
Abstract
Objectives:
The current study aimed to determine the magnitude of home delivery and its associated factors in East Africa using data from the Demographic and Health Survey.
Methods:
We pooled data from the Demographic and Health Survey of the 11 East African countries and included a total weighted sample of 126,107 women in the study. The generalized linear mixed model was fitted to identify factors associated with home delivery. Variables with adjusted odds ratio with a 95% confidence interval, and p value < 0.05 in the final generalized linear mixed model were reported to declare significantly associated factors with home delivery.
Result:
The weighted prevalence of home delivery was 23.68% (95% confidence interval: [23.45, 23.92]) among women in East African countries. Home delivery was highest in Ethiopia (72.5%) whereas, it was lowest in Mozambique (2.8%). In generalized linear mixed model, respondent’s age group, marital status, educational status, place of residence, living country, wealth index, media exposure, and number of children ever born were shown significant association with the home delivery in the East African countries,
Conclusion:
Home delivery varied between countries in the East African zone. Home delivery was significantly increased among women aged 20–34 years, higher number of ever born children, rural residence, never married, or formerly married participants. On the contrary, home delivery decreased with higher educational level, media exposure, and higher wealth index. Wide-range interventions to reduce home delivery should focus on addressing inequities associated with maternal education, family wealth, increased access to the media, and narrowing the gap between rural and urban areas, poor and rich families, and married and unmarried mothers.
Introduction
Maternal mortality remains a major public health problem worldwide. The sub-Saharan African regions bear the highest burden, with 85% of maternal deaths reported from the region. Studies indicate that every year, 529,000 maternal deaths and 4 million newborn deaths in the first week of life occur around the world.1,2 The estimated maternal mortality ratio (MMR) in developing countries (239 per 100,000 live births) is 20 times higher compared to the developed regions (12 maternal deaths per 100,000 live births). Despite great improvement in recent decades, the drop in maternal mortality is far from reaching a target decline of reaching less than 70 MMR by 2030 at the current pace.3,4
Most maternal deaths in sub-Saharan Africa are highly attributed to home delivery, with most births occurring at home. In low- and middle-income countries (LMICs), many deliveries still occur at home without the assistance of trained attendants.2,5 Mothers deliver in an unhygienic environment, without a skilled birth attendant and lifesaving medications. Sub-Saharan Africa and South Asia together contribute over 85% of maternal deaths, and of which only half of deliveries are at home.6,7 The negative impact of home delivery extends to the child and is responsible for neonatal morbidity and mortality. Since home deliveries are attended by unskilled health care professionals and occur in an unsafe environment, they lead to adverse neonatal and maternal outcomes such as an increased risk of infection, postpartum hemorrhage (PPH), and HIV/AIDS transmission to relatives or traditional birth attendants, who deliver without protective equipment. Most of these maternal deaths are preventable if appropriate and timely interventions are applied.8,9
Evidence showed that although skilled birth attendants can save the lives of women, only 59% of births were attended by skilled birth attendants between 2012 and 2017 in sub-Saharan Africa. The high load of home deliveries in the region is a precipitating factor for the high maternal mortality rate. The large proportion of direct cause of maternal death including obstetric complications such as hemorrhage, pregnancy-induced hypertension, sepsis, and obstructed labor which collectively accounts for 64% of maternal deaths could be prevented primarily by making the delivery attended by a skilled birth attendant at a health facility.10,11
Despite the high proportion of MMR in East African countries primarily attributed to home delivery, overall magnitude of home delivery and its determinants remains unclear. In addition, the pooled analysis among East African countries using Demographic and Health Survey (DHS) data which are nationally representative is crucial for understanding common determinants across countries, and this in turn helps to reduce prevalence of home delivery. Therefore, the current study aimed to determine the magnitude of home delivery and its determinant factors in East Africa using data from the DHS.
The finding of the current study provides evidence for health planners, decision makers, stakeholders, and health professionals in planning for further reduction of home delivery which is helpful in turn to decrease maternal mortality in LMICs. Moreover, being a pooled analysis, power of the study increases and helps to reduce the measurement errors and bias resulting from heterogeneity in designs and data collection methods.
Methods
Study setting, design, and period
We conducted a cross-sectional pooled analysis based on DHS conducted in the 11 East African countries (including Burundi, Comoros, Ethiopia, Kenya, Malawi, Mozambique, Rwanda, Tanzania, Uganda, Zambia, and Zimbabwe) from 2012 to 2017. The DHS is considered as the main data source as it was designed to provide population and health indicators at the national and regional levels. The data collection period was varying but includes the data of 5 years prior to the survey. This further data analysis was carried out between January and February 2021.
Based on updated country income classifications for the World Bank 2020 fiscal year, Burundi, Ethiopia, Malawi, Mozambique, Rwanda, Tanzania, and Uganda are low-income countries, while Comoros, Kenya, Zambia, and Zimbabwe are LMICs. 12
Data source and sampling
Data were obtained from the DHS measure program on the website www.measuredhs.com after we submitted concept notes about the project. We pooled the most recent DHS data from the 11 countries of East African countries. There are 20 countries in the Regions of East Africa according to World Health Organization (WHO) classification. In history, only 13 of these countries had DHS data. For this study, 11 countries were included 13 (Figure 1).

Schematic presentation of the countries sampled from East Africa for the pooled analysis of home delivery.
The DHS used two stages of stratified sampling technique to select the study participants. In the first stage, the Enumeration Areas (EAs) were randomly selected. In the second stage, households were selected. We pooled data from DHS from the 11 East African countries and included a total weighted sample of 126,107 women who had a history of delivering children in the last 5 years prior to the survey day in the study.
Data collection methods
The DHS program adopts standardized methods that involve uniform questionnaires, manuals, and field procedures to gather information that is comparable between countries around the world. It is the representative household surveys that capture data from a wide range of monitoring and impact evaluation indicators in the area of population, health, and nutrition with face-to-face interviews of women aged 15–49 years. Each country’s survey consists of different data sets, including men, women, children, birth, and household data sets. Detailed survey methodology and sampling methods used in gathering the data have been reported elsewhere. 14 For this study, we used the Individual Record Data Set (KR file) which contained information on eligible women aged 15–49 years in each country.
Variables and measurement
Outcome variable
The outcome variable of this study was a home delivery. The response variable was generated from the question asked to women who gave birth within 5 years preceding the survey question. The response was dichotomized as a home delivery and institutional delivery (if delivered at any type of health institutions). Home delivery includes the option given in the survey question termed home of respondents and home and others’ home. Health institutions include government hospitals, health centers, health posts, private clinics, or private hospitals. If women deliver at home, we coded “1,” otherwise coded “0.”
Independent variables
Country, age, marital status, educational level, place of residence, wealth index, sex of head of household, age of head of household, media exposure, and total children ever born were included as independent variables in this study
Statistical analysis
The variables were extracted using the KR file. We use STATA software version 16.0 to clean, recode, and analyze the pooled data. After joining the extracted data from the 11 East African countries, we weighted the data using the individual sample weight of the women (v005) and strata (v021). The proportion of home delivery was described and presented using a pie chart. The DHS data had a hierarchical structure as women were nested within a cluster, and clusters within the country. Hence, the data violate the independence of the observation, as the women may share similar characteristics within the cluster (and/or country). This implies that there is a need to consider the variability between clusters by using generalized linear mixed models (GLMMs). The odds ratio test, the intra-cluster correlation coefficient (ICC), the median odds ratio (MOR), and the proportional change in variance (PCV) were calculated to measure the variation between clusters. The ICC quantifies the proportion of the total observed difference in home delivery attributable to cluster variations (degree of heterogeneity). On the contrary, MOR was used to quantify the variation or heterogeneity in home delivery between clusters. Therefore, MOR is defined as the median value of the odds ratio between the high odds of the cluster and the lower odds of the cluster when selecting two clusters/EAs randomly. Finally, PCV measures the total variation in home delivery attributed to factors at the individual and community levels in the final model compared to the null model. The detail description and formulas for ICC, 15 MOR, 16 and PCV 16 are described elsewhere. The null model, individual level, cluster level, and factors of both cluster and individual level were fitted. Model comparison was made based on the deviation likelihood ratio (2LLR) since the models were nested. Finally, a GLMM (family (binomial) link (logit)) with factors both at individual and cluster level was selected.
Variables with a p value < 0.2 in the bivariable analysis for individual and community factors were fitted into the multivariable model. Variables with adjusted odds ratio (AOR) with 95% confidence interval (CI), and p value < 0.05 in the final GLMM were reported to declare significantly associated factors with home delivery.
Results
Sociodemographic characteristics
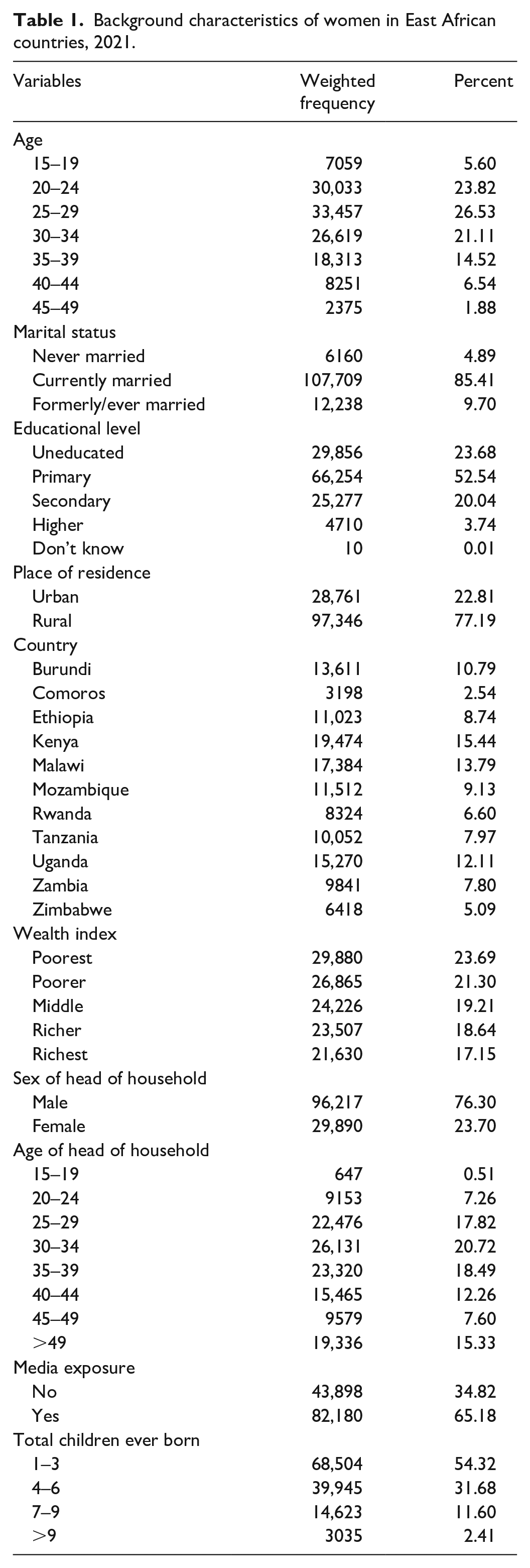
In this study, a total of 126,107 weighted data of women who delivered in the 5 years preceding each country’s DHS were included. The highest proportion of data came from Kenya (15.44%), Malawi (13.79%), and Uganda (12.11%), while Comoros (2.54%) and Zimbabwe (5.09%) were the countries with the smallest number of women included in the study. Highest percentage (26.53%) of women were in age group 25–29 years followed (23.82%) by 20–24 years. Currently married women accounted for the large majority (85.41%) of the study participants. More than half (52.54%) of the women attended primary education. More than three-fourth (77.19%) of the study participants were living in rural areas. Males were the head of household in three out of four (76.30%) of the study participants. Near to two-thirds (65.18%) of the participants reported exposure to media. The sociodemographic characteristics of the participants are summarized in Table 1.
Background characteristics of women in East African countries, 2021.
Prevalence of home delivery
The weighted prevalence of home delivery was 23.68% (95% CI: [23.45, 23.92]) among women in East African countries (Figure 2). Home delivery was highest among Ethiopian women (72.5%), followed by Kenyan women (37.5%) and Tanzanian women (34.7%). On the contrary, it was lowest among women from Mozambique (2.8%), Rwanda (6.9%), and Malawi (7.1%).

The prevalence of home delivery among women in East African countries, 2021.
Home delivery was higher among women 45–49 years (33.8%) followed by 40–44 years (32.4%) and 35–39 years (26.6%). In the same way, home delivery was higher among currently married women (24.4%), uneducated women (39.8%), women from rural area (27.9%), and women with lower economic status (36.2%). The proportion of home delivery was higher among women living in household headed by male (24.5%), women who have no media exposure (32.2%), and women who ever born greater than nine children (42.9%). The prevalence of home delivery ranged from 13.8% among women from households headed by people aged 15–19 years to 27.3% among the head with age group 40–44 years (Table 2).
Distribution of home delivery among women in East African countries, 2021.

Factors associated with home delivery
From fitted four models (null model, individual level, cluster level, and both cluster- and individual-level factors), the model with both cluster- and individual-level factors was found to be optimal model (variance = 1.34, p < 0.001). Accordingly, respondent’s age group, marital status, educational status, place of residence, living country, wealth index, media exposure, and total children ever born were shown significantly associated with the home delivery in the East African countries.
In this final best-fit model, approximately 29% of the variability between communities in the odds of home delivery was due to community-level factors (ICC = 28.87%) and approximately 73% of the variance in the odds of home delivery (PCV = 72.71%) between clusters was attributed to both individual and community-level factors. The MOR (3.82; 95% credential interval: [3.67, 3.98]) showed that the unexplained heterogeneity between clusters (EA) was of greater relevance than the individual variables considered in the analysis to understand the pattern of home delivery.
The odds of home delivery were 14% times lower among both mothers younger than 20 years (AOR = 0.86, 95% CI: [0.79, 0.94]) and mothers older than 34 years (AOR = 0.84, 95% CI: [0.79, 0.89]) compared to women in the age group 20–34 years. Never married and formerly married women were 21% (AOR = 1.21, 95% CI: [1.09, 1.34]) and 30% (AOR = 1.30, 95% CI: [1.22, 1.49]) more likely to delivery at home as compared to currently married women. Women at primary education level, secondary level, and higher (tertiary) level were 30% (AOR = 0.70, 95% CI: [0.67, 0.74]), 60% (AOR = 0.40, 95% CI: [0.37, 0.43]), and 86% (AOR = 0.14, 95% CI: [0.11, 0.17]) less likely to deliver at home compared to uneducated women. The odds of home delivery was 2.27 (AOR = 2.28, 95% CI: [2.07, 2.49]) times higher among women living in rural areas in compared with urban women.
The odds of home delivery were 2.24 times (AOR = 2.24, 95% CI: [1.99, 2.61]) higher among Ethiopian women than among Kenyan women. However, the odds of home delivery were reduced by 98% (AOR = 0.02, 95% CI: [0.02, 0.03]) among women from Mozambique, 96% (AOR = 0.02, 95% CI: [0.02, 0.03]) among Malawian women, 94% (AOR = 0.06, 95% CI: [0.05, 0.07]) Rwandan women, 95% (AOR = 0.05, 95% CI: [0.04, 0.06]) Burundian women, 85% (AOR = 0.15, 95% CI: [0.13, 0.18]) Zambian women, 75% (AOR = 0.25, 95 CI: [0.20, 0.30]) women from Comoros, 69% (AOR = 0.32, 95% CI: [0.27, 0.38]) Zimbabwean women, 66% (AOR = 0.33, 95% CI: [0.29, 0.37]) Ugandan women, and 53% (AOR = 0.47, 95% CI: [0.41, 0.54]) Tanzanian women compared to Kenyan women.
Compared with women with poorest wealth status, the odds of home delivery was decreased by 26% (AOR = 0.74, 95% CI: [0.70, 0.78]), 40% (AOR = 0.60, 95% CI: [0.57, 0.64]), 55% (AOR = 0.45, 95% CI: [0.42, 0.49]), and 74% (AOR = 0.26, 95% CI: [0.24, 0.29]) among women with poorer, middle, richer, and richest wealth status, respectively. Women who had been exposed to the media had 19% (AOR = 0.81, 95% CI: [0.78, 0.85]) lower chances of home delivery compared to women without exposure to the media. The odds of home delivery was increased by 17% (AOR = 1.17, 95% CI: [1.15, 1.18]) as a total number of children was increased by one child. The odds of home delivery were reduced by 9% (AOR = 0.91, 95% CI: [0.87, 0.95]) among mothers in the women’s household head compared to mothers whose husband is household head (Table 3).
Bivariable and multivariable mixed-effect GLMM analysis of home delivery among women in East African countries, 2021.
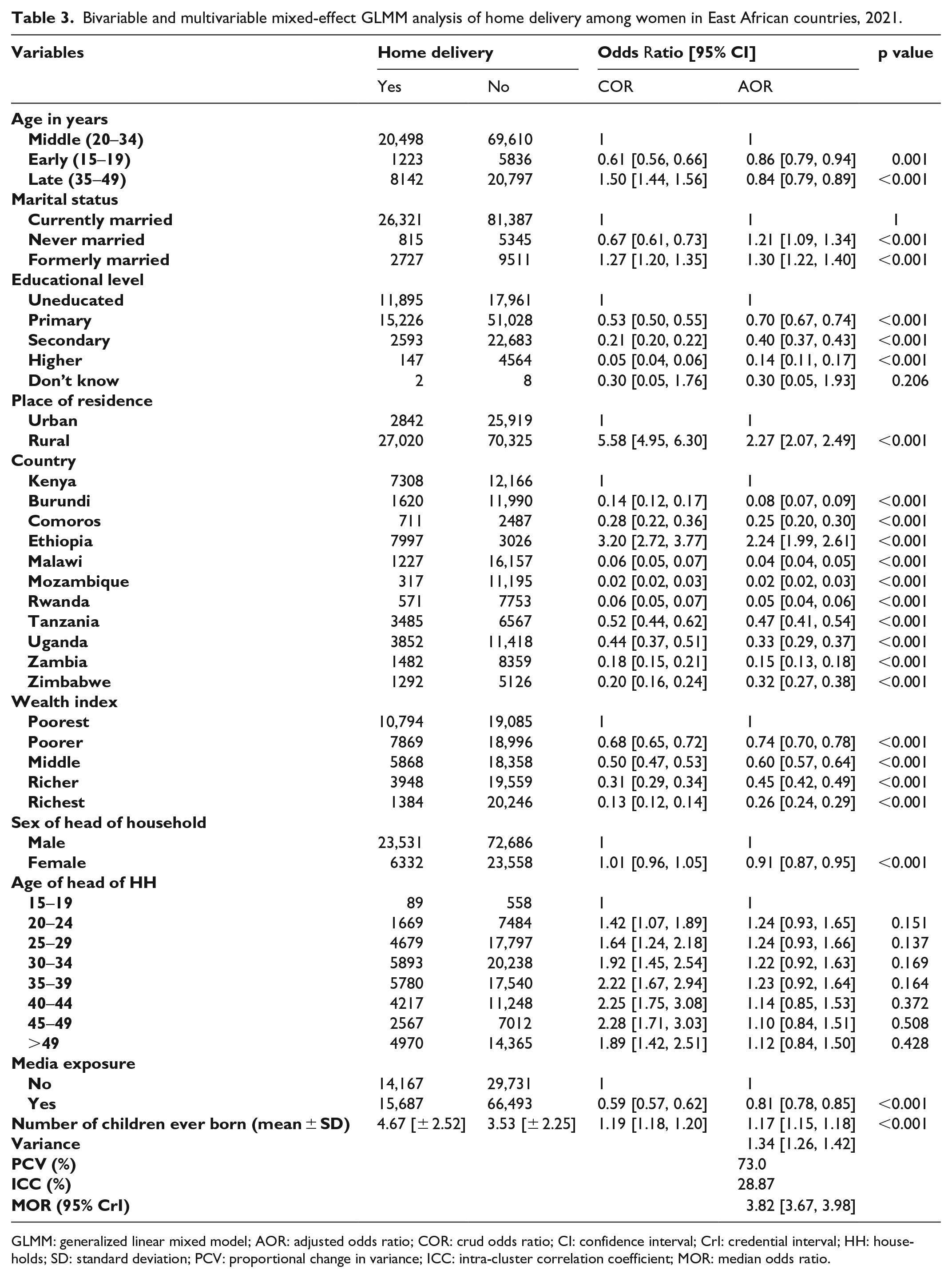
GLMM: generalized linear mixed model; AOR: adjusted odds ratio; COR: crud odds ratio; CI: confidence interval; CrI: credential interval; HH: households; SD: standard deviation; PCV: proportional change in variance; ICC: intra-cluster correlation coefficient; MOR: median odds ratio.
Discussion
This study included a total of 126,107 women who gave birth in the 5 years preceding each recent survey conducted in East African countries. The prevalence of home delivery was wide-ranging between countries in Eastern Africa (ranging from 2.8% in Mozambique to 72.5% in Ethiopia). The expected reason for this great difference between the proportion of home delivery among these two countries (Ethiopia and Mozambique) is the existence of health extension worker in Ethiopia which can facilitate delivery at home.
The prevalence of home delivery was associated with the age group of the respondent, marital status, educational status, place of residence, country of residence, wealth index, media exposure, and number of children ever born. The pooled prevalence of home delivery from the East African region is consistent with the Indian DHS report (22%) 17 and lower than the studies conducted in Nigeria. 18 Compared to Kenyans, the probability of home delivery was 2.24 times higher among Ethiopians. However, the probability of home delivery decreased by 98% for Mozambique, 96% for Malawian, 95% for Rwandan, 92% for Burundian, 85% for Zambian, 75% for Comoros, 68% for Zimbabwean, and 66% for Ugandan. The geographical locations of studies varied widely with populations with differing background characteristics and social customs. In addition to social determinants, the health service coverage, quality of maternal health care services, economical, and health policy of the country might have a role in reducing the home delivery. 19
The probability of home delivery was reduced by about 15% among women aged 15–19 years and 35–49 years compared to women in the middle age group (20–35 years). This association is similar to the result of a previous study. 2 Currently, unmarried women (never married or formerly married) were more likely to deliver at home compared to currently married women. Theories linking marital status, pregnancy, and birth preparedness indicated that unmarried women faced a lack or reduced level of psychosocial support and relationship stability. 20 Pregnant women without marriage might be unplanned and/or unwanted. On the contrary, there is low social acceptance of unmarried status because there is still social stigmatism surrounding illegitimate births in many countries. Therefore, unmarried women can be intrinsically different from married women who can be less empowered, self-isolated, or lack motivation to access the health service.21–23 All these factors might be increasing the odds of home delivery among currently unmarried mothers.
Educated women had less probability of having children at home compared to uneducated women. The result was in line with individual studies conducted in rural Ethiopia,24–26 Zimbabwe, 27 Nigeria, 28 Ghana,29,30 Guinea, 21 and Nepal. 31 The reason for this might be due to the fact that when mothers are educated, it is more likely to enhance female self-determination, positive attitudes, and financial freedom.32,33 Furthermore, it is more likely that educated women demand higher quality services and be alert of difficulties during pregnancy as well as childbirth. As a result, they are more probable to use maternal health care services unlike the illiterate ones. 34 These could collectively influence mothers’ awareness to seek better maternal health services, including delivery in health facilities.
Women in rural areas had higher odds of home delivery, which is similar to findings in previous studies.21,26,29,35 Rural residents in sub-Saharan African countries have poor access to health care facilities. Moreover, lack of privacy and confidentiality, and negligence in the provision of care during childbirth by skilled birth attendants are the fears of the women. 36 With rural health care provider shortages, greater travel distances, and very limited access to obstetric care, it could be likely that there would be a high risk of home delivery in rural areas.
Compared with women with poorest wealth status, the odds of home delivery were decreased by 26%, 40%, 55%, and 74% among women with poorer, middle, richer, and richest wealth status, respectively. This result was in agreement with previous studies. 24 –26,29 The financial capacity of the family and the costs related to transportation may determine the place of delivery. Moreover, women from higher wealth status might be more empowered, participate in decision, and seek maternal health service.
Consistent with previous studies,21,26,37,38 our finding suggests that women exposed to media had about 20% lower odds of home delivery compared to women without exposure to the media. The promotion of institutional delivery by media and the danger of home delivery can influence mothers to develop positive behavior toward delivery in a health facility.
The other most significant determinant of home delivery in this study was the number of children. The probability of home delivery increased by 17% as the number of total children in the household increases by one child. This finding was consistent with previous studies conducted in Ethiopia.21,26 Since women normalize childbirth, they might be less likely to seek care during labor. 39 The literature also indicated that previous interactions between women and health facilities have an influence, and poor experiences during previous deliveries can discourage women from returning for the next birth.40,41 Therefore, the less fear of complications, the adverse experience of care for women during childbirth could discourage them from using health facility services in subsequent pregnancies. In addition to these, multiparous mothers who had done their previous deliveries at home might be more likely to deliver at home in their recent pregnancy.42,43
This further analysis of data obtained from the nationally representative data in the East Africa DHS dataset was population-based with high response rate. The sample size used is large enough to detect the association factors with the high power of the study. Hence, this study is beneficial to inform policymakers and planners on their intervention line up.
Limitations of the study include as in any cross-sectional nature of the study design, the finding from this study may not be found a true causal association between the home delivery and covariate. Data were collected based on self-report from mothers within 5 years prior to the survey, and this could be a potential source of recall bias. There was no information on numerous other important factors in the use of maternal health services during childbirth, including the existence of emergencies during home delivery that require professional assistance and outcomes from previous use of health services. Furthermore, some important factors such as antenatal care and obstetric histories are not included in the analysis, as there was no similar definition or classification among the included countries. Since some countries have no DHS program, some countries have limited data access, and some excluded due to the old survey (more than 10 years), the result of this study may not be representative of the entire East African zone.
Conclusion
Home delivery was varied between countries of the East African zone. Home delivery was significantly increased among women with middle-aged, high number of ever born children, rural residence, never married, or formerly married participants. On the contrary, home delivery decreased with higher educational level, media exposure, and higher wealth index.
Wide-range interventions to reduce home delivery should focus on addressing inequities associated with maternal education, family wealth, increased access to the media, as well as narrowing the gap between rural and urban areas, poor and rich families, and married and unmarried mothers.
Footnotes
Acknowledgements
We would like to express our very profound gratitude to the measure DHS for providing us the data for the study area.
Author contributions
Conception of the work, design of the work, acquisition of data, analysis, and interpretation of data were conducted by L.D.R. and B.S.T. Data curation, drafting the article, revising it critically for intellectual content, validation, and final approval of the version to be published were done by L.D.R., A.T., A.B.W., and B.S.T. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
We requested DHS Program, and permission was granted by 149848 reference number to download and use the data for this study from ![]() . Informed consent was not sought for the present study because it is secondary data analysis. There are no individual identifiers reported in any part of this manuscript. All the data management and analysis strictly followed the standard indicated in the manuals of DHS.
. Informed consent was not sought for the present study because it is secondary data analysis. There are no individual identifiers reported in any part of this manuscript. All the data management and analysis strictly followed the standard indicated in the manuals of DHS.
Availability of data and materials
All necessary information was included with the manuscript. The preprint is available on research square.