
Abstract
Objectives
Maintaining good oral health after stroke is challenging due to physical and cognitive impairments and hospital-related factors. This study aimed to understand the oral and/or denture care (ODC) practices of healthcare professionals (HCPs) and explore the oral health and ODC experiences of stroke survivors (StS).
Methods
We used a mixed-methods approach. Quantitative data were derived from a survey of HCPs in acute stroke care and rehabilitation and from a retrospective chart review of admissions over one year. An embedded qualitative multiple case study with StS admitted to rehabilitation gathered information from care observations, oral examinations, semi-structured interviews, and charts.
Results
The survey involved 32 HCPs. All believed that ODC was part of self-care and over 90% believed that toothbrushing helps patients feel better and provides comfort while eating. However, 59% indicated insufficient training to perform oral health assessments and provide ODC. The chart review included 168 charts: 103 from acute care and 65 from rehabilitation. Notations about patient oral health status were written by nurses or speech-language pathologists in 46% and 65% of acute care and rehabilitation charts, respectively. ODC occurred less than once/day in acute care. In rehabilitation, occupational therapists assessed ODC functions in 55% of patients, but documentation of ODC provision was lacking. Qualitative themes from the case study included i) Valued oral health and ODC, ii) Independent ODC before stroke, iii) inconsistent support for ODC in acute care, iv) increased self-efficacy despite irregular ODC during rehabilitation, and v) ongoing reliance on caregivers or staff for ODC.
Conclusions
This study identified significant gaps in oral health and ODC practices during post-stroke hospitalization despite attention to oral health from HCPs. Both settings lacked evidence-based ODC approaches tailored to patient needs. We advocate for protocols that include oral screening tools, promote twice-daily toothbrushing, and incorporate ODC education for HCPs, StS, and caregivers.
Keywords
Introduction
Stroke is a global leading cause of death and disability. 1 In Canada, more than 400,000 people live with long-term disabilities 2 and half need assistance with activities of daily living (ADLs). 3 ADLs are essential tasks which include personal hygiene such as oral and/or denture care (ODC). ODC involves sequential activities requiring motor dexterity, perceptual capacities, and sensory integrity. Stroke can adversely affect these domains due to the abrupt onset of functional impairments, posing serious challenges to independent ODC in stroke survivors (StS).
Motor impairments affecting the limbs and face occur in 80% of StS 4 and impact ODC performance. 5 For example, holding a toothbrush can be hard for StS even six months after stroke. 6 Mandibular and facial paresis can cause difficulty swallowing, 7 while tongue weakness can hinder post-swallow oropharyngeal clearance. 8
Perceptual impairments, such as hemispatial neglect, can also lead to poor oral hygiene. 9 To illustrate, difficulty with internal and external spatial orientation can compromise responsiveness to stimuli on the side opposite the stroke lesion, 10 exacerbating issues with unilateral facial awareness. This could lead to poor recognition of food pocketing in the lateral sulci of the paretic side and also compromise ODC efficiency. 11 Concomitant to potential motor weakness and perceptual limitations, some StS may have sensory loss that could grossly impact oral care behaviours and/or cause dysphagia. 12 Dysphagia affects almost half of StS 13 and may render oral care unsafe, warranting special consideration for practice including healthcare professional (HCP) education. 14 Furthermore, post-stroke cognitive impairments may induce overlaid impacts on dysphagia and ODC. Neurocognitive disorders (NCD) are frequent after stroke 11 and even mild NCD incurs infrequent toothbrushing, tooth loss, 12 and poor oral health, 13 while major NCD (dementia) may compromise both independent ODC and ODC provision. 14
Additional stroke-related conditions may further hinder oral and denture care. Orofacial/oral apraxia, reported in approximately 35% of stroke survivors, 15 impairs the ability to plan and sequence voluntary oral movements essential for swishing, rinsing, and spitting. Post-stroke depression, affecting an estimated 17% of survivors, 16 may reduce motivation and adherence to hygiene routines and has been associated with poorer oral health outcomes.17,18 Fatigue—experienced by nearly half of stroke survivors 19 —can limit participation in activities of daily living, constrain cooperation with care providers, and reduce opportunities for assisted ODC. Together, these conditions may compound motor, sensory, and cognitive impairments, increasing stroke survivors’ dependence on healthcare professionals for effective ODC.
Consequently, during hospitalization and rehabilitation, many StS become dependent for ODC. 20 Although nurses acknowledge the importance of ODC after stroke, barriers such as lack of knowledge/training,5,7 time constraints, 21 and prioritization of other care activities 21 may hinder their ability to provide the support StS need for ODC. StS′ oral health may therefore deteriorate during hospitalization, 22 leading to dental caries, tooth loss, 23 increased risk of malnutrition, 24 and poorer overall patient outcomes. 25 Inadequate oral care can increase bacterial accumulation and cause gum infection (periodontitis), which itself has been associated with stroke risk. 26 This raises the risk of aspiration pneumonia, 27 especially in dysphagia cases, increasing hospital stay 28 and mortality rates. 29
On the other hand, good oral health can benefit StS during their recovery. A healthy oral cavity enhances eating by increasing saliva production 30 and enabling chewing, 12 improving swallowing safety and promoting oral nutritional intake. Good oral health also has positive effects on well-being, 31 self-esteem, and social interactions. 32 Thus, the prevention and treatment of oral pathologies help mitigate the systemic complications of stroke and enhance general health and participation. 31
While there is evidence of the importance of post-stroke ODC, care provision varies across healthcare institutions. 21 Guidelines and protocols are scarce,20,33 and basic information about the frequency of care provision and advisable cleaning products are inconsistent.21,34,35 Canadian guidelines recommend oral health assessments 36 and ODC,36,37 but lack further specifications for HCPs. Our purpose was to describe current ODC practices among HCPs and to explore the oral health experiences of StS across acute care and rehabilitation. The goal was to identify gaps that could inform the future development of evidence-based oral healthcare protocols.
Methods
This research was guided by Social Cognitive Theory, which posits that health behaviours are influenced by self-efficacy, outcome expectations, health goals, and sociostructural factors. 38 Focusing on self-efficacy – the individual’s belief that they can successfully perform ODC – we selected “experience” and “beliefs” as potential influencers for patients’ and HCPs’ oral health behaviours 39 (Supplementary Figure 1). “Knowledge”, although not depicted as a core construct in the Social Cognitive Theory model, is explained as a precursor to self-efficacy and was therefore added explicitly as a construct, since deficits in oral health knowledge and training are consistently identified in the literature as major barriers to HCPs’ confidence and behaviour.
To better understand ODC practices and experiences using the Social Cognitive Theory constructs, we applied a mixed-methods design with a concurrent embedded approach. 40 In this design, the quantitative component served as the primary strand, while the qualitative multiple case study was embedded to provide contextual insight into stroke survivors’ and caregivers’ experiences. Although the quantitative results are presented first due to their primary role, data collection for the survey, chart review, and case study occurred within the same overall timeframe. The primary method was quantitative and included a retrospective chart review (hereafter, chart review) and a prospective oral health and care survey of HCPs (survey), both conducted at an acute care hospital and an in-patient rehabilitation facility. The secondary method was a qualitative multiple case study (case study) 41 completed in rehabilitation. The survey, chart review, and case study were designed as complementary components and were not conducted sequentially. Ethical approval was received from both settings (#20200771-01H,#M16-20-028) and University of Ottawa (#H02-21-5972).
The survey included physicians, nurses, speech-language pathologists (SLPs), and occupational therapists working in the two settings during the year of 2021. Dentists were not included because they are not part of the inpatient acute or rehabilitation stroke teams at the participating hospitals and do not provide daily oral care to hospitalized stroke patients. The target sample size for the survey was at least 15 healthcare professionals per care setting, for a minimum total of 30 participants. This threshold is recommended to mitigate undue heterogeneity when examining multiple variables in applied health research. 42 The survey involved a 45-item questionnaire regarding HCPs’ thoughts and ODC practices. Questions were chosen from previously published questionnaires39,43,44 selected for their alignment with Social Cognitive Theory constructs, a literature review, and expert input. Item formats included multiple-choice, 7-point Likert scale,45,46 and open-ended questions (Supplementary Table 1).
The chart review included 110 stroke admissions randomly selected from consecutive acute care admissions over one year (2021) at the acute care hospital, and 66 admissions from rehabilitation (60 randomly selected from consecutive admissions, plus six from the case study). In consultation with a biostatistician, these sample sizes were determined to allow estimation of ODC rates with a margin of error of ≤5% (T. Ramsay, personal communication, December 13, 2019), while accounting for potential losses due to ineligible cases based on our previous study. 33 Eligible patients included those with confirmed hemorrhagic or ischemic strokes. We developed a data collection manual with operational definitions and a data extraction form including the following variables: patient characteristics, stroke information, impairments (assessed by HCPs), patients’ oral health status, and ODC frequency (available only in acute care). Fifteen percent of charts in acute care underwent independent review by two data abstractors and 10% of rehabilitation charts by two and three data abstractors; the proportions differed across settings due to variations in charting structures and data extraction logistics, and both fall within the common 15% range for reliability checking in retrospective chart reviews. 47
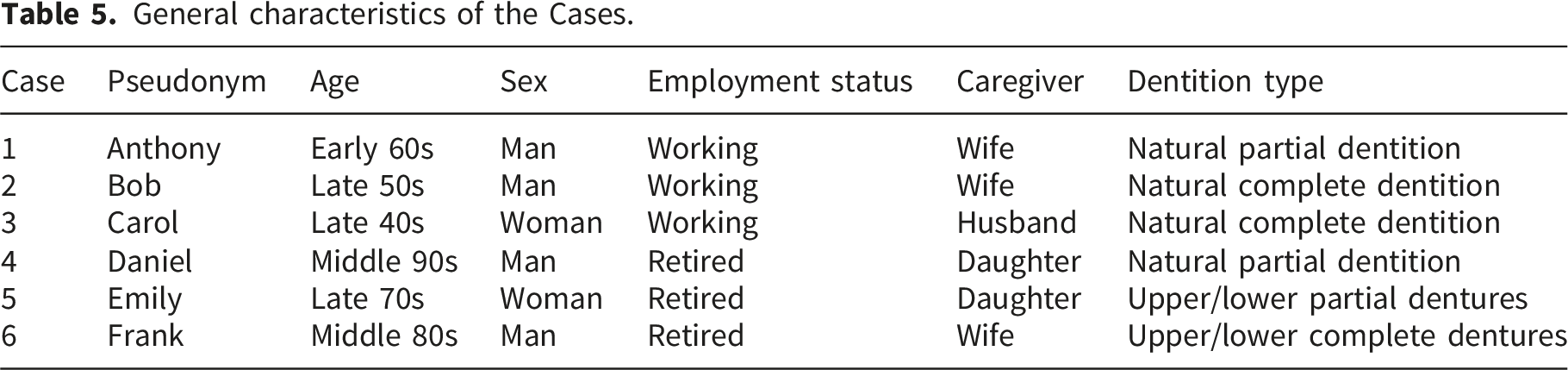
The case study involved a purposive sample of six StS (i.e., Cases) recruited at the rehabilitation facility in 2021. Six stroke survivors were recruited, consistent with Stake’s multiple case study approach, which recommends four to ten cases to support in-depth understanding of the phenomenon of interest. 41 Cases from different age groups, with a particular focus on seniors, and with variation in dentition status were sought. Exact ages were not reported to maintain participant anonymity. Given the small sample size, single-site recruitment, and detailed case descriptions, age ranges were used in accordance with the study’s ethical requirements.
Adult StS were approached in person by a point-of-care health professional based on broad eligibility (adult age, confirmed stroke diagnosis, capacity to consent, and availability of a caregiver), after which the research team assessed final eligibility. Purposive sampling was used to select individuals best positioned to provide detailed accounts of their ODC experiences, consistent with the exploratory and illustrative aims of this case study. To reduce heterogeneity associated with cumulative impairments and prior rehabilitation experiences, only individuals with a first-ever stroke were included, allowing clearer attribution of ODC challenges to a single stroke event. This criterion differed from the chart review, where stroke recurrence status was not consistently recorded. Patients with severe receptive aphasia (assessed by speech-language pathologists) prohibiting interview participation were excluded. Cases were recruited from a rehabilitation program, and interviews explored their oral health and ODC experiences across the full hospitalization trajectory, including their prior acute care stay.
The case study involved four data collection methods by NG-J (a female dentist and researcher, undertaking training in qualitative research during her PhD at the time of the study). Initially, each Case was observed during two full rounds of routine daily nursing care, with observations covering the entire duration of each round and the researcher acting as a complete observer. Observations focused on oral and denture care when present, including care practices, contextual factors, and staff–patient interactions. The first round was conducted with participants blinded to the study objectives. Before round two, they were informed of the objectives and the researcher’s background. NG-J had no prior relationship with participants. Field notes were guided by a structured observation form developed a priori from existing literature48,49 (Supplementary Table 2). Second, NG-J performed oral examinations on StS using The Oral Health Assessment Form for Adults from the World Health Organization (WHO) 50 and The Holistic and Reliable Oral Assessment Tool (THROAT). 51 To avoid pain, she documented three surrogate markers instead of WHO gingival probing: tooth loss, gingival assessment, and tooth mobility. 52 Third, NG-J conducted open-ended semi-structured interviews with the Cases and caregivers. The interview guide (Supplementary Table 3) included questions adapted from the validated questionnaire Oral Health Impact Profile 53 and based on prior studies exploring ODC experiences among StS and HCPs.54,55 Interviews were audio-recorded, conducted once per dyad (StS-caregiver), and lasted approximately 40 minutes. Transcripts were not returned to participants for comment or correction. NG-J took brief notes during the interviews. Finally, she conducted chart audits for each Case using the same procedures as for the chart review.
Data analysis
Survey Likert responses were numerically coded (1-7) and binarized for descriptive commonality (‘agree’ for lowest three, ‘disagree’ for highest three. The middle score (4) was selected in only 5% of all responses and is therefore not reported in the summary; however, the full dataset is available upon request. Open-ended responses were analyzed separately for content related to the Social Cognitive Theory constructs.
The chart review analysis involved descriptive statistics for dependent (e.g., oral care recommendations) and independent variables (e.g., dysphagia). Potential patient overlap between settings precluded inferential statistical tests. Chart review validity followed operational definitions and diagnostic determinations from studies and expert opinion. Reliability involved percent agreement and Cohen’s kappa for data extractors. Because the chart review relied on routine clinical documentation, some variables were not consistently recorded across charts. The chart review manual and data extraction form were comprehensive, and multiple sections of each chart were reviewed to identify the required information. Data points that were not documented were excluded from analyses for that; percentages were calculated using variable-specific denominators, excluding charts with missing or undocumented data for that variable. All analyses were descriptive and based solely on available data.
For the case study, we applied a two-level thematic analysis (intra- and cross-case) 41 using the Framework Method 56 (Supplementary Figure 2). Analytic rigour was ensured through collaborative coding and investigator triangulation. The authors NG-J and RB independently coded all interviews during the first coding cycle and resolved discrepancies through consensus, generating an initial analytical framework (Temporary Codebook 1) This framework was iteratively refined through inductive and deductive coding, with earlier transcripts reviewed to ensure completeness. Codes were examined within each case and then grouped across cases into higher-order categories. New codes and categories emerged through the fifth interview, but none appeared in the sixth, indicating that data saturation was achieved. Contradictory data were retained to inform theme refinement. Based on these categories, NG-J developed the themes, which were reviewed by KSS and HF to explore alternative interpretations and enhance credibility. 56 Data from interviews, observations, oral examinations, and chart reviews were triangulated by cross-verifying information from these multiple sources to strengthen Case interpretation and analytic consistency. 41 NG-J and RB coded the Cases, NG-J created themes, and KSS and HF reviewed codes and themes. 57 Participants did not provide feedback on the findings. Data were managed using NVivo® and Excel®. NG-J maintained a reflexive diary to account for personal bias, enhancing transparency and credibility. 41
The final mixed-methods analysis involved a description of the quantitative and qualitative components within a concurrent embedded mixed-methods design, where qualitative results supported and enriched interpretation of the quantitative findings. 40
Results
Oral health and care survey
Respondents’ work experience as healthcare professionals and stroke team members.
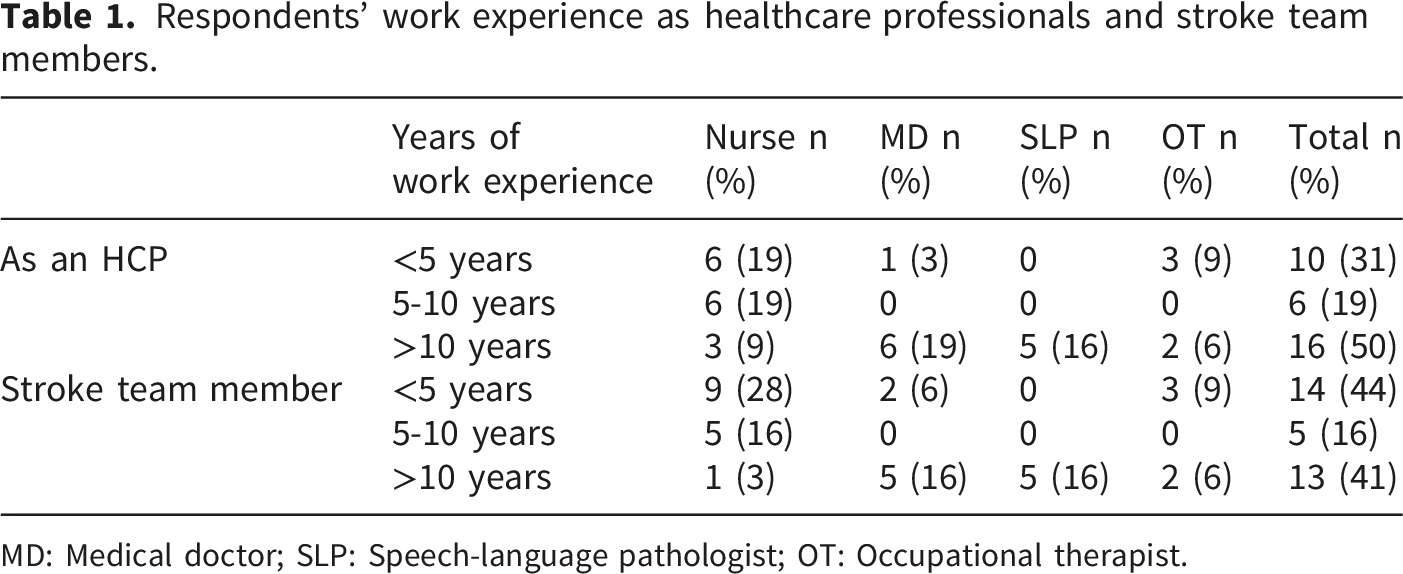
MD: Medical doctor; SLP: Speech-language pathologist; OT: Occupational therapist.
Knowledge, Experience, Beliefs, Self-efficacy: Ninety-one percent of HCPs regarded mouth care as a high priority. All believed that oral care was part of self-care and should include tongue, palate, and gum cleaning. Most considered that toothbrushing would help patients feel better (97%), provide comfort when eating (94%), and prevent oral diseases (97%), while 84% felt that modifications for patients with dysphagia were necessary. In addition, 77% agreed that denture wearers were also susceptible to oral health problems. HCPs agreed with recommendations for toothbrushing twice a day (73%), overnight denture removal (78%), and dental check-ups every six months (56%). However, 53% considered the oral cavity difficult to clean, and 47% found oral care provision unpleasant.
Outcome expectations: All HCPs considered that stroke-induced motor, sensory, and cognitive impairments challenged independent ODC, and 91% believed that poor oral care related to pneumonia.
Sociostructural factors: Fifty-nine percent had not received oral healthcare education or training. Fifty-three percent lacked confidence in performing oral health assessments and 39% felt incapable of delivering good oral care. Workplace barriers reported by respondents were: 72% lacked ODC continuing education, 69% identified missing oral hygiene supplies, and 47% found nurses lacked time for ODC delivery.
Retrospective chart review
A total of 168 charts were reviewed. Eight were excluded given an undetermined stroke diagnosis or other brain pathologies.
Patient characteristics: In acute care, patients averaged 74 (SD=15) years old, with 58% women; in rehabilitation, the mean age was 73 years (SD=12), with 45% women. Supplementary Tables 4 and 5 have additional demographic information and medical history. Dentition type (natural teeth vs. denture) was documented in 32% of acute care charts and 95% of rehabilitation charts. Interrater reliability between data extractors was high, with percent agreement of 93% in acute care and 96% in rehabilitation, and corresponding Cohen’s kappa values of κ = 0.86 and κ = 0.84, respectively.
Stroke features in acute care and rehabilitation facilities.
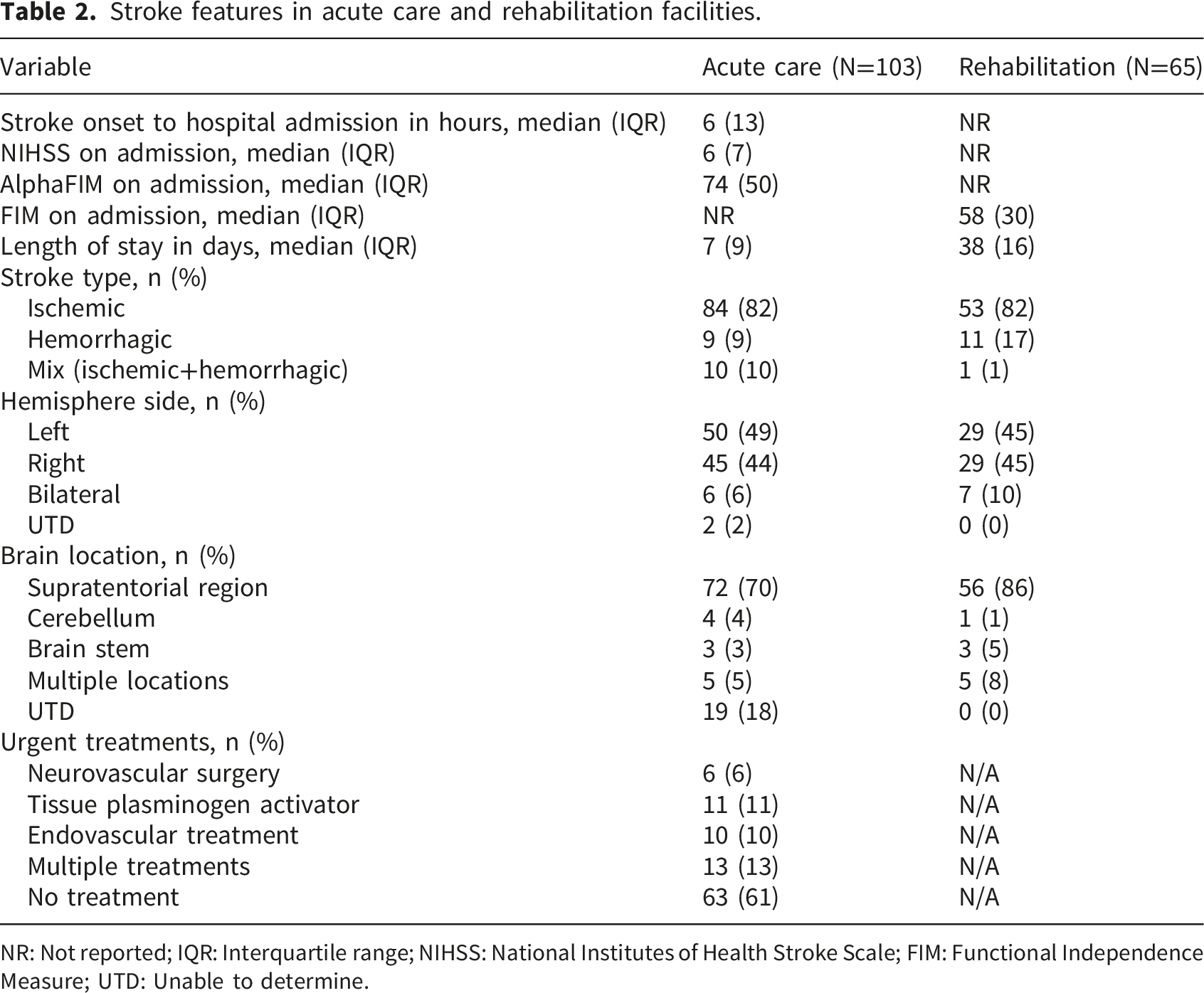
NR: Not reported; IQR: Interquartile range; NIHSS: National Institutes of Health Stroke Scale; FIM: Functional Independence Measure; UTD: Unable to determine.
During hospitalization, infections rates were low and comparable across settings, occurring in 15% of acute care patients and 14% of those in rehabilitation. Urinary tract infections were more common than pneumonia in both settings: 8% vs. 6% in acute care and 8% vs. 3% in rehabilitation.
Dysphagia and oral assessment results in acute care and rehabilitation facilities documented by healthcare professionals.
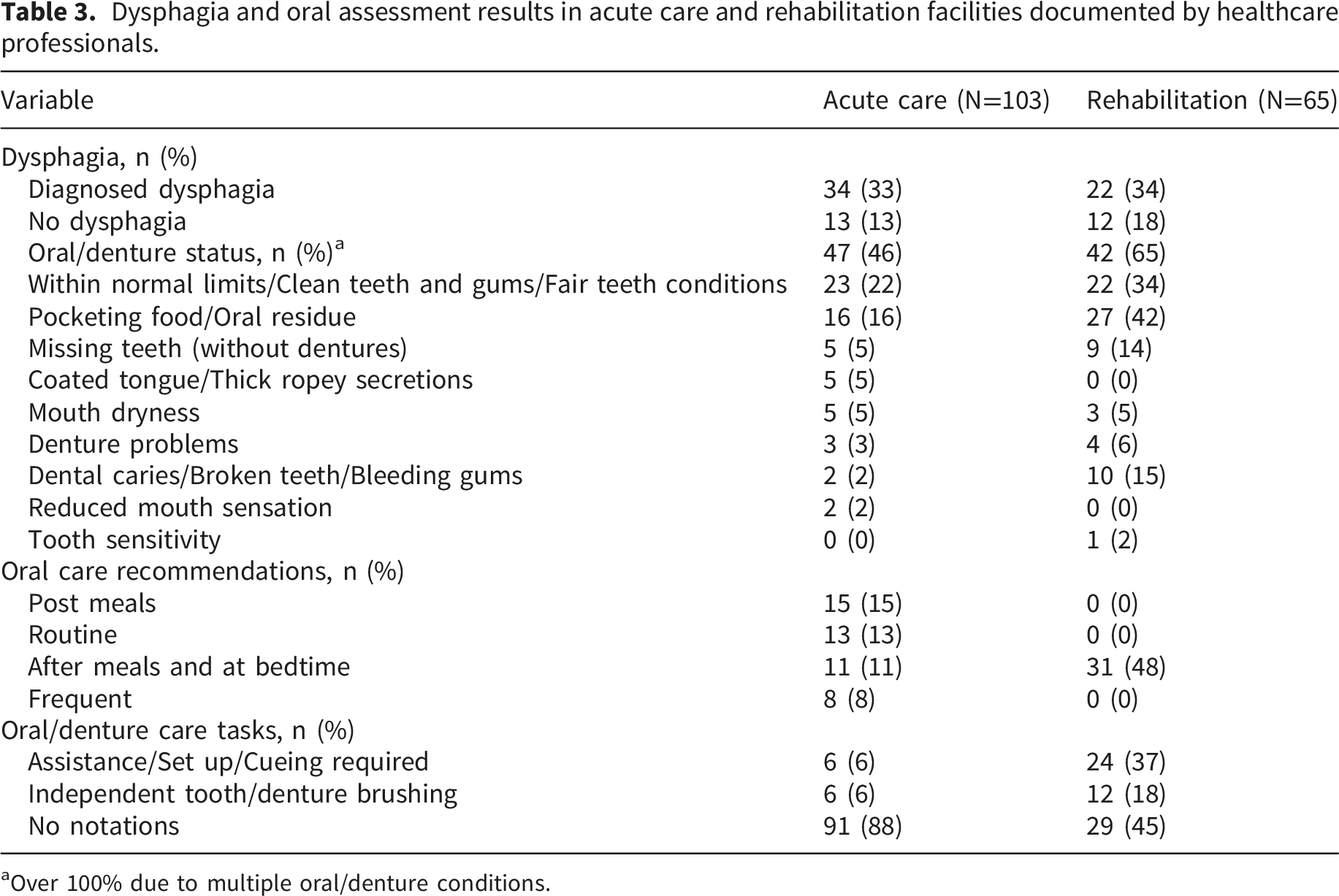
aOver 100% due to multiple oral/denture conditions.
Impairments Relevant to Oral and Denture Care: Other stroke-related impairments affecting ODC were documented across disciplines (physiotherapists, occupational therapists, speech-language pathologists). Arm/hand hemiparesis was common overall but showed a markedly different distribution by setting, affecting 57% of patients in acute care versus 92% in rehabilitation; about half of these cases involved the dominant arm/hand, underscoring the potential impact on fine motor tasks required for ODC. Facial hemiparesis was more frequent in acute care (approximately two-thirds) than in rehabilitation (40%). Ambulatory impairments were widespread, noted in 72% of acute care charts and universal (100%) in rehabilitation. Apraxia (e.g., arm/hand apraxia) was comparatively uncommon and similarly distributed (11% in each setting). Hemispatial neglect or inattention showed a moderate-to-high prevalence with a higher concentration in rehabilitation, documented in 27% of acute care patients and 46% of rehabilitation patients.
Documented instances of oral and/or denture care in acute care hospital.
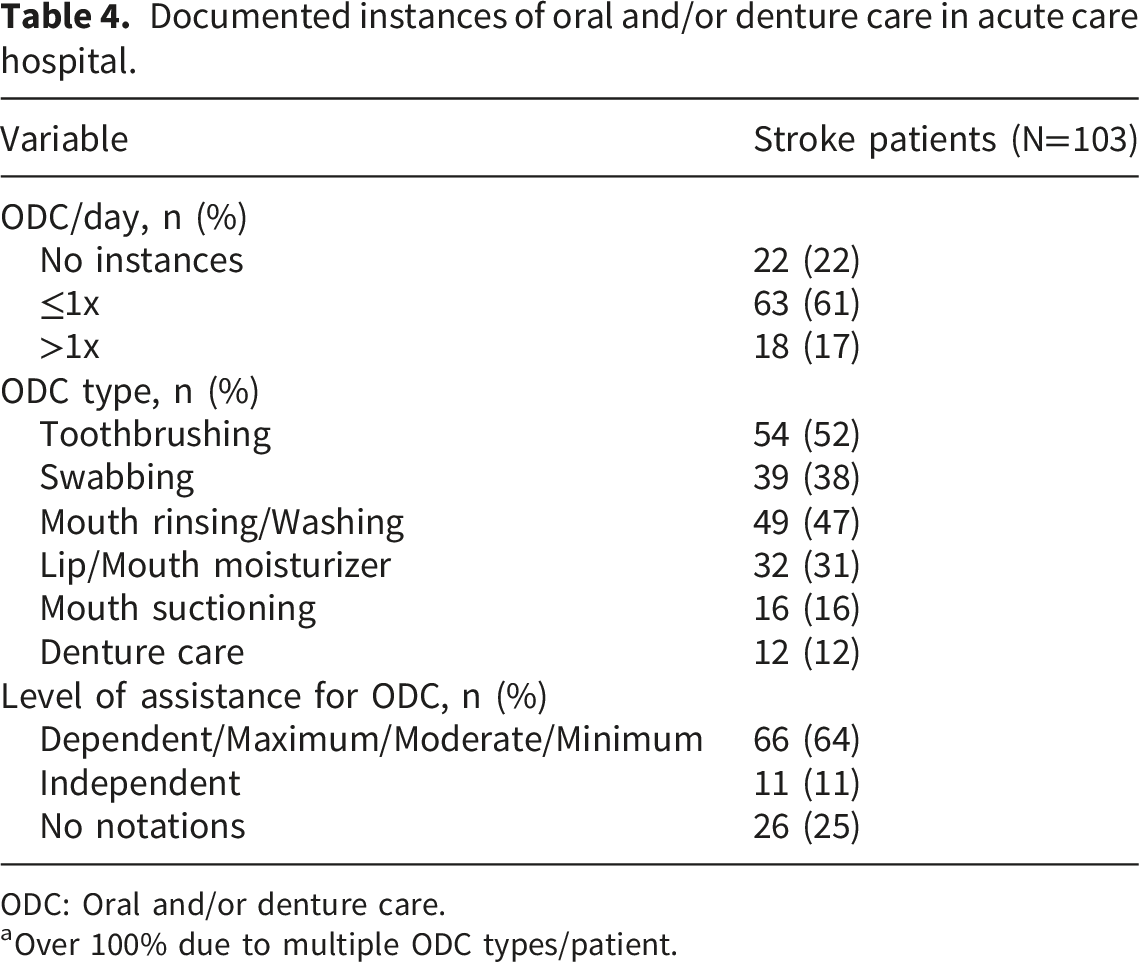
ODC: Oral and/or denture care.
aOver 100% due to multiple ODC types/patient.
Discharge characteristics: Discharge information included return home in 40% and 76% of patients in acute care and rehabilitation, respectively (Supplementary table 6). The Median NIHSS score at discharge was 3 (IQR=4) in acute care and the median FIM score at discharge from rehabilitation was 95 (IQR=38).
Multiple case study
General characteristics of the Cases.
Thematic analysis of MCS yielded five themes, two related to ODC before the stroke event and three related to stroke-induced challenges.
Theme 1: Valued oral health and ODC
The Cases appreciated oral health and acknowledged the importance of daily ODC to keep “healthy teeth and gums”. Oral examinations were consistent with these values in several Cases: for example, Anthony’s oral tissues appeared healthy with no overt active caries, and Bob’s gums and mucosa were compatible with health. Observations included noting that Cases who described strong pre-stroke oral hygiene routines tended to re-establish organized set-ups such as keeping toothbrush and paste in fixed locations and following consistent sequence of steps for oral care.
Theme 2: Independent ODC before stroke
The Cases performed daily ODC independently and four attended regular preventive dental appointments. To illustrate, Anthony said “I brushed once a day I had a toothbrushing and toothpick regimen. Plus, I Had oral care from a provider twice a year”. Oral examination findings aligned with self-reports of pre-stroke routines: some Cases presented with restorations consistent with prior preventive/dental care. Conversely, participants with less frequent regular preventive histories such as Daniel showed greater in-session plaque or debris after meals. Observations showed that despite having been fully independent with ODC before stroke, some Cases like Carol now needed her caregiver to set up her oral hygiene kit.
Theme 3: Inconsistent support for ODC in acute care
During stroke hospitalization, Cases’ ODC routine changed, and they lost self-efficacy for ODC. Daniel’s caregiver said “his hands were not working” and Bob explained he felt disoriented “I didn’t think of anything if somebody didn’t ask me to do oral care, I wouldn’t do it”. Nonetheless, support from HCPs was not regularly received. Frank mentioned, “nurses were so busy they didn’t even know I’ve got teeth”. Anthony’s caregiver declared “he did not brush for a whole week during his 11-day stay”. Emily received some ODC, but her caregiver said that a regular oral care provision schedule was not followed”. Meanwhile, Carol’s caregiver mentioned she had ODC “twice a day while she was tube fed They used a sponge with mouthwash it wasn’t until she started to eat food again that we brushed her teeth”. Two caregivers highlighted that only swabs were available. They all agreed that a kit from home was necessary to facilitate Cases’ ODC.
Theme 4: Increased self-efficacy despite irregular ODC assistance in rehabilitation
In rehabilitation, participants had different experiences. Five cases had their ODC abilities assessed by occupational therapists. Only Bob did not because he usually brushed his teeth after breakfast and the assessment happened before. Nonetheless, he declared “nurses made sure I’ve done oral care”. He and Anthony compensated for the weakness of their dominant hand thanks to rehabilitation therapies. Carol, Emily, and Frank, who were dependent for ODC, did not receive regular care from the nurses. Their caregivers helped, but Emily’s was “too afraid to do it because of the choking risk”. Emily had dysphagia. The observations showed that Daniel brushed his own teeth but had difficulty grasping the thin toothbrush handle and sometimes dropped it on the floor. Also, it was observed that a Case needed assistance for ODC due to the hospital’s inaccessible building infrastructure: it was visibly difficult for him to reach doorknobs and open faucets from a wheelchair. Still, two caregivers said the rehabilitation hospital was “homy”, “not like a hospital”. The participants felt the rehabilitation environment more pleasant and encouraging for Cases to advance their ODC abilities than the acute care hospital.
Theme 5: Ongoing reliance on caregivers or staff for ODC
Besides the observed body movement restrictions, impairments such as fatigue, aphasia, hemispatial neglect, concentration difficulties, dysphagia, and orofacial hemiparesis challenged independent ODC. Emily, for instance, received set up assistance for ODC during one of the observations, but fatigue and poor concentration prevented her from finishing it – a rehabilitation assistant completed the task. The oral examination showed visible plaque and debris in Emily’s mouth. Despite all the difficulties, the MCS participants believed the stroke recovery trajectory was positive and expected further improvements, especially after discharge. Once home, the Cases would feel more comfortable and less overwhelmed but acknowledged continuous need for assistance for ODC, as Frank said, “I’d ask her [caregiver] to clean my teeth [at home]. Otherwise, it’s [going to be] hard for me”.
Key findings for the mixed-methods analysis are in Figure 1. Across data sources, ODC was consistently identified as relevant to post-stroke care, though reported and/or observed practices were variable during hospitalization. HCPs acknowledged the importance of ODC, while case study participants described disrupted routines and reduced independence following stroke. Main quantitative and qualitative results according to the modified Social Cognitive Theory model.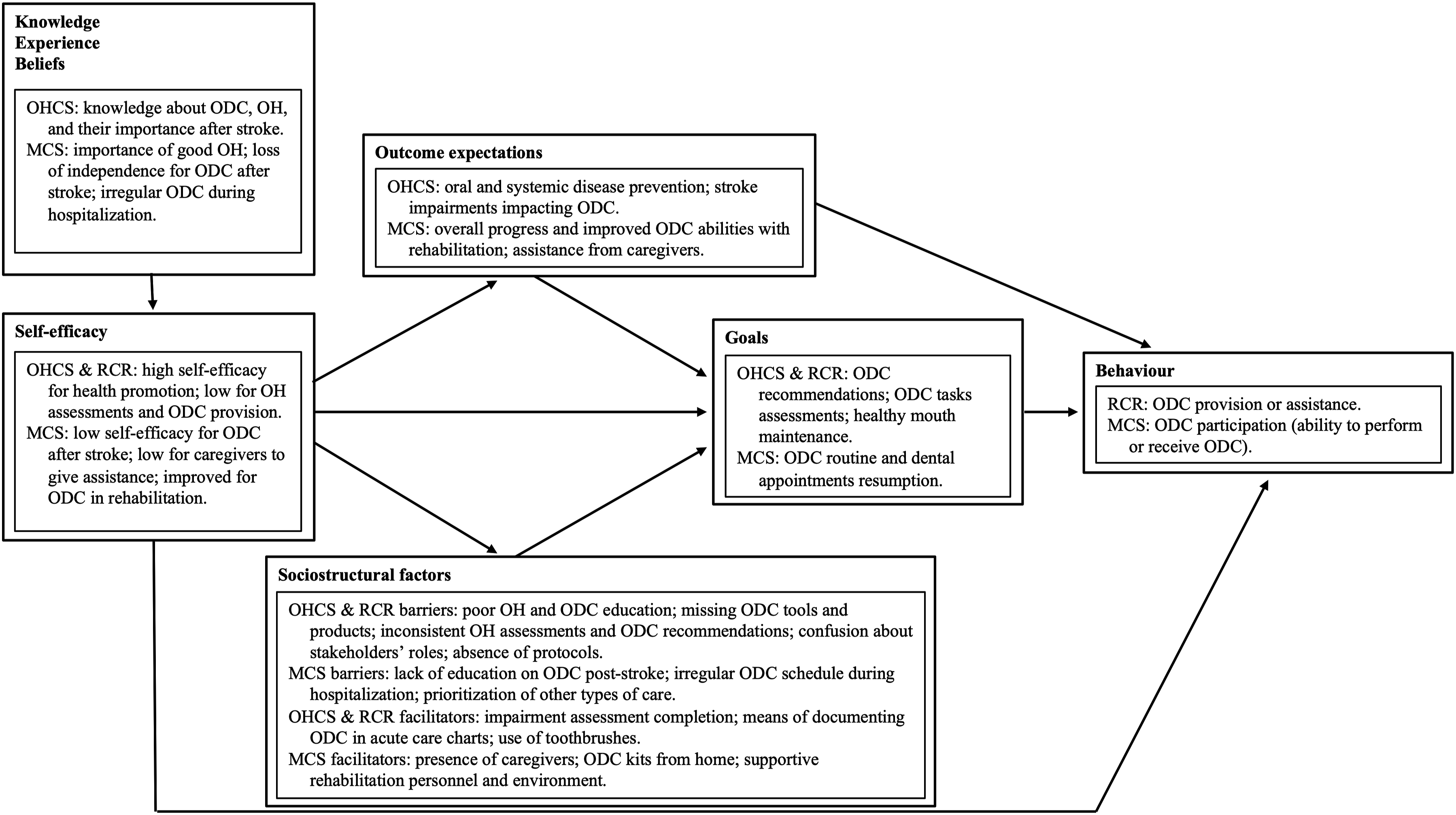
Self-efficacy differed by role and care phase, with HCPs reporting greater confidence in health promotion than in ODC assessment or delivery, and case study participants describing limited ability to perform or receive ODC early after stroke, with some improvement during rehabilitation.
Expected outcomes and goals across sources centred on disease prevention, functional progress, re-establishment of ODC routines, and caregiver involvement.
Sociostructural factors from the surveys, chart review, and case study included inconsistent education and assessment practices, limited availability of tools and protocols, and variable caregiver and environmental supports.
These factors corresponded with documented and reported ODC behaviours, including provision or assistance by healthcare providers and limited participation by patients depending on functional status and available support.
Discussion
This mixed-methods study integrated quantitative and qualitative data to examine post-stroke ODC practices and patient experiences in hospital through the lens of Social Cognitive Theory. Across data sources, Social Cognitive Theory constructs helped explain how individual capacities, environmental conditions, and care behaviours interacted to shape ODC delivery following stroke.
Case study participants valued oral health and described strong pre-stroke ODC, reflecting well-established knowledge and beliefs about ODC as a core self-care activity, consistent with prior research. 59 Both stroke survivors and caregivers expressed optimism about recovery and had goals to improve oral and denture care skills during rehabilitation in order to re-establish pre-stroke behaviours.
Despite these positive beliefs and goals, stroke impairments substantially reduced Cases’ self-efficacy for ODC. Tasks such as reaching the sink, setting up hygiene tools/products, and effectively cleaning mouths/dentures became challenging. The chart review showed that walking difficulties and arm-hand hemiparesis were prevalent post-stroke, with half of patients experiencing dominant-hand paralysis and nearly two-thirds in acute care requiring assistance with ODC. Facial hemiparesis, present in over half of patients, likely further impeded oral containment of hygiene products (e.g., mouthwash, toothpaste). In the case study, performing ODC was laborious and often impossible without assistance, aligning with previous reports. 60 Toothpaste and water spillage during oral care further illustrated the physical challenges faced by patients.
Stroke-related perceptual and cognitive impairments also impacted self-efficacy for independent ODC. Hemispatial neglect, documented in one-third of patients, may explain the presence of food residue in one-quarter of charts, since this condition, can cause poor oral hygiene on the neglected side. 9 Likewise, neurocognitive disorders, identified in one-third of patients, are associated with periodontal disease 61 and reduced capacity for self-care. In the case study, a participant with moderate post-stroke neurocognitive disorder was not able to perform independent ODC and exhibited gum inflammation, and tooth mobility, consistent with periodontal disease.
Consequently, some StS relied on HCPs for ODC. Survey findings showed that HCPs generally had strong knowledge, positive beliefs, and favourable outcome expectations regarding oral health. They believed oral and denture hygiene are part of normal self-care activities, and expected that good hygiene habits prevented infections, consistent with prior literature. 62 However, these cognitive factors did not consistently translate into ODC behaviours.
In acute care, under half of acute care charts noted patients’ oral health status, with most information recorded by speech-language pathologists rather than nurses, suggesting that screening often occurred only when speech-language pathologists were involved in patient care. Inconsistent screening and charting may lead to unmet needs and inadequate care monitoring. 14 In contrast, rehabilitation ODC documenting behaviours differed since both nurses and speech-language pathologists recorded patients’ oral health status in over two-thirds of charts, despite the absence of standardized assessment protocols. All case study charts had speech-language pathologist or nursing notations.
Dysphagia further influenced ODC practices. One-third of the patients in the chart review had dysphagia, and nearly all of these (94%) had oral health chart notations, likely reflecting speech-language pathologist involvement and a more consistent charting behaviour. In contrast, only a small portion of patients without documented dysphagia assessments (12%) had oral health notations. Because speech-language pathologists typically assess only referred patients, 63 individuals may not receive adequate screening or follow-up. 64
Although speech-language pathologists demonstrated relatively consistent behaviours regarding ODC recommendations in the chart review regardless of patients’ oral health or dysphagia status, nursing adherence to ODC varied. Similar rates of care provision were documented independently of speech-language pathologist involvement. Despite survey findings indicating strong HCP knowledge of importance of oral care, ODC task behaviours—documented only in acute care—remained infrequent. The reasons for inconsistencies in oral health screening and ODC remain unclear. Nurses, unlike speech-language pathologists, may have conducted oral screenings without documenting them as previously reported 64 or may have experienced low self-efficacy related, possibly due to inadequate training. Indeed, despite knowing the link between dysphagia, aspiration pneumonia, and poor oral health, half of survey respondents reported no ODC training. Most also identified sociostructural barriers, including limited or no access to continuing education in workplace, which may further reduce self-efficacy and consistency in care provision, as previously reported.63,65
Additional sociostructural barriers likely influenced ODC behaviours. Supply shortages and high work demands have been cited previously 66 and were echoed in this study. Case study participants reported that ODC was feasible only when caregivers provided hygiene kits. HCPs reported sporadic availability of supplies in hospitals. Toothbrushes were scarce, yet oral swabs—intended for mucosal, not dental cleaning 35 —were abundant and readily available, despite presenting choking risks due to behavioural factors or misuse. 67 Although time constraints were not a unanimous sociostructural barrier reported in the survey, the Cases described that nurses relied on healthcare aides. Notably, almost half of HCPs did not recognize the potential role of other care providers’ potential role in providing ODC, consistent with previous findings. 21
Caregiver involvement might have further contributed to inconsistencies in ODC behaviours. In the case study, caregivers may have performed ODC without corresponding documentation, yet often lacked self-efficacy, especially when dysphagia was present. StS themselves frequently lacked the knowledge or experience to guide caregivers. Training healthcare aides 54 and providing targeted education for patients and caregivers 68 may improve confidence, safety, and consistency, particularly for those at higher risk of aspiration.
The integrated interpretation of these findings was guided by Social Cognitive Theory, which provided a coherent analytical framework across both quantitative and qualitative components of the study. Quantitative results reflected key Social Cognitive Theory constructs, including self-efficacy, outcome expectations, and sociostructural factors, while the qualitative cases enriched these constructs by illustrating how stroke survivors and healthcare providers experienced barriers, facilitators, and motivations in real clinical contexts. For example, post-stroke physical, perceptual, and cognitive impairments reduced survivors’ confidence in performing ODC, while limited training, inconsistent documentation practices, and resource constraints appeared to undermine healthcare providers’ self-efficacy and consistency in care delivery. Integrating the two strands through an SCT lens allowed us to interpret observed practice patterns—such as variable screening, infrequent documentation, and reliance on informal caregiver support—as the result of interacting personal, behavioural, and environmental influences shaping oral and denture care behaviours after stroke.
Collectively, uncertainties in oral health knowledge, ODC behaviours, and sociostructural factors —including unclear stakeholder roles—have important implications for patient safety, continuity of care, and clinical monitoring. Inconsistent documentation and irregular ODC practices limit the ability to track oral health changes, identify emerging risks, and ensure completion of recommended care. This gap is particularly concerning given that HCPs in our survey acknowledged the link between poor oral hygiene and aspiration pneumonia, yet behaviours did not consistently reflect this awareness. Without reliable screening, documentation, and follow-through, patients with dysphagia, reduced alertness, or impaired oral clearance may be exposed to preventable risks such as aspiration of residual food, bacterial load, or oral debris.
These findings underscore the need for clear, evidence-based ODC protocols. We recommend that both acute and rehabilitation settings develop standardized protocols to improve consistency, enhance patient safety, support continuity across providers, and facilitate monitoring throughout hospitalization. Protocols should be tailored to patient needs, while considering local factors such as resource availability and referral pathways. The use of a standardized oral health screening tool with follow-up actions—such as the Comprehensive Oral Assessment Tool for Stroke (COATS) 32 or the Canadian Oral Health Screening Tool for Seniors 69 —alongside adequate education on its application, would support uniform, evidence-based care. Clearly defined roles and ongoing education for HCPs, caregivers, and patients are also essential for effective implementation and sustainability.
While dentists are not currently integrated into routine inpatient stroke care, their involvement will be essential in the development of future evidence-informed ODC protocols. Our findings provide foundational information to support interdisciplinary efforts in which dental professionals collaborate with healthcare providers who deliver ODC at the bedside, contributing expertise in assessment, prevention, and protocol design.
Additional recommendations include toothbrushing at least twice a day in rehabilitation settings. This routine reduces dental plaque and gingival bleeding in StS 70 aligns with i) Canadian guidelines,71,72 ii) our survey reported beliefs, iii) the pre-hospital experiences of most case study participants, and may be feasible for nurses 14 and caregivers. 73 In acute care, we support oral and denture care after meals and before bedtime for StS with dysphagia and those not eating by mouth, as recommended by Canadian guidelines, 31 to reduce choking risk and help prevent aspiration pneumonia.
This study has several limitations with implications for both interpretation and transferability. First, because the middle option on the Likert scale was rarely selected, responses were binarized, which may have reduced the nuance of participants’ views. Second, although healthcare providers from both acute care and rehabilitation settings were invited to participate, only 32 survey responses were obtained, limiting statistical power. Third, the case study component included only individuals in rehabilitation, as conducting interviews with stroke survivors in acute care is often challenging due to the severity of physical and cognitive impairments and, at the time of data collection, pandemic-related restrictions. As a result, acute care experiences were captured through survivors’ and caregivers’ retrospective accounts rather than direct observation or interviews. Fourth, ODC frequency data were available only in acute care charts, representing a structural missing data issue that limited direct comparisons of ODC practices across care settings and constrained interpretation of setting-specific differences. Additionally, the voluntary nature of survey participation may limit the representativeness and transferability of findings. Researcher involvement in data extraction, coding, and analysis may have introduced interpretive bias, although standardized procedures and a researcher reflexive diary were used to mitigate this risk. Finally, given the descriptive and observational design, findings cannot support causal inferences or establish links between screening practices and patient outcomes.
Conclusion
Overall, this mixed-methods study demonstrates that post-stroke ODC behaviours are shaped by the interaction among stroke-related impairments and healthcare providers’ and stroke survivors’ knowledge, beliefs, self-efficacy, expectations, goals, and sociostructural conditions, as conceptualized by Social Cognitive Theory. Although providers recognize the importance of oral health and its role in preventing complications, care delivery and documentation remain inconsistent in the absence of standardized protocols, training, and clear role delineation. These findings support interdisciplinary efforts to design and evaluate evidence-informed ODC protocols to improve patient safety and continuity of care.
Supplemental material
Supplemental material - Oral health after stroke: A mixed-methods study involving healthcare professionals, stroke survivors and primary caregivers
Supplemental material for Oral health after stroke: A mixed-methods study involving healthcare professionals, stroke survivors and primary caregivers by Nalia Gurgel-Juarez, Hillel Finestone, Katrine Sauvé-Schenk, Michael Wiseman, Dylan Blacquiere, Ramin Banimahdi, Anne Carey and Heather L. Flowers in SAGE Open Medicine
Footnotes
Acknowledgments
We thank the collaboration of patients, caregivers, healthcare professionals, hospital staff, and students.
Ethical considerations
Ethical approval was received from the Ottawa Health Science Network (#20200771-01H), Bruyère Health (#M16-20-028) and the University of Ottawa (#H02-21-5972).
Consent to participate
All participants provided written informed consent in accordance with the regulations of the three research ethics boards.
Author contributions
Nalia Gurgel-Juarez and Heather Flowers contributed to the conception of the study; acquisition, analysis, and interpretation of data. Hillel Finestone, Katrine Sauvé-Schenk, and Anne Carey contributed to acquisition, analysis, and interpretation of data. Michael Wiseman contributed to analysis and interpretation of data. Dylan Blacquiere contributed to acquisition and interpretation of data. Ramin Banimahdi contributed to acquisition and analysis of data. All authors contributed to the study design, participated in the drafting and critical revision of the manuscript, approved the final version, and agree to be accountable for all aspects of the work, ensuring the accuracy and integrity of the research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Network for Canadian Oral Health Research and the University of Ottawa, Faculty of Health Sciences. The first author received funding from the Ontario Graduate Scholarship, the University of Ottawa Excellence Scholarship, and the Life Research Institute.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.