
Abstract
Objective:
This study aimed to determine the burden of diabetic peripheral neuropathy and its associations with overweight/obesity and impaired blood glucose among diabetic patients in Eastern Ethiopia.
Method:
A total of 644 diabetic individuals were included in the study through systematic random sampling techniques. The Michigan neuropathy screening instrument was used to evaluate the presence of diabetic neuropathy. Data were presented using narrative, figures, and tables from the results of statistical analysis. The descriptive result was reported using frequency (percentage) for categorical variables and mean ± SD for continuous measures, respectively. Multivariable logistic regression was performed to identify factors associated with diabetic peripheral neuropathy.
Results:
The overall prevalence of diabetic peripheral neuropathy was 47.8% (95% CI: 43.9%–51.7%). Low monthly income (AOR: 2.02, 95% CI: 1.09, 3.73), history of khat chewing (AOR: 2.32, 95% CI: 1.04, 4.907), impaired blood glucose (AOR: 1.52, 95% CI: 1.63, 1.94), physical inactivity (AOR: 2.76, 95% CI: 1.74, 4.36), and raised body mass index (AOR: 2.45, 95% CI: 1.01, 4.99) were factors significantly associated with diabetic peripheral neuropathy.
Conclusion:
The study emphasizes the value of early diabetic peripheral neuropathy detection and the widespread presence of diabetic peripheral neuropathy risk factors in diabetes patients. Any initiative intended to lessen the burden of diabetic peripheral neuropathy-related morbidity and high health care costs must be implemented as a strategy.
Introduction
Diabetic peripheral neuropathy (DPN) is one of the most debilitating and distressing effects of diabetes mellitus. 1 Important sensations in the extremities, like touch, position, temperature, and pain, are not felt by diabetic individuals with nerve function impairment, which leads to unnoticeably lost limbs.2 –4
The possible mechanisms of DPN development are multi-dimensional. Increased glucose entry into the nerves under conditions of high blood sugar causes the glycolytic pathway to become saturated and prevents the synthesis of adenosine triphosphate, which affects the speed of nerve signal transmission and the structural integrity of the nerves.5,6 Reactive oxygen species, which are a set of inflammatory cascades that result in neuronal damage and death, are produced by persistently elevated blood glucose. Additionally, under conditions of raising blood glucose level, the protein structure of neuron reacts with the glucose. 7 This peripheral nerve fiber modified by advanced glucose end products is vulnerable to macrophage phagocytosis and contributes to segmental degeneration, which reduces nerve signal transmission.8 –10
The burden of DPN across 23 studies in Africa was 46%. 11 In sub-Saharan Africa, the prevalence is quite different and ranges from 50.7% to 56.2%, as reported by Ghana and Yemen, respectively.12,13 Even though there were lots of inconsistent reports, glycemic control, duration of diabetes, and socioeconomic factors affect the prevalence of DPN.14 –16
In general, the burden of diabetic neuropathy and its determinant factors in diabetic patients has been less reliably quantified in Ethiopia. Therefore, the aim of our study was to determine the magnitude and determinant factors of DPN among patients with diabetes attending public hospitals in Dire Dawa, Eastern Ethiopia.
Methods and materials
Study area and period
A facility-based cross-sectional study was conducted at Dire Dawa public hospitals (Dilchora and Sabian Hospitals) from October 29, 2022, to January 25, 2022. Dire Dawa City is located in the eastern part of the nation’s capital city, Addis Ababa. 17 For the catchment population, the urban area has one general hospital, one reference hospital, eight health centers, and three private hospitals. Dilchora (referral) and Sabian (general) hospitals provide inpatient and outpatient health care services, including diabetic care and follow-up.
Source population
All diabetic patients attending diabetic clinics in Dire Dawa public hospitals were the source population.
Study population
All selected diabetic patients receiving care at public hospitals in Dire Dawa and present during the course of the data collection period were the study population.
Eligibility criteria
All type 1 and type 2 diabetic patients aged 18 years and older receiving care at public hospitals in Dire Dawa diabetic clinics, and at least one prior follow-up visit in each hospital were included. Patients with HIV/AIDS, peripheral nerve injury, leprosy, patients on anti-tuberculosis treatment, stroke, bilateral below-knee amputation, and severe communication impairments were excluded from this study.
Sample size determination
For the first objective (prevalence), the sample size was computed based on a single population proportion formula assuming the prevalence (p) of DPN at 53.6%, 18 with a 95% confidence interval and a 4% marginal error. The derived sample size was 599.

Where; n = sample size required
Za/2 = the value of Z (the standard normal distribution value) at the selected level of significance = 1.96.
p = proportion of peripheral neuropathy among diabetic patients (53.6%).
d = Margin of error = 0.04.

The sample size for the associated factors (second objective) was determined using the double population proportion formula considering the previous study by using open Epi Info statistical software (Manufactured by Disease Control and prevention [CDC, Atlanta]), considering 80% power and a one-to-one ratio 18 (Table 1).
Sample size calculation for factors associated with diabetic peripheral neuropathy, 2022–2023.

AOR: adjusted odds ratio.
We took the largest sample size from the first objective (n = 599). Hence, considering a non-response or refusal rate of 10%, the required sample size was 659.
Sampling technique
A systematic random sampling technique was used to select the study subjects. Based on the hospital’s chronic care registration book, an average of 910 diabetic patients attended Dilchora Hospital in 6 months, compared to 534 patients at Sabian Hospital. The study samples were proportionally allocated to each hospital based on the source population. The number of study participants enrolled in Dilchoral Hospital was (659/1444) × 910, or 414. Moreover, the number of study participants enrolled in Sabian Hospital was (659/1444) × 534, or 245. By dividing the average number of patients attending the clinic in a month by the sample size (N/n), every second eligible participant was selected until the desired sample size was achieved.
Data collection tool and procedures
Data were collected using a structured questionnaire through face-to-face interviews, patient record reviews, and a physical examination. The questionnaire contains socio-demographic factors, the Michigan neuropathy screening instrument, behavioral characteristics, and some clinical variables. The questionnaire (the Michigan neuropathy screening instrument) was validated with sensitivities of 79%, and specificities of 91% respectively.3,14,19 –21 It is a noninvasive and inexpensive measurement tool that evaluates sensory and motor components of neuropathy and contains history and physical assessment parts.7,22
Michigan neuropath screening Instrument (MNSI) history version: It contains 15 items that were administered by the interviewer, of which 13 assess symptoms of DPN, while item number 4 is a measure of impaired circulation and item number 10 is a measure of general asthenia; hence, it was not included in the scoring. The total score ranges from 0 to 13 points, and a score of ⩾7 indicates the presence of DPN.
MNSI examination and scoring: It assessed the following five variables on each foot, which were performed by a physiotherapist.
Physical examination of the feet, which is scored for abnormalities of appearance (deformities, infection, and dry skin/callus), presence of ulcers, vibration perception at the distal great toe, ankle reflexes, and pressure sensation (monofilament).
Scores assigned during the procedure include appearance of feet (normal = 0, abnormal = 1), ulceration (absent = 0, present = 1), ankle reflexes (absent = 1, present with reinforcement = 0.5, present = 0), vibration perception (absent = 1, reduced = 0.5, present = 0), and monofilament test (absent = 1, reduced = 0.5, present = 0). 23
The participants’ weights were determined using a calibrated weighing scale while they were not wearing heavy clothing or shoes. An upright standing stance was used to measure height using a conventional height measurement scale in meters. Body mass index is calculated by dividing a person’s weight (in kilograms) by the square of their height (in meters). Using a measuring tape, the waist circumference was measured in centimeters at the horizontal plane halfway between the lower margin of the ribs and the upper border of the iliac crest.
Using a calibrated sphygmomanometer and a stethoscope, blood pressure was measured on the left arm in millimeters of mercury with the subject seated in a chair after 5 min of rest. For data gathering, BSc nurses and a public health officer were recruited. On the day of the survey, fasting blood sugar (FBS) readings were taken, and with informed agreement, FBS readings from the preceding month were retrieved from a medical record.
Study variables
List of study variables (Table 2).
List of study variables for diabetic peripheral neuropathy.

Operational definition
Controlled blood glucose was indicated when FBS results were less than 130 mg/dl (i.e., an average of two visits), whereas uncontrolled or impaired blood glucose level was considered when a parameter was 130 mg/dl and beyond.
Participants in the study were considered physically active if they had engaged in brisk walking or carrying light loads for 150 min a week, or if they had engaged in running, carrying or lifting heavy loads, digging, or construction work for the past 3 months. Physically inactive participants were not classified as either of the above. 24
Participants in the study who had ever attempted to smoke cigarettes (once or twice) were considered smokers. A study participant was considered a “current smoker” if they had smoked cigarettes at least once during the month (30 days) before the survey. 25
Alcohol consumption: Men consumed an average of six drinks per occasion in the 30 days preceding the study, while women consumed an average of four drinks per occasion. 26
Khat chewing: A person who has used khat at any point in their lifetime is referred to as a khat chewer. Those who had used Khat within the previous month of the poll were considered to be current users. Current users were divided into frequent and infrequent users. Habitual khat users were those who chewed the drug at least three times a week, while occasional users were those who did so occasionally. 27
DPN: The patient’s history version of the MNSI questionnaire score was 7 and above for abnormal responses in the legs (feet) and/or the lower extremity examination version of the MNSI score was 2.5 and above in the legs. The diabetic patient was considered to have DPN. 22
Data quality
The data collection tool prepared in English was translated into local languages and retranslated back to English. The data collectors received 2 days of instruction on the study’s goal, measurement method, and ethical considerations. All questionnaires were checked daily for completeness, accuracy, and clarity by the investigators. A pre-test of the data collection tool (questionnaire) was done by pre-testing 5% (33 individuals) of the study participants at Dire Dawa Health Center. Furthermore, the data were checked during entry and compilation before analysis.
Data analysis procedure
The collected data were checked for completeness, coded, and then entered into the statistical package for social sciences (SPSS) Version 21 (IBM SPSS Modeler, 2013) for summarization and analysis of the data. Frequencies, means, and proportions were used for the descriptive analysis of the data. A binary logistic regression model was used to describe the association between outcome variables and explanatory variables. After bivariate logistic regression, variables with a p ⩽ 0.25 were entered into a multivariate logistic regression model to identify the independent contribution of each explanatory variable. Adjusted odds ratios and their corresponding 95% CI were reported to assess the association between individual variables and the outcome variable. p < 0.05 was considered statistically significant.
Results
Socio-demographic variables
In this study, a total of 644 diabetic patients were interviewed out of 659, with a response rate of 97.72%. The factors contributed to the non-respondents: three study participants declined to take part, four were HIV positive, two had preexisting neurological issues, and the remaining six people lost their earlier FBS test results. The mean age of the participants was 54.1 ± 7.44, and 52.2% of the study participants were female. More than half of the participants were married (54.0%), and nearly two-thirds (65.8%) of the participants were of urban residence. Nearly half of the study participants, 315 (48.9%), attended formal education, and 200 (31.1%) earned less than 1000 birr per month (Table 3).
Socio-demographic characteristics of respondents attending chronic care in Dire Dawa public hospitals in Eastern Ethiopia, 2022–2023 (n = 644).

Medical and lifestyle-related characteristics of the study participants
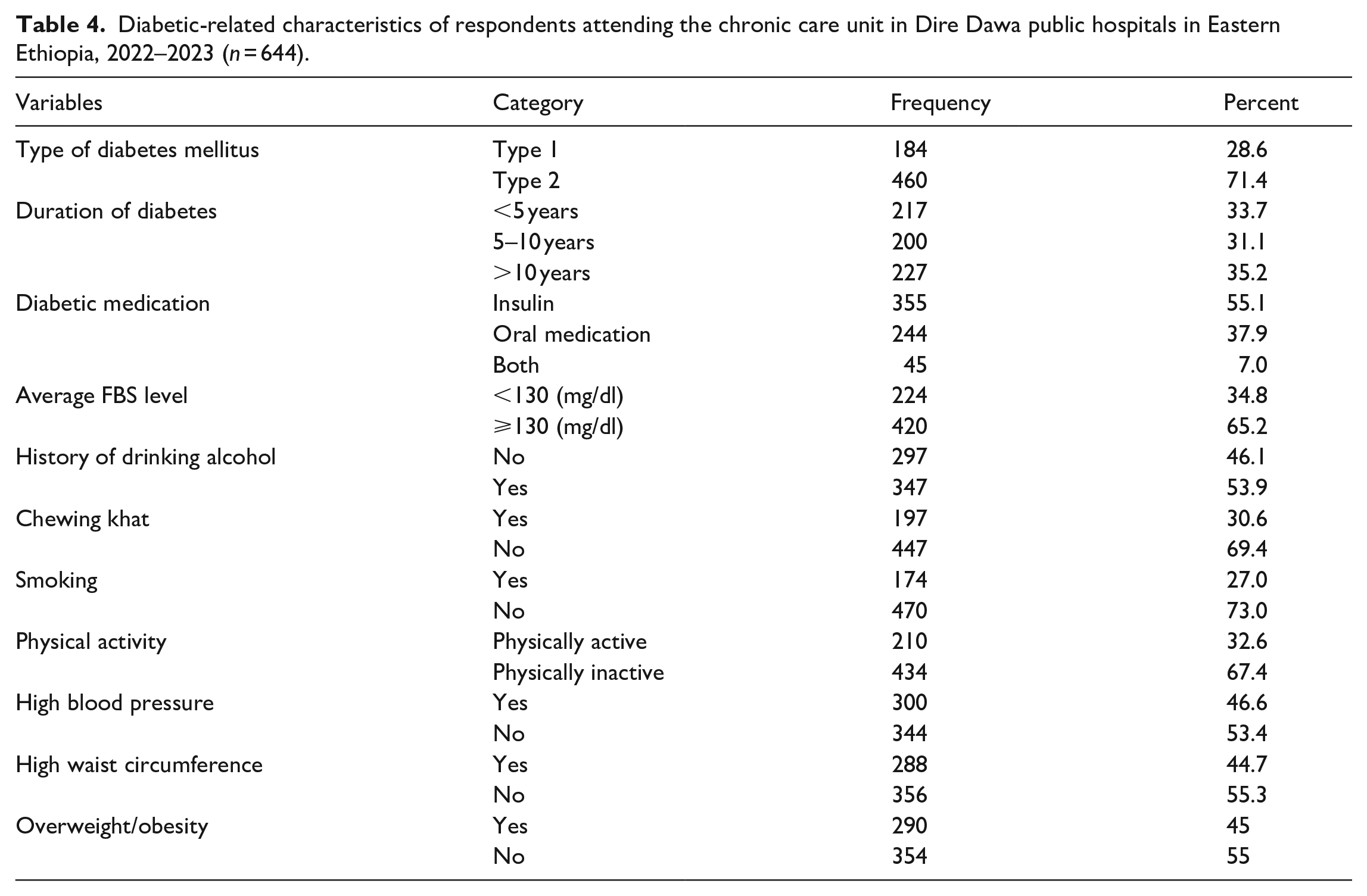
More than a quarter (28.6%) of respondents had type 1 diabetes. Moreover, 35.2% of the participants stayed with diabetes for longer than 10 years. Almost more than half of the subjects were drinking alcohol (53.9%), 447 (69.4%) chewed khat, and nearly one-fourth (27.0%) of the participants had smoked a cigar. Likewise, 290 (45%) study participants had a body mass index of 25 kg/m2 or more (overweight or obesity), and 300 (46.6%) were hypertensive (BP 140/90) (Table 4).
Diabetic-related characteristics of respondents attending the chronic care unit in Dire Dawa public hospitals in Eastern Ethiopia, 2022–2023 (n = 644).
Prevalence of DPN
The prevalence of DPN was determined for each study participant using the combined MNSI symptom and sign scores. The MNSI tool for diabetic neuropathic symptoms was used to define neuropathy as a score greater than or equal to 7 (out of 13) or a score of 2.5 (out of 10) on a physical assessment for neuropathy. The overall prevalence of DPN among the study population was 308 (47.8%) (95% CI: 43.9%–51.7%). Based on the symptom score, the prevalence of DPN was 248 (38.5%), while it was 279 (43.3%) based solely on the physical examination score (Table 5).
The prevalence of diabetic peripheral neuropathy among diabetic patients attending Dire Dawa public hospitals in Eastern Ethiopia, 2022–2023 (n = 644).
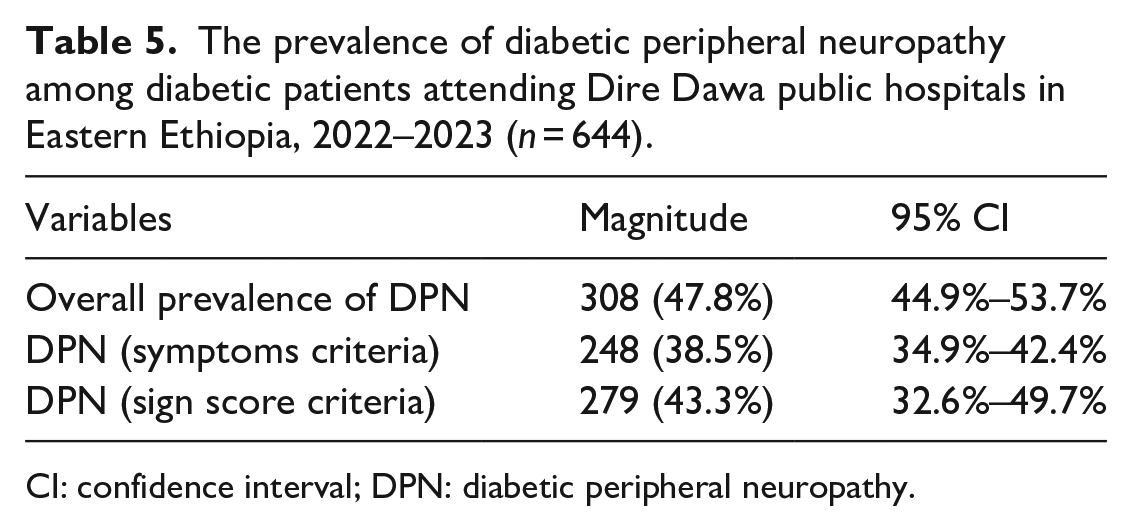
CI: confidence interval; DPN: diabetic peripheral neuropathy.
Factors associated to DPN
At bivariate analysis, age over 40 years, male sex, being married, urban residence, monthly income, duration of diabetes, alcohol consumption, history of khat chewing, status of physical activity, poor glycemic control, comorbid hypertension, waist circumference, and body mass index were significantly associated with DPN (p ⩽ 0.25).
In multiple logistic regression, participants who have a monthly income of less than 1000 birr were two times (AOR: 2.02; 95% CI: 1.09, 3.73) more likely to have DPN than those study participants with an income of more than 3000 birr. Similarly, participants who had a history of khat chewing were 2.32 times (AOR:2.32, 95% CI: 1.04, 4.907) more likely to have DPN than those who did not chew khat. Moreover, participants who were physically inactive were nearly three times (AOR: 2.76; 95% CI: 1.74, 4.36) more likely to have DPN than physically active study participants. Furthermore, participants with impaired blood glucose levels were 1.52 times (AOR: 1.52, 95% CI: 1.63, 1.94) more likely to have DPN than those with controlled blood glucose level. Similarly, study participants who had a raised body mass index were 2.45 times (AOR: 2.45, 95% CI: 1.01, 4.99) more likely to have DPN than their counterparts (Table 6).
Factors associated with diabetic peripheral neuropathy among diabetic patients attending Dire Dawa public hospitals in Eastern Ethiopia, 2022–2023 (n = 644).
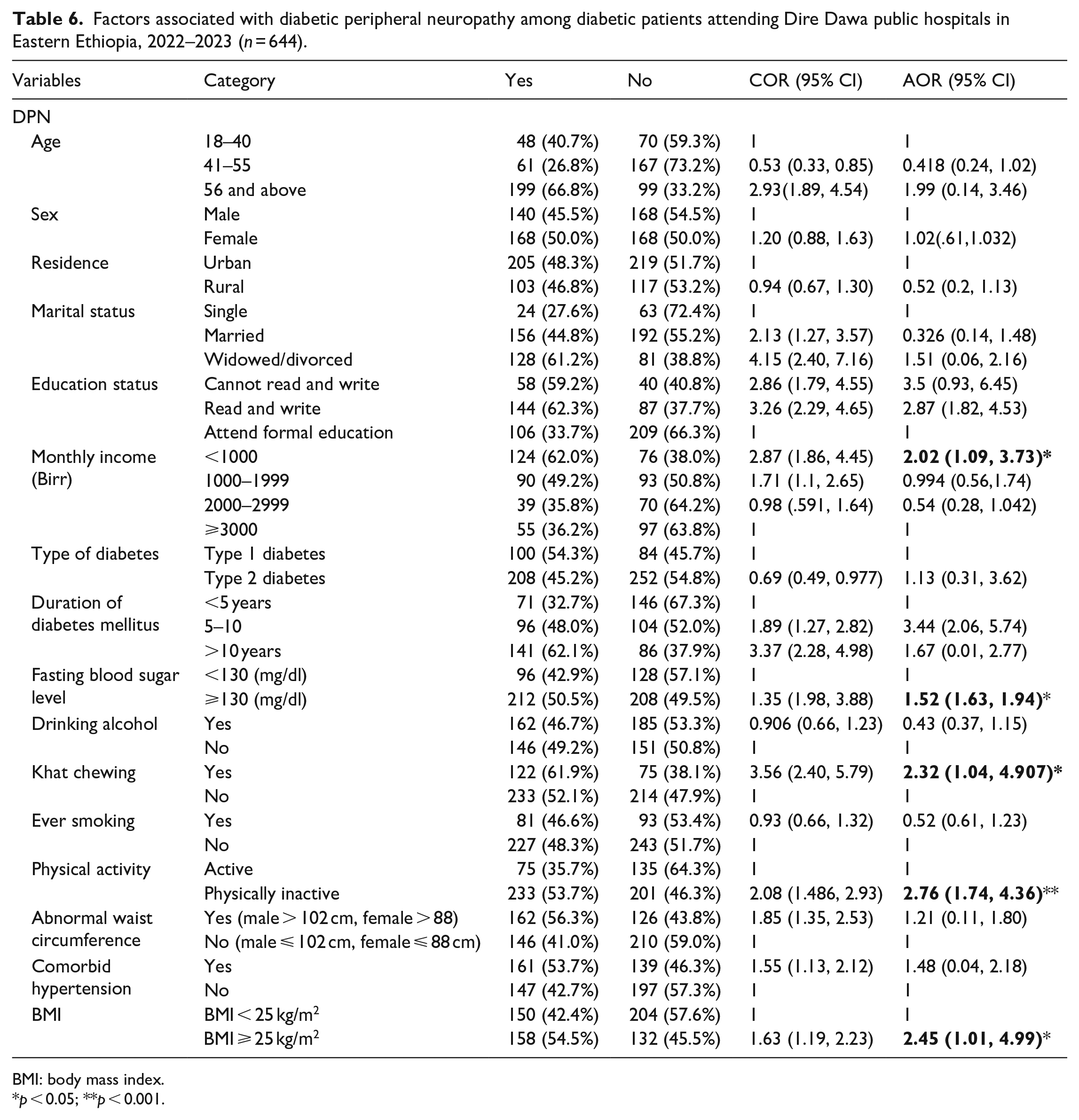
BMI: body mass index.
p < 0.05; **p < 0.001.
Discussion
We investigate the magnitude of DPN and its associated factors among diabetic patients, which had previously been reported only infrequently. In this study, the magnitude of DPN was 47.8%. Low monthly income, history of khat chewing, physical inactivity, comorbid hypertensive illness, and raised body mass index were independent predictors of DPN.
In our study, we found that the overall magnitude of DPN was 47.8% (95% CI: 44.9%–53.7%). A similar finding was reported in a study conducted in Ghana (50.7%), 13 Nigeria (39.7%), 28 Bahirdar (52.2%), 29 and Jimma university Medical Center (53.6%), 18 However, it is lower than the studies conducted in Benin (88.7%), 30 and Yemen Aden Diabetic Center (56.2%). 12 On the other hand, this finding was relatively higher than studies conducted in India (31.1%), 31 Morocco (15%), 32 Tanzania (13.6%), 33 and Uganda (29.4%). 34 The disparities might be explained by the use of various measurement tools and the recruitment of numerous critically ill individuals with complicated medical conditions. For instance, in the case of northern Tanzania, they used the Toronto Clinical Scoring System DPN assessment tool, and the mean age of the study participants was 57.2 years.
The current study discovered that patients with low monthly income (less than 1000 birr) were twofold more likely to have DPN than those who had earned more than 3000 birr. This finding is consistent with a study from Iran 35 and Egypt. 36 This could be explained as those poorly paid study participants are unable to access better diabetic health care and a healthy diet, and concomitant daily income-related stress aggravates the occurrence of DPN. However, this finding is in contrast with most of the studies done on the association between DPN and monthly income status.18,29 This could be due to the level of socioeconomic status, the time of the study, or the sample size variation across different studies.
The likelihood of diabetic neuropathy was 52% (AOR: 1.52) higher in patients with impaired blood glucose status compared to patients with controlled blood glucose levels. This was in accordance with the results of other studies in Nigeria, 28 Tanzania, 33 and southern Ethiopia. 14 This may be due to the fact that prolonged, unchecked high blood glucose levels cause the creation of additional neuropathogenic added sugar, which weakens the integrity of neurons.5,7 Similarly, studies indicated that cathinone released when chewing khat has a catecholamine-like effect on glucose by raising blood glucose levels and perhaps by lessening the effects of insulin on the target tissues. Additionally, cathinone reduces the activity of enzymes that metabolize free radicals, intensifying oxidative stress, which is a critical factor in the onset of diabetes and its complications.38,39 In this study, people with a history of khat chewing were 2.32 times more likely to have DPN compared to non-chewers. This finding is comparable with a meta-analysis and cross-sectional studies done in Saudi Arabia and Yemen.40,41 Multiple study findings reported that cathinone released from khat chewing has an amphetamine-like effect on carbohydrate metabolism, increasing blood glucose levels, possibly by reducing the effects of insulin on the target tissues, which is indirectly related to high hyperglycemia-related neuropathy. Furthermore, cathinone decreases the activity of free radical metabolizing enzymes thereby heightening oxidative stress, which has a vital role in the development of diabetes and diabetes-related complications.41,42
In agreement with other reports, our data showed that study participants not involved in physical activity were almost three times more likely to have DPN compared to physically active study participants.15,42 This could be explained by the fact that physical activity increases muscle size, capillary number, and insulin sensitivity in peripheral tissue, all of which work together to lessen neuronal damage or neuropathy.43,44
Moreover, diabetic participants with a high body mass index (BMI ⩾ 25 kg/m2) were 2.45 times more likely to develop DPN compared to those with a normal body mass index. This finding is consistent with the findings from India, 31 Yemen, 12 and north-west Ethiopia. 29 This could be explained by having a high body mass index, which encourages chronic low-grade inflammation and insulin resistance by increasing the release of interleukin-6 and tumor necrosis factor alpha. 45 However, this study is inconsistent with the findings from Nigeria 28 and south-west Ethiopia. 18 . The disparities might be due to variations in levels of physical activity, healthcare utilization behavior, socioeconomic status, and outcome measurement tools. For example, in south-west Ethiopia, DPN was assessed by non-standard tools, including history and physical examination.
Limitation of the study
A few methodological limitations should be taken into consideration when interpreting and evaluating the results of this study. The glycemic control status was measured using the average of two consecutive fasting blood glucose levels instead of considering the gold standard HbA1C due to a lack of resources. Non-response bias, where non-responders may differ from survey respondents in specific ways, is another flaw in our study. It was also challenging to adequately account for the quantity and duration of khat chewing.
Conclusions
DPN was prevalent and predicted by patients with low monthly income, a history of khat chewing, a raised body mass index (⩾25 kg/m2), not being involved in physical exercise, comorbid hypertension, and impaired glucose control.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231220784 – Supplemental material for Diabetic peripheral neuropathy and their associations with overweight/obesity and impaired blood glucose among diabetic patients in Eastern Ethiopia: Institutional-based study
Supplemental material, sj-docx-1-smo-10.1177_20503121231220784 for Diabetic peripheral neuropathy and their associations with overweight/obesity and impaired blood glucose among diabetic patients in Eastern Ethiopia: Institutional-based study by Dilnessa Fentie, Yonatan Solomon, Fitsum Abebe, Tariku Derese, Feven Tigstu and Tekleberhan Hailemariam in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank Dire Dawa regional health Beuro chief executive officers, the study participants, and data collectors for their unlimited support.
Author contributions
DF and YS: wrote the original draft, developed the methodology, and were involved in project supervision. FA and TD: analyzed the data and distributed resources. FT and TH: wrote the main manuscript text. All authors reviewed the manuscript.
Ethical approval and consent to participate
The study was done in accordance with the Helsinki Declaration on Studies on Human Study Participants. Ethical clearance was obtained from the Institutional Review Board (IRB) at Dire Dawa University (protocol number DDU-IRB-2022-102). Participants were informed about the purpose, objectives, and their right to participate or not in the study. Informed written consent was obtained from the study participants to start data collection. For illiterate study participants, the data collectors read the consent form and the protocol of the study. Subsequently, each study participant provided their informed consent and inked fingerprints to participate voluntarily in the study.
Declaration of conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Dire Dawa University under an annual competitive research grant. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data availability statement
All relevant data is included within the paper and its supporting information files.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.