
Abstract
Objective:
Vaginal birth after cesarean could be considered a reasonable and safe option for most women with a previous cesarean section. However, it is not easy to select pregnant mothers who are a candidate for a trial of labor after cesarean. Therefore, this study is aimed to identify determinants of successful vaginal birth after previous cesarean delivery in public hospitals in East Wollega, Western Ethiopia, 2020.
Methods:
A facility-based unmatched case–control study was conducted on 115 cases and 115 controls. Cases were those women who successfully delivered vaginally and controls were those women delivered by cesarean section after trial of labor. Data were collected using a pre-tested structured questionnaire and organized using Epidata version 3.1. Descriptive analysis and logistic regressions were performed. The adjusted odds ratio with a 95% confidence interval was used and statistical significance was declared at P-value < 0.05.
Results:
The study revealed that rural residence (adjusted odds ratio = 3, 95% confidence interval = 1.25–7.21), having no history of stillbirth (adjusted odds ratio = 4.2, 95% confidence interval = 1.20–14.62), prior vaginal birth after cesarean (adjusted odds ratio = 2.4, 95% confidence interval = 1.2–6.4), counseling about a trial of labor after cesarean during antenatal follow-up (adjusted odds ratio = 4.7, 95% confidence interval = 1.88–11.74), and birth interval of >2 years (adjusted odds ratio = 8.9, 95% confidence interval = 3.25–24.67) were found to be determinants of successful vaginal birth after cesarean.
Conclusion:
Place of residence, history of stillbirth, history of vaginal birth after cesarean, counseling about mode of delivery during antenatal care, and birth interval were determinants of successful trial of labor after cesarean. Given these factors, it is recommended that care providers should advocate delaying pregnancy for at least 2 years and counseling women about trial of labor after cesarean during antenatal care follow-up.
Introduction
A trial of labor after a cesarean (TOLAC) delivery refers to a planned attempt to deliver vaginally by a woman who had a repeat cesarean delivery regardless of its outcome. If it is successful, it will result in vaginal birth after cesarean (VBAC), and if it fails, it will end in another cesarean delivery.1–3 According to different works of literature, there is a consensus that planned VBAC is a clinically safe choice for the majority of women with a single previous lower segment cesarean delivery for non-recurring indications.
Compared to repeated cesarean delivery, VBAC is associated with no surgical complication, shorter hospital duration, less risk of postpartum hemorrhage, decreased maternal morbidity, and decreased risk of complication in future pregnancies. In addition to this, VBAC is also a key strategy to decrease unnecessary repeated cesarean births and is also more cost-effective under a wide variety of circumstances.4–6
The dictum that goes once a cesarean always cesarean changes to the TOLAC in the 1970s, the rates of VBAC were reported to be 5% and 28.3% by the year 1985 and 1996, respectively, resulting in a 2.8% decrease of cesarean delivery rates. But since there was no adequate information regarding factors associated with the success of TOLAC and criteria for candidates of TOLAC, the number of reports of uterine rupture and other complications related to TOLAC was increased and the overall rate of VBAC decreases to 8.6% by the year 2016; in addition to this, some hospitals stopped offering TOLAC due to fear of complications.2,6
Compared to women who undergo repeated cesarean delivery, women who undergo TOLAC and had successful vaginal birth generally had lower rates for most of the morbidities. 7 On the contrary, failed trials of labor were generally associated with higher morbidities than scheduled repeated cesarean deliveries, especially for ruptured uterus.1,2,7
In Ethiopia, magnitude of successful TOLAC was not clearly known. There are only a few studies on TOLAC. 7 A study in Addis Ababa showed 69.4% of mothers had successful VBAC. 8 Therefore, identifying determinants of VBAC delivery, especially in a resource-limited setting, reduces cesarean delivery rates, and thus decreases maternal morbidities from cesarean deliveries. It also saves financial resources in the health sector.
Methods and materials
Study period and area
The study was conducted from 29 February to 30 June in all public hospitals in East Wollega, Western Ethiopia. There are five public hospitals in the zone. Of these, one is a comprehensive specialized hospital (Nekemte Specialized Hospital), one is a teaching referral hospital (Wollega University Referral Hospital), and the other three are general public hospital (Gida General Hospital, Sire Hospital, and Arjo Hospital). Obstetrics services of these hospitals are led by 10 obstetricians, 9 integrated emergency obstetrics and surgery professionals, and more than 80 professional midwives.
Study design
A facility-based, unmatched case–control study was employed for this study. To include as many variables as possible, matching was not carried out.
Study population
All laboring women who had one lower uterine segment cesarean scar (LUSCS) and agreed to TOLAC from 29 February to 30 June 2020, were the study population.
Cases were all women who had a successful vaginal birth after undergoing a trial of labor and controls were women who failed trial of labor. Women with previous two cesarean scars were excluded.
Sample size determination and sampling technique
The sample size of this study was calculated using Epi-info version 7.0.8 based on the following assumptions; the case to control the ratio of 1:1, 95% confidence level (CI), power at 80%, and proportion of exposure of controls (prior successful VBAC) to be 6.79% with adjusted odds ratio (AOR) of 3.39. 7 By adding a 10% non-response rate, the final sample size was 236 with 118 cases and 118 controls.
Data collection procedures
Data on sociodemographic variables, obstetrics factors, medical factors, and fetal factors were collected using a structured interviewer-administered questionnaire which was developed by reviewing different works of literature across the world.2,4,7–18 Cases were identified by trained general practitioners. These cases were reviewed and approved for inclusion by the attending obstetrician. Eight midwifery professionals were recruited and trained to collect data. All questionnaires were checked for completeness by the principal investigator.
Statistical analysis
The data were coded and entered into EPI data version 3.1 and transferred to SPSS version 25 software for analysis. Categorical variables have been expressed as frequencies and percentages. The odds ratio (OR) along with their 95% CIs were calculated. All variables that had a P-value of <0.2 in the bivariate analysis were included in the multivariate logistic regression analysis model to determine the factors associated with successful VBAC. Statistical significance was set at a P-value of <0.05.
Results
Sociodemographic characteristics of the study participants
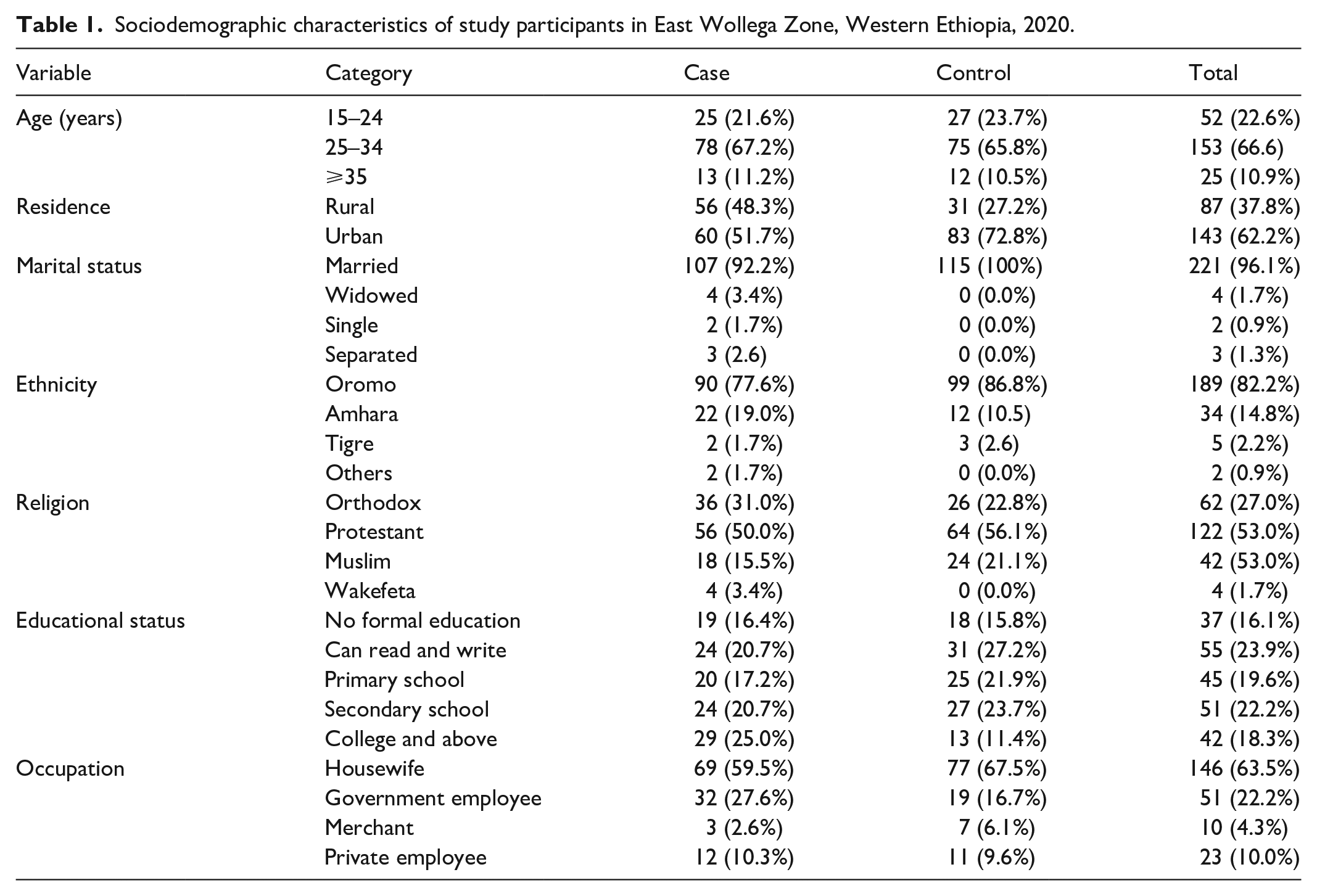
A total of 230 participants (115 cases and 115 controls) with a response rate of 97.4% have been considered in the final analysis. The mean age of cases was 27.8 with standard deviation (SD) ±4.33 and the mean age of controls was 27.4 with SD ±4.48. Sixty (51.7%) cases and 31 (27.2%) controls were from rural. Nineteen (16.4%) cases and 18 (15.8%) controls had no formal education (Table 1).
Sociodemographic characteristics of study participants in East Wollega Zone, Western Ethiopia, 2020.
Obstetrics characteristics of study participants
The majority of controls, 83 (72.2%), and half of, 57 (49.6%), cases were para 2 and para 3–4, respectively. The mean gestational age of the cases is 38.28 ± 2.016 and it is 39.04 ± 1.867 for the controls. One-hundred six (92.2%) cases and 55 (47.8%) controls had a birth interval of more than 2 years. Regarding antenatal care (ANC) follow-up, 97% of cases and 96.5% of controls had ANC follow-up. Of total participants with antenatal follow-up, 95% of cases and 49% of controls have been counseled about TOLAC. The number of women admitted to being in the active phase of labor was similar for cases and controls. Results regarding the duration of labor show that majority of the women in the case group had a duration of labor of ⩽8 h while the majority of controls had a duration of labor of ⩾9 h. Ten (8.6%) of cases and 25 (21.9%) of controls have a history of stillbirth (Table 2). The most common indication of previous cesarean delivery among cases was malpresentation, 26 (22.4%).
Current obstetric characteristics of study participants, East Wollega, Western Ethiopia, 2020.

GA: gestational age; ANC: antenatal care; VBAC: vaginal birth after cesarean delivery; CS: cesarean; TOLAC: trial of labor after a cesarean.
However, the most common indication in controls was a failure of labor progress, 34 (29.8%) (Figure 1).

Indication of previous cesarean section from study participants, East Wollega, 2020.
Determinants of successful vaginal birth after previous cesarean delivery
In this study, multivariate logistic regression analysis showed the place of residency, having no history of stillbirth, prior VBAC, a birth interval of more than 2 years, and counseling about TOLAC during ANC follow-up was found to be significant determinants of VBAC.
The odds of rural residence is three times higher in cases than in controls (AOR = 3, 95% CI = 1.25–7.21). The odds of having no history of stillbirth are four times higher in cases than in controls (AOR = 4.19, 95% CI = 1.20–14.62). The odds of prior VBAC is twice higher in cases than controls (AOR = 2.4, 95% CI = 1.2–6.4). The odds of receiving counseling regarding TOLAC is about 4.7 times higher in cases than in controls (AOR = 4.71, 95% CI = 1.88–11.74) and the odds of a birth interval of greater than 2 years is almost 9 times higher in cases than in controls (AOR = 8.96, 95% CI = 3.25–24.67) (Table 3).
Determinants of successful vaginal birth after previous cesarean delivery among study participants in East Wollega, Western Ethiopia, 2020.

COR: crude odds ratio; AOR: adjusted odds ratio; SVD: spontaneous vaginal delivery; VBAC: vaginal birth after cesarean delivery; TOLAC: trial of labor after cesarean delivery.
P < 0.05; **P < 0.01; ***P < 0.001.
Discussion
The findings of the study revealed that rural residence, having no history of stillbirth, counseling regarding TOLAC during ANC follow-up, and birth interval of greater than 2 years are significant determinants of VBAC.
Women with low socioeconomic status are less likely to decline the trial of labor after cesarean. 9 In this study, women who live in rural areas were three folds more likely to have successful VBAC than those who live in urban areas. This might be explained by the fact that rural residents prefer vaginal birth because of their lifestyles and fear of surgery. This finding is similar to a study conducted in Southeastern Anatolia, Turkey. 4
Having no history of stillbirth is also a significant determinant factor of successful VBAC. Results from the study conducted in Addis Ababa are also in line with this finding. 7 This implies that having a bad obstetric history like stillbirth can determine the mode of delivery. Mothers with previous cesarean delivery assume that the cesarean route of delivery would give the mother a higher chance of having an alive baby. 7
In this study, prior successful VBAC was found to be associated with current successful VBAC which is similar to other studies.2–4,7 Many authors reported a history of prior spontaneous vaginal delivery as an important determinant for successful VBAC.4,5,7 This study failed to show that.
In this study, counseling regarding TOLAC during ANC follow-up is also a significant determinant of successful VBAC. This finding is consistent with the study conducted in Sudan, Khartoum maternity hospital.1,3,5,10 This might be because women who had been counseled regarding TOLAC during ANC follow-up have better knowledge on the benefits and risks of VBAC and better psychological readiness for vaginal birth which might be very helpful in achieving successful VBAC delivery when compared to women who had not been counseled.5,11 A final decision for the mode of delivery should be agreed upon by the woman and member(s) of the treating team before the expected date of delivery.5,12
The birth interval of greater than 2 years is also one of the significant determinants of successful VBAC. This is supported by similar studies.13–15 Therefore, delaying pregnancy more than 2 years in mothers with previous cesarean section is recommended. Practitioners should also consider this when counseling pregnant mothers for VBAC. 16 However, a study conducted in Ethiopia did not show this association. 7
In this study, maternal age is not found to be a significant determinant of successful VBAC. This is supported by other studies.7,17,18 However, one study showed a significant association between age and the success of VBAC. 19 This contradiction is most probably because, unlike women in developing countries, women in developed countries report their exact age, and the association is clearly shown.
In this study, unlike other studies,4,7 stage of labor or cervical dilatation does not affect VBAC. Because the proportion of participants in latent and active phases were similar.
Results of this study have indicated that the majority of participants who have received general anesthesia during the previous cesarean delivery have failed TOLAC while the majority of the participants who had received local anesthesia had successful VBAC. However, the use of local anesthesia during previous cesarean delivery is not found to be significantly associated with successful VBAC.
Limitations of this study
This study was a cross-sectional study and may not show the cause and effect relationship. The other limitation could be a small sample that might lead to statistical imprecision. Therefore, further studies with a larger sample size are advisable.
Conclusion
Place of residence, history of stillbirth, history of VBAC, counseling about mode of delivery during ANC, and birth interval were determinants of successful TOLAC. Given these factors, it is recommended that care providers should advocate delaying pregnancy for at least 2 years and counseling women about TOLAC during ANC follow-up.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221097597 – Supplemental material for Determinants of successful trial of labor after a previous cesarean delivery in East Wollega, Western Ethiopia: A case–control study
Supplemental material, sj-docx-1-smo-10.1177_20503121221097597 for Determinants of successful trial of labor after a previous cesarean delivery in East Wollega, Western Ethiopia: A case–control study by Lemane Dereje, Temesgen Tilahun and Jote Markos in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Wollega University for all-around support. The authors acknowledge East Wollega Zonal Health Department heads and hospital managers for their participation and facilitating the process of data collection. The authors’ appreciation also goes to the supervisors, data collectors, and all of the study participants.
Author contributions
L.D. conceived the study, participated in the design of the questionnaire, in drafting and finalizing the manuscript, and assisted with the design of the study and data analysis. All authors read and finally approved this manuscript for submission. T.T. conceived the study, its overall design, and execution, designed the questionnaire, performed data collection, performed the statistical analysis, and served as the lead author of the manuscript. J.M. conceived the study, participated in the design of the questionnaire, performed the statistical analysis, drafted the manuscript, and assisted in the design of the study and data analysis.
Availability of data and materials
The data sets are available from the corresponding author on a reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical clearance was obtained from the Research Ethics Review Committee of Wollega University (approval no./ID = WU/RD/370/2012).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study has been funded by Wollega University who did not influence study design, data collection, analysis, and interpretation of data, and in writing the manuscript.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.