
Abstract
Introduction:
Diarrhea is one of the public health important diseases in developing countries. Among the causative agents of diarrhea, Salmonella serovars and Shigella species continue to play a major role in resource-limited countries. The aim of this study was to assess the prevalence of Salmonella and Shigella, risk factors, and antimicrobial susceptibility profiles among adult patients with complaints of diarrhea.
Methods:
A hospital-based cross-sectional study was conducted among adult patients with complaints of diarrhea at Hawassa University Comprehensive Specialized Hospital from March 2019 to November 2019. A structured questionnaire was used to collect sociodemographic, behavioral, and environmental characteristics of participants. Fecal samples were inoculated onto Selenite F broth and Xylose Lysine Dextrose media to isolate Salmonella serovars and Shigella species. Antibiotic susceptibility testing was performed by the Kirby-Bauer method. Data were analyzed by SPSS computer software version 20. Bivariate and multivariable analysis was used to determine the association between dependent and independent variables.
Results:
The overall prevalence of Salmonella serovars and Shigella species was 8.6% with 95% confidence interval (3.2–13.8). Participant those who do not wash their hands were three times more likely to be infected with Salmonella and Shigella (p < 0.001) than their counterparts. Participants who consume uncooked food had about two times the chance to be infected with Salmonella and Shigella (p < 0.001) than their counterparts. All serovars of Salmonella and serotypes of Shigella were resistant to ampicillin.
Conclusion:
In this study, relatively a high prevalence of Salmonella serovars and Shigella species was found among adult patients with complaints of diarrhea at Hawassa University Comprehensive Specialized Hospital. Consuming uncooked food and not washing hands were significantly associated with the prevalence of Salmonella and Shigella.
Introduction
Diarrhea is caused by a wide variety of bacteria, viruses, and parasites. 1 Among the diarrheal pathogens, Salmonella serovars and Shigella species continue to play a major role as the etiology of diarrhea and dysentery, thus presenting a serious challenge to public health authorities worldwide. 2
Globally, 780 million individuals lack access to improved drinking water and 2.5 billion lack improved sanitation. 3 Diarrhea caused by infection is highly prevalent in developing countries. Globally, there are nearly 1.7 billion cases of diarrheal disease every year. 3
In Africa, about 115 people die as a result of diarrheal diseases every hour, mostly because of Shigellosis and Salmonellosis which are linked to contaminated food and water due to poor sanitation and hygiene. 4 People living in developing countries, where there is limited access to safe water or lack of infrastructures required for sanitation, have increased risk to develop diarrheal disease due to viral, bacterial, and parasitic pathogens. 5
Salmonella serovars are the main cause of food-related diseases that results in enterocolitis, enteric fever, and sepsis. Disease caused by Salmonella lasts for a few days and it is usually self-limited; however, it may progress to a more serious infection.6,7 Shigella species are solely confined to the gastrointestinal tract and are responsible for dysentery. Humans acquire Shigella via ingestion of contaminated water and food. 8 The prevalence of Shigella is high in resource-limited countries where there is no access to clean water and food and proper disposal system. 8
In developing countries like Ethiopia, the uncontrolled prescription of antibiotics has led to the emergence of antibiotic-resistant bacteria. 9 Resistance may be acquired mostly by selective pressure due to indiscriminate and misuse of antibiotics. 10 This made antibiotic selection difficult for the treatment of disease caused by Salmonella serovars and Shigella species.11–13 Several studies have reported antibiotic-resistant Salmonella and Shigella from different parts of Ethiopia.13–16 Diarrhea is still prevalent in different parts of Ethiopia especially those caused by Salmonella serovars and Shigella species account for the highest proportion. The aim of this study was to determine the prevalence of Salmonella serovars and Shigella species, serotype distribution, risk factors, and antimicrobial susceptibility profile among adult patients with complaints of diarrhea.
Materials and methods
Study area
This study was conducted at Hawassa University Comprehensive Specialized Hospital (HUCSH) which is located in Hawassa city. Hawassa is located 275 km from the capital city of Ethiopia, Addis Ababa. The city is located at 7′ 30″ latitude North and 37′ 30″ East longitude. HUCSH is a tertiary health care hospital serving the population of South Nations Nationalities Peoples Regions (SNNPR) and the neighboring Oromia region.
Study design and period
A hospital-based cross-sectional study was conducted from March 2019 to December 2019.
Eligibility criteria
All volunteer adult patients with complaints of diarrhea and those aged ⩾18 years were considered for this study. Patients who took antibiotics in the last 2 weeks prior to data collection and those who were critically ill and unable to be interviewed were excluded from the study.
Operational definition
Diarrhea: Passing three or more loose or liquid stools over a 24-h period.
Sample size
The sample size was determined (N = 278) using a single population proportion formula. A prevalence reported from Jimma University Specialized Hospital (11.9%), 17 a 95% confidence interval (CI), 4% margin of error, and 10% non-response rate was considered in the calculation of the sample size. The participants were recruited using a systematic random sampling technique. According to data obtained from the hospital, 1039 adult patients with complaints of diarrhea were expected to visit the hospital during the study period. The interval (K = 4) was obtained by dividing the patient flow by the sample size. Accordingly, every fourth adult patient with complaints of diarrhea was recruited. The first participant was selected by a lottery method.
Data collection
Study variables
Dependent variables: Culture results of stool.
Independent variables: Sociodemographic factors, environmental factors, and behavioral factors.
Sociodemographic data
A structured questionnaire which was adapted with modification from a study conducted in the Afar region, Ethiopia, 18 was used to collect sociodemographic, behavioral, and environmental.
Laboratory data
Two grams of semi-formed stool or 2 mL watery stool sample was collected from the study participants using a coded disposable plastic cup. First stool samples were inoculated onto selenite F (Oxoid, Hampshire, UK) broth and incubated at 37°C. Then subcultured onto Xylose Lysine Deoxycholate (XLD; Oxoid) agar and incubated at 35°C–37°C for 18–24 h. After 24 h of incubation, the culture media was evaluated for the presence of bacterial growth. The identity of bacteria was confirmed using a panel of biochemical tests recommended for enteric bacteria. 10 Typical colonies were then further characterized based on colony morphology (Salmonella appears as pink-red colonies with a black center, while Shigella appears as pink-red colonies on XLD). For identification of Salmonella serovars and Shigella species, all suspected colonies were inoculated onto appropriate biochemical media (Oxoid) including Kligler iron agar, Lysine iron agar, Simmon’s citrate agar, sulfide indole motility medium, and urea. For identification of Salmonella serovars, Wellcolex Color Salmonella (Remel Inc., Lenexa, KS, USA) was used. Shigella species was confirmed by slide agglutination using commercially available, absorbed rabbit antisera (Biotec Laboratories, Radstock, UK).
Antibiotic susceptibility testing
Antibiotic susceptibility testing was conducted using Kirby-Bauer disk diffusion methods according to the Clinical and Laboratory Standards Institute (CLSI) guideline. 19
Data quality control
The questionnaire was prepared in English and translated into Amharic, and finally, the Amharic version was translated back to English by a different person to ensure the consistency of the questionnaire. The questionnaire was pre-tested on a 5% sample size at Adare General Hospital for the validation of the questionnaire. To check the sterility of the culture media, 5% of the media were incubated without inoculation. The performance of media was checked using reference strains.
Data analysis
Data entry and analysis were carried out using SPSS version 20 software. Data were summarized using text and tables. Logistic regression was used to determine predictors of the prevalence of Salmonella serovars and Shigella species. Factors with a p value of less than 0.25 in bivariate analysis were further analyzed by multivariable logistic regressions. A p value of less than 0.05 was taken as a cut point to determine a statistically significant association.
Results
Sociodemographic profile
A total of 278 adult patients with complaints of diarrhea have participated in this study with a response rate of 100%. Most of the participants were within the age group of 18–24 years. Of the total participants, males accounted for 54.3%. The majority of participants were urban dwellers (80.9.0%). Most of the participants (57.9%) were government employees (Table 1).
Sociodemographic profile of adult patients with complaint of diarrhea at HUCSH, South Ethiopia, 2020 (N = 278).

HUCSH: Hawassa University Comprehensive specialized hospital.
Prevalence and associated factors
The overall prevalence of Salmonella serovars and Shigella species was 8.6% with 95% CI: (3.2–13.8). The proportion of Salmonella serovars and Shigella species was 15 (5.4%) and 9 (3.2%), respectively. The proportion of Salmonella Typhi, Salmonella Paratyphi, Shigella dysenteriae, and Shigella flexneri were 11 (4%), 4 (1.4%), 6 (66.7%), and 3 (1.1%), respectively (Table 2).
Proportion of bacteria isolated from adult patients with complaint of diarrhea at HUCSH, South Ethiopia, 2020 (N = 24).
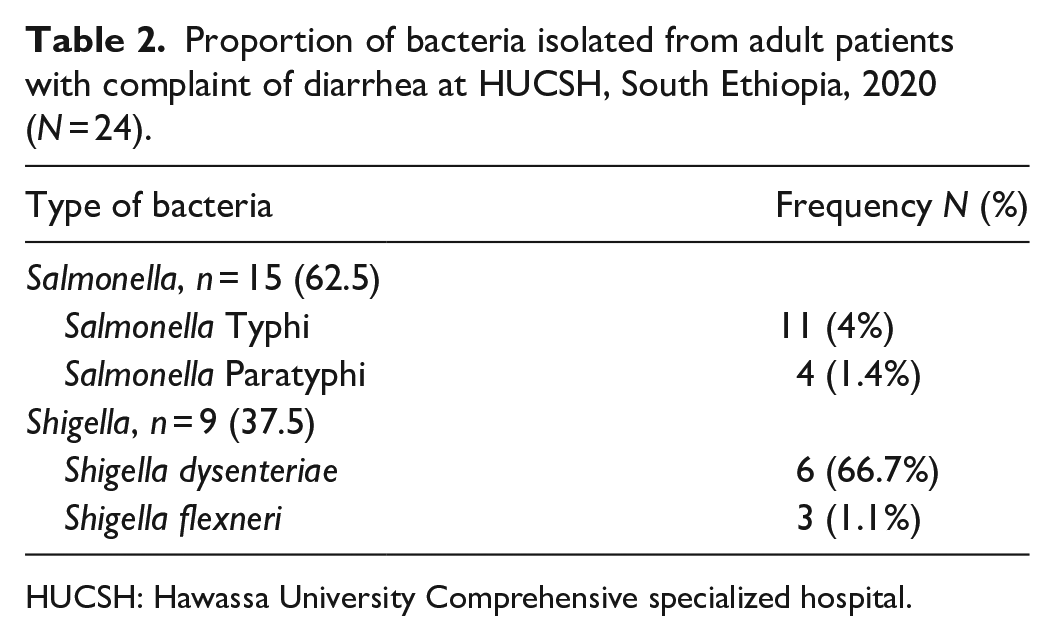
HUCSH: Hawassa University Comprehensive specialized hospital.
Participant those who do not wash their hands were about three times more likely to be infected with Salmonella serovars and Shigella species (p < 0.001). Participants who consume uncooked food were about two times more likely to be infected with Salmonella and Shigella (p < 0.001) (Table 3).
Factors associated with prevalence of Salmonella serovars and Shigella species among adult patients at HUCSH, 2020 (N = 278).

HUCSH: Hawassa University Comprehensive specialized hospital; COR: crude odd ratio; AOR: adjusted odd ratio; CI: confidence interval.
Antimicrobial susceptibility profile
All serovars of Salmonella and species of Shigella were resistant to ampicillin. All of them were susceptible to meropenem. The majority of S. Typhi (62.5%) were resistant to chloramphenicol (Table 4).
Antimicrobial susceptibility pattern of Salmonella serovars and Shigella species isolated from adult patients with diarrhea at HUCSH, South Ethiopia, 2020 (N = 24).

HUCSH: Hawassa University Comprehensive and Specialized Hospital; n: number; AMP: ampicillin; AUG: augmentin; CTZ: ceftazidime; CTR: ceftriaxone; CHL: chloramphenicol; CIP: ciprofloxacin; GEN: gentamycin; MER: meropenem.
Discussion
The prevalence of Salmonella serovars among adult patients with complaints of diarrhea found in this study (5.4%) is higher than the study conducted in Gondar (1.08%), 20 Tigray (1.6%), 21 and Djibouti (2.9%). 22 In contrast, the finding of this study is low compared to reports from Harar, Ethiopia (11.5%); 23 Dilla, Ethiopia (9.5%); 24 and Libya (17.5%). 25 The finding of this study is in agreement with a study conducted in Hawassa (5.1%). 26 This could be explained by variation in sociodemographic factors, sample size, season, the diagnostic method used, and the study setting. The prevalence of Shigella species (3.2%) detected in this study is higher than the prevalence of Shigella reported from Hawassa, Ethiopia (1.3%);23,27 however, it is lower than the prevalence reported from Nigeria (6.1%); 28 Harare, Ethiopia (6.7%); 23 Afar, Ethiopia (7.4%); 18 Djibouti (7.7%); 22 and Kenya (16%). 29 Similar finding was reported from Dilla Ethiopia (3.2%). 24 This variation could be explained by the same reason explained for variation in the prevalence of Shigella serovars. The prevalence of Shigella in this study was in line with the prevalence reported from Arba Minch, Ethiopia (3%). 30
The proportion of S. dysenteriae (2.2%) found in this study is higher than the proportion reported from Gondar, Ethiopia (1%); 20 Nigeria (1.1%); 28 and Djibouti (1%). 22 In contrast, the finding is lower than the reports from Adama, Ethiopia (23.8%) 31 and Kenya (4.5%). 29 On the other hand, the proportion of S. flexneri (1.1%) is lower than reports from Gondar, Ethiopia (3%); 20 Nigeria (3.13%); 28 Djibouti (5.7%); 22 and Kenya (9%). 29 In this study, S. Typhi accounts for 4%, which is higher than the prevalence of S. Typhi reported from Kenya (<1%) 29 and Djibouti (<1%). 22 Unlike this study, higher proportion of S. Typhi was reported from Mekelle, Ethiopia (21.3%) 21 and Adama, Ethiopia (21.4%). 31 The possible explanation for the variation might be due to sociodemographic factors, sample size, the difference in the study population, the method of diagnosis, and the study setting.
In this study, adult patients who do not wash their hands were three times more likely to be infected by Salmonella serovars and Shigella species (p = 0.002). This finding is in line with studies conducted in Arba Minch, Ethiopia 30 and Afar, Ethiopia. 18 Adults who consume raw or uncooked food were two times more likely to be infected with Salmonella serovars and Shigella species (p = 0.001). This finding was comparable with a report from Hawassa, Ethiopia. 27 Factors such as access to latrine and having domestic animals in their homes were not significantly associated with the prevalence of Salmonella and Shigella (p > 0.05).
In contrast to this study, a significant association between access to a latrine and possessing animals with the prevalence of Salmonella and Shigella was reported from Afar, Ethiopia 18 and Djibouti, 22 respectively. This variation could be due to differences in sociodemographic factors and improved awareness of the community about personal and environmental hygiene. In this study, a high proportion (27.3%) of adult patients with complaints of diarrhea who drink other sources of water (spring, well, and rain) were infected with Salmonella and Shigella even though it was not statistically significant (p > 0.05).
All Salmonella isolated in this study were resistant to ampicillin. This finding was comparable with studies conducted in different parts of Ethiopia.17,20,24 In line with studies conducted in Hawassa 26 and sub-Saharan African countries, 32 73.3% of Salmonella spices isolated in this study were resistant to chloramphenicol. The prevalence of ampicillin (25%) and chloramphenicol (22.5%) resistant Salmonella reported from Libya was low compared to our study. 25 Unlike this study, the majority of Salmonella isolated from Kenya (65%) 28 and Djibouti (56%) 22 were resistant to amoxicillin-clavulanate and gentamicin, respectively.
All Shigella species isolated in this study were resistant to ampicillin. This finding was comparable with studies conducted in different parts of Ethiopia.17,20 Similar to our study, all and 66.7% of Shigella from Djibouti 22 and Nigeria 28 were resistant to ampicillin and chloramphenicol, respectively. The prevalence of ampicillin-resistant Shigella reported from Kenya (44%) 27 was low compared to our study. In contrast to this study, the majority of Shigella isolated from Kenya (65%) 29 and Djibouti (100%) 22 were resistant to amoxicillin-clavulanate and gentamicin, respectively.
Conclusion
The overall prevalence of Salmonella serovars and Shigella species was 8.6%. The proportion of Salmonella serovars and Shigella species was 15 (5.4%) and 9 (3.2%), respectively. S. Typhi, S. Paratyphi, S. dysenteriae, and S. flexneri accounted for 11 (4.0%), 4 (1.4%), 6 (2.1%), and 3 (1.1%), respectively. Participants who do not wash their hands were about three times more likely to be infected with Salmonella serovars and Shigella species. Participants who have a habit of consuming uncooked food were about two times more likely to be infected with Salmonella and Shigella. All Salmonella serovars and serotypes of Shigella serotypes were resistant to ampicillin.
Limitations of the study
As the study was cross-sectional, it does not establish a temporal relationship between cause and effect. Since this is a single-site study, which is hospital-based, it is difficult to generalize the finding of this study to all adult populations with complaints of diarrhea in Hawassa city.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211000911 – Supplemental material for Salmonella and Shigella and antimicrobial susceptibility profiles among adult patients with complaints of diarrhea at Hawassa comprehensive specialized hospital, Hawassa, Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121211000911 for Salmonella and Shigella and antimicrobial susceptibility profiles among adult patients with complaints of diarrhea at Hawassa comprehensive specialized hospital, Hawassa, Ethiopia by Kassahun Abera, Tariku Lambiyo Anticho and Musa Mohammed Ali in SAGE Open Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from * Institutional Review Board (IRB) Hawassa University College of Medicine and Health Sciences (IRB/161/10).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.