds of under-5 mortality among children with rural residence were 2.81 times greater than among children with urban residence. Moreover, the odds of under-5 mortality were higher among mothers who gave birth with preceding birth intervals of less than 24 months. A child whose preceding birth interval was less than 24 months had a 0.235, 0.174, 0.143, and 0.107 predicted probability of dying in the years 2000, 2005, 2011, and 2016, respectively.
Conclusion:
Child mortality varied across time in Ethiopia. Understanding both the time-varying nature of the correlates and changes in the type of their associations can help to explain some of the decreases in child mortality rates. Direction and/or presence of a relationship between these correlates and child mortality significantly interacted with time. Therefore, to mitigate the burden of under-5 mortality, the concerned body should provide awareness to the community.
Introduction
Under-5 mortality (U5M) rates refer to the probability of a child born in a specific year or period dying before reaching 5 years of age expressed per 1000 live births. 1 According to a 2019 report, 5.8 million children died worldwide in their first 5 years. 2 Even if it decreased by more than half since 1990, still it is unacceptably large. 3 In sub-Saharan Africa and southern Asia, the U5M rate remains high. 4 Most of these deaths are due to stoppable or curable health problems, such as malaria, diarrhea, and pneumonia, which affect under-5 children. 5 Reducing child mortality is recognized as a sustainable development goal of a united nation, and the third global child target for 2030 calls for ending under-5 children deaths and reducing U5M to a minimum of 25 per 1000 live births in each country. 6
Most of the sub-Saharan African countries have practiced methods that cause most rapid decreases in child mortality rate. 7 However, there exist greater disparity, and a large number of child deaths remain among different nations. It remains one of the biggest public health problems in the region.4,7 All top 10 nations that had U5M rates over 90 per 1000 live births are in sub-Saharan Africa. These nations conjointly account for around 60% of the entire under-5 deaths. Most of the causes are infectious diseases and malnutrition that can be treated and/or avoided.4,6
Ethiopia is one of the five countries that partake half of all under-5 deaths in 2018. 6 The 2016 Ethiopian Demographic and Health Survey (EDHS) reported that the country’s U5M rates are 67 children per 1000 live births. 8 Children’s mortality is still high due to prevalent diseases such as fever, diarrhea, cough, malaria, and measles. 9 Nationwide studies have been conducted to estimate the prevalence of associated risk factors of under-5 deaths in Ethiopia.9,10 Different studies and reports suggested that there is a decline in U5M in Ethiopia although there are disparities among regions.6,11,12
In Ethiopia, recent studies 10 have sought to identify the risk factors of U5M using statistical models. However, these studies feature methodological shortcomings. First, the studies used an inappropriate model to the data used. The samples underlying the Demographic and Health Survey (DHS) dataset are complex because stratified multistage cluster sampling was used. It led households in the target population to have unequal probabilities of being selected. 8 Second, ignoring sampling weights leads to erroneous parameter estimates. 13
The objective of this study is to identify correlates and trends of U5M in Ethiopia using 2000–2016 EDHS data by answering the following research questions: 1 What is the trend of U5M from 2000 to 2016 EDHS? 2 What are the correlates that contribute to U5M in Ethiopia? First, the study examines whether there is a significant U5M intra-class correlation (ICC) in the clusters. If the existence of time and regional dependency is observed, the subsequent objective will be to explore important implications to targeting policy for better interventions and to identify variables that might account for the mortality using a multilevel logistic regression model. Furthermore, the study would be the first ever to identify determinants of child mortality in Ethiopia.
The remainder of the article is organized as follows. The data source, sample size and design, some basic statistical analysis, and estimation methods and inferences are introduced in section “Methods.” The results from applying the proposed models to the study data are discussed in section “Results.” Finally, the main discussion and conclusion of the study are given in sections “Discussion” and “Conclusion,” respectively.
Methods
Source of data and study design
The source of data for this study was taken from EDHS conducted by Central Statistics Agency (CSA), which was conducted across the country and available in the Monitoring and Evaluation to Assess and Use Results Demographic and Health Surveys (MEASURE DHS) database at https://dhsprogram.com/data/available-datasets.cfm. EDHS granted permission to access data through the project title “Trend and Correlates of Under-Five mortality.” The DHS is a periodic cross-sectional survey administered at the household level, funded by United States Agency for International Development (USAID) in many middle- and low-income countries. The first Ethiopian DHS (EDHS) was conducted in 2000 and then subsequently in 2005, 2011, and 2016.
Child mortality is one of the sections that have been covered in each subsequent year in the nine regions and two administrative regions both at rural and at urban levels. The EDHS data of 2000, 2005, 2011, and 2016 included a sample of approximately 10,873, 9861, 11,654, and 10,641 under-5 children, respectively, which were used in this study.8,14–16
Inclusion and exclusion criteria
All of the under-5 children whose household response was full were eligible for the study. On the contrary, those whose household response was not full were excluded from the study and counted as missing data in the analysis process.
Data weight
The sampling weights account for the selection probabilities of children at two stratified sampling stages. The design weights are then adjusted for non-response at each level to calculate the final survey weights for children. 17
Bias reduction method
Including survey weights of different levels without scaling produces biased parameter estimates. The survey weight scaling techniques are considered to be a bias minimization technique. 18 The scaling technique which minimizes bias of estimates is given below:
Level 2, household

Level 1, child, scales

where
Variables in the Study
Dependent variable
In this study, the dependent variable is coded as 1 if the child died before reaching 5 years of age and 0 if the child is alive. Therefore, the ith child is represented by a random variable
Independent variables
Factors that are used as prognosticators of U5M included in this study were selected based on the three-level weighted logistic regression model in the univariable analysis at 25% level of significance. These variables are mother’s education level (no education, primary, secondary, or higher), wealth index (poor, middle, rich), sex of household head (male, female), residence (urban, rural), preceding birth interval (<24, 24–47, ⩾47), mother’s age at first birth (<15, 15–25, ⩾25), birth order (⩽3, >3), place of delivery (not health institution, health institution), sex of a child (male, female), plurality (single, multiple), and weight of child at birth (small, average, large). Survey time was used as a moderator variable.
Statistical analysis
Multilevel logistic regression model
Since our dependent variable is dichotomous, logistic regression is the popular model to analyze datasets. 19 This model assumes that all children are independent in the sense that any variable explaining the dependent variable has the same effect in all clusters. Generally, children are nested within households, and households are nested within the cluster and there is a lack of independence across levels of nested data as they are sharing the common characteristics. To overcome these problems, multilevel logistic regression model is an appropriate model. A multilevel logistic regression model can be used to analyze nested sources of variability in hierarchical data, taking account of the variability associated with each level of the hierarchy. 19 There is an individual factor that contributed to U5M as well. The variations among individuals, households, and clusters have different structures. 20
Consider a binary response variable

where
Level 3, cluster, ICC

Level 2, household, ICC

Parametric estimation
Parametric estimation in multilevel logistic regression is not direct like an ordinary regression model. To estimate unknown parameters, standard errors (SE), and confidence interval (CI), the pseudo-maximum likelihood estimation for generalized linear mixed models with two or more levels using adaptive quadrature is implemented in GLLAMM, 22 which is one of the Stata packages. 23
Results
The U5M rate refers to the chance of dying before age 5 years per 1000 live births. Based on the survey of 2000, 2005, 2011, and 2016 EDHS, it was found that the U5M proportion displays a decline in the study periods. The trend in U5M rates in Ethiopia for 2000–2016 EDHS data indicates the average mortality in the preceding 5 years of the survey year. The results of the data depict that U5M is declining over the past decades. The mortality declined from 166 deaths per 1000 live birth in 2000 to 67 deaths per 1000 live births in 2016. This is equivalent to a 60% decline between 2000 and 2016 (Figure 1).

Trend in under-5 mortality rate in Ethiopia, 1997–2013.
Correlates of U5M in Ethiopia
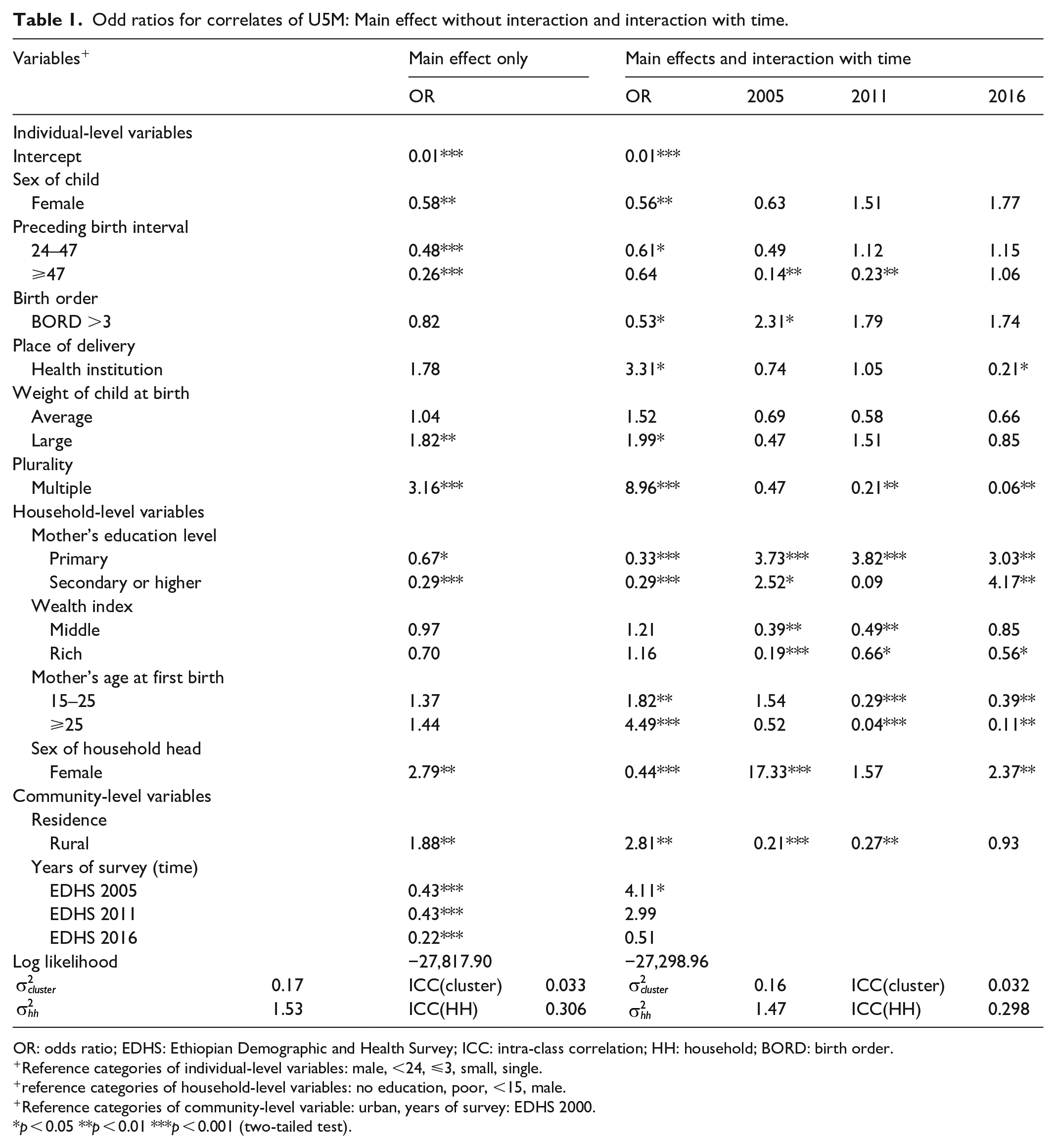
For multivariable three-level logistic regression model, we included sex of a child, preceding birth interval, birth order, place of delivery, weight of child at birth, and plurality as first-level variables; mother’s education level, wealth index, mother’s age at first birth, and sex of household head as second-level variables; and residence and survey time as third-level variables. Sex of child, preceding birth interval, weight of child at birth, plurality, mother’s education level, sex of household head, and residence were found to be significant for the main effect without interaction. Including the significant correlates in the main effect without interaction birth order and mother’s age at first birth were found to be significant for the main effect with interaction (Table 1).
Odd ratios for correlates of U5M: Main effect without interaction and interaction with time.
OR: odds ratio; EDHS: Ethiopian Demographic and Health Survey; ICC: intra-class correlation; HH: household; BORD: birth order.
Reference categories of individual-level variables: male, <24, ⩽3, small, single.
reference categories of household-level variables: no education, poor, <15, male.
Reference categories of community-level variable: urban, years of survey: EDHS 2000.
p < 0.05 **p < 0.01 ***p < 0.001 (two-tailed test).
The odds of U5M of females were 0.56 times (odds ratio (OR) = 0.56, p < 0.01) less than the odds of male children. The odds of U5M for multiple births were 8.96 times (OR = 8.96, p < 0.01) greater than the odds of single births. The odds of U5M for mother’s education level with primary and secondary or higher education were 0.33 and 0.29 times (OR = 0.33, p < 0.01 and OR = 0.29, p < 0.01) less than the odds of mothers with no education level, respectively. The odds of U5M for female household were 0.44 times (OR = 0.44, p < 0.01) less than that for male household head. The odds of U5M among children with rural residence were 2.81 times (OR = 2.81, p < 0.01) greater than among children with urban residence. The rest of the correlates including birth order, place of delivery, wealth index, and mother’s age at first birth did not show any significant association with U5M as we observed from the main effect without interaction (Table 1).
The odds of U5M for children living in rural areas were 2.82 times (OR = 2.82, p < 0.01) greater than among children living in an urban area in 2000 EDHS. The mortality for female children was 44% (OR = 0.56, p = 0.048) times less than for male children in 2000 EDHS. The mortality for multiple births was 8.96 times (OR = 8.96, p < 0.01) greater than for single birth in 2000 EDHS.
The variances of the random effects are 0.16 for the cluster and 1.47 for the household. Estimated ICC for cluster level and household level is 0.032 and 0.298, respectively (Table 1).
The predicted probability of child mortality of those who lived in a poor household is 0.117, 0.096, 0.085, and 0.071 in 2000, 2005, 2011, and 2016 EDHS, respectively. Similarly, the probability of child mortality of those who lived in a middle household is 0.171, 0.110, 0.076, and 0.060 in 2000, 2005, 2011, and 2016 EDHS, respectively. A child who lived in a rural area in 2000, 2005, 2011, and 2016 had a 0.141, 0.094, 0.081, and 0.070 predicted probability of dying. The predicted probability of U5M for mothers with primary education levels in 2000, 2005, 2011, and 2016 is 0.123, 0.07, 0.069, and 0.055, respectively. A child whose preceding birth interval was less than 24 months had a 0.235, 0.174, 0.143, and 0.107 predicted probability of dying in 2000, 2005, 2011, and 2016, respectively. Similarly, a child whose preceding birth interval was 47 months or more had a predicted probability of dying of 0.085, 0.047, 0.047, and 0.041 in 2000, 2005, 2011, and 2016, respectively (Table 2).
Predicted probability of under-5 mortality in Ethiopia from 2000 to 2016 Ethiopian Demographic and Health Survey.

Discussion
U5M is still a major public health problem in sub-Saharan African countries.10,21 Nowadays, improving the health status of children and increasing child health care are low in less-resourced countries including Ethiopia. 24 Therefore, the study aims to identify correlates and trends of U5M in Ethiopia using four-time EDHS data. It is more relevant if the trend of U5M can be studied by considering several surveys over time. This is very important in saving more children’s lives and reducing the gap between developed and limited resource setting countries regarding U5M.
In Ethiopia, there have been substantial improvements in saving children’s lives after the implementation of health interventions since 1960. 25 Our study result also indicates that the mortality rate has declined from 166 deaths per 1000 live birth in 2000 to 67 deaths per 1000 live births in 2016. The result is similar to the study done in Ethiopia. 10 The analysis revealed that a child who is living in rural area faced a higher risk of mortality than a child residing in urban area. This result is supported by the study based on 2011 and 2016 EDHS, in which they showed that the highest percentage of death was recorded in rural areas.26–28
According to the result, multiple births significantly affect under-5 children. Children born with multiple births had a higher risk of dying than those with single births through the study periods. The result was in line with the study done in Ethiopia,28–33 in which the odds of U5M were five times higher among children born with multiple births compared to single birth. Based on the result, sex of a child is also one of the correlates of U5M. The risk of death of a female child is different from that of a male child. Male children had a higher risk of dying than female children. This result is similar to a study done by Fikru et al. 10 and Zewudie et al. 28 However, it contradicted the study conducted in rural settings of Ethiopia. 34
Similarly, the odds of an under-5 child dying before 5 years of age in the case of having a primary and secondary or higher educated mother were reduced compared to a child having no educated mother. The result is supported by Zewudie et al. 28 The finding of the study showed that the odds of dying before 5 years of age were reduced for mothers with age at first birth ⩾25 compared to mothers age at first birth <15 years. Therefore, it is better to have a child at ⩾24 years of age.
In general, the factors related to child mortality vary across time. Understanding both the changing nature of the factors and the changing magnitude of their relationships can help to explain some of the decreases in child mortality rates. The observed significant decrease in U5M is encouraging. This suggests that the country is gradually reaching one of the Sustainable Development Goals (SDG), which is to minimize the child mortality rate below 25 per 1000 live births by 2030. 35
Strengths and weakness of the article
The strength of this study was the incorporation of four times repeated cross-sectional surveys conducted at the national level to see the trend and determinant factors of U5M. This could increase the generalization of the study findings to the whole region of Ethiopia. Almost all of the studies conducted on U5M in Ethiopia did not include the effect of clusters, which accounts for the heterogeneity;10,36,37 rather, they relied on regions, 20 which is not large enough to account for disparities. 38 This study is not free from limitations since some important variables were not included and was only limited to the variables mentioned in the methodological part. Furthermore, some variables with a large number of missing observations were omitted. In addition, the cross-sectional survey is not free from bias as it was collected once per 5 years. Furthermore, power analysis for sample size calculation was not done. These in turn might affect our conclusions.
Conclusion
Child mortality varied across time in Ethiopia. Understanding both the time-varying nature of the correlates and changes in the type of their associations can help to explain some of the decreases in child mortality rates. Sex of child and weight of the child at birth showed significant association with child mortality without interaction effect. On the other hand, birth order, place of delivery, plurality, wealth index, and mother’s age at first birth are significant correlates associated with U5M. Direction and/or presence of a relationship between these correlates and child mortality significantly interacted with time. Therefore, to mitigate the burden of U5M, the concerned body should provide awareness to the community.
Footnotes
Acknowledgements
The authors would like to acknowledge the Central Statistics Agency of Ethiopia and the DHS office as they approved access to the data after we prepared the proposal on the title.
Author contribution
KSW: contributed to study concept, design, and statistical analysis and drafted the manuscript. RHB: participated in data clearance, drafted the manuscript, and performed the statistical analysis. Both authors approved the final manuscript.
Availability of data and materials
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The EDHS are secondary data, which are publicly available; approval was sought from MEASURE DHS/ICF International, and permission was granted for this use. The original DHS data were collected in conformity with international and national ethical guidelines. Ethical clearance was provided by the Ethiopian Public Health Institute (EPHI) (formerly the Ethiopian Health and Nutrition Research Institute (EHNRI)) Review Board, the National Research Ethics Review Committee (NRERC) at the Ministry of Science and Technology, the Institutional Review Board of ICF International, and the US Centers for Disease Control and Prevention (CDC). Written consent was obtained from mothers/caregivers and data were recorded anonymously at the time of data collection during EDHS 2000, 2005, 2011, and 2016. Supplementary information about DHS data usage and ethical standards are available at ![]() .
.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.