
Abstract
Introduction:
An occupational injury is a global health issue, and in hotel industries, little is known about it. The aim of this study was therefore to assess the epidemiology of occupational injuries in international brand hotels.
Method:
An institutional cross-sectional study was conducted among 330 workers using a systematic random sampling method. Using EpiData and SPSS, respectively, data were entered and analyzed. The final results were explained and presented with the adjusted odds ratio and the 95% confidence interval, and the results of the qualitative data were triangulated with quantitative data.
Results:
Of the 330 study participants, 125 (37.9%; 95% confidence interval (32.7%, 43.8%)) reported having sustained an occupational injury. The study showed those who had four or less family members (adjusted odds ratio: 0.484, 95% confidence interval (0.286, 0.818)), those who had low educational background (adjusted odds ratio: 1.466, 95% confidence interval (1.098, 1.959)), those who had 2 years or less work experience (adjusted odds ratio: 1.065, 95% confidence interval (1.023, 1.108)), those who were working in shifts (adjusted odds ratio: 2.559, 95% confidence interval (1.197, 5.474)), and those who had sleep disturbance (adjusted odds ratio: 1.797, 95% confidence interval (1.025, 3.151)) were factors significantly associated with occupational injury.
Conclusion:
The study found that the prevalence rate was very high. Among the variables included in the analysis, having four or less family sizes, low educational background, having work experience of 2 years or less, working in shifts, and having sleep disorders/problems were statistically significant. It is therefore recommended that health and safety training and reinforcement be provided to increase awareness and understand the risk factors at the workplace.
Introduction
An occupational injury is an unexpected and unplanned occurrence that results in injury, illness, death, or economic devastation to families, business, and communities.1–4 Hotels are generally organized into different departments providing guests with specialized services. 5 There are potentially hundreds of ways in which employees can harm themselves; majors are commonly referred to as forceful exercises, awkward postures, repetitive movements, the handling of various tools and equipment, a fast-paced work environment, and little rest. 6 Evidence showed that the direct cost of a workplace injury can amount to 14%–16% of payroll expense and indirect costs of a workplace injury can amount to 42%–48% of payroll expenses. 7 A study done on hotel housekeepers in the US hotel industry shows that 52% of injuries were classified as acute trauma followed by 39% considered to be musculoskeletal disorders with upper extremity the most common body region of injury. 8
Evidence has shown that the magnitude of this injury is common among different industrial workers. It is preventable and modifiable by addressing factors such as the use of personal protective equipment (PPE), the rotation of jobs, the provision of health and safety training, overtime work, lack of vocational training, and dissatisfaction with work.9–12 The 2019 Ethiopian National Hotel Grading Report shows that 83 hotels were ranked between one and four stars. The grading was carried out by native experts, and the scheme was designed following international hotel grading standards. 13
The hotel industry operates with a large number of human resources worldwide and the job description of hotel workers varies depending on their position, but many of them are tasked with a job of cleaning, maintaining, and caring for the property. 14 Ethiopian hospitality industry workers have been identified as under-researched and under-served workers facing uneven distribution of health outcomes compared to other industrial workers in the country. 15 The aim of this study was therefore to assess the epidemiology of occupational injuries and associated factors among hotel workers in Addis Ababa.
Methods
Study design and study period
An institution-based cross-sectional study both descriptive and analytical methods were conducted from 1 to 15 May 2019, among employees of the brand hotels in Kirkos sub-city, Addis Ababa, a capital city of Ethiopia. The time frame has included injuries that have occurred in the last 12 months before data collection time. The sub-city has 11 woredas, which constitute kebele, the smallest administrative level in the city. According to the recent data from the Kirkos sub-city head office, the current population is estimated to be 235,441. The sub-city, with an estimated population of 235,441, is one of the densely populated sub-cities. Addis Ababa city has six international brand hotels in which this sub-city consists of four of the brand hotels, that possessed about 1860 workers, from oldest to newest brands: Hilton Addis Ababa Hotel, Sheraton Addis Hotel, Radisson Blu Hotel, and Marriott Executive Apartment Hotel. The remaining two brand hotels are the Ramada Addis and the Golden Tulip Hotel which are located in the Bole sub-city. The hotels comprise several main departments performing various functions like housekeeping, food and beverage service, stewarding, laundry, engineering and guest services (front offices), finance, human resources, and security department.
Population and sampling
International hotels seem safe most of the time in Ethiopia, even though the magnitude of the injury is high and under-reported in these hotels. All brand hotel employees working in the brand hotels located in the Kirkos sub-city of Addis Ababa were the source population while selected employees of the brand hotels who met the eligibility criteria during the study period were the study population for the quantitative study. The inclusion criterion was being employees of the brand hotels who completed their probation period while those employees who were newly hired (on probation period) were excluded from the study. For qualitative data, key informants of brand hotels, administrative bodies such as human resources officers, safety officers, supervisors, staff clinic physicians, and nurses were included in the study. For quantitative data, the sample size was calculated using the single population proportion formula based on the following assumptions: prevalence of occupational injuries from previous study 38.4%, 16 the margin of error 5%, and 95% confidence level. With an additional 10% non-response rate, the sample size was found to be 334 which was proportionally allocated to each hotel. Samples were chosen using a systematic random sampling technique and the first case was selected using a lottery method. The total number of employees of each hotel was divided by the number of allocated sample sizes. Then, k-value was calculated for each, and they were selected using the employee’s identification number. There were 350 employees in Radisson Blu Hotel, 715 in Sheraton Hotel, 150 Marriott Hotel, and 635 in Hilton Hotel. Accordingly, 114, 128, 64, and 26 samples were selected from Hilton Hotel, Sheraton Hotel, Radisson Blu Hotel, and Marriott Hotel, respectively. For the qualitative study, six purposefully selected key informants, the department supervisor’s manager, and security directors have participated in the study.
Data collection tool and procedure
Data were collected using a pre-tested and structured questionnaire that was prepared originally in English and translated into Amharic and back-translated into English to ensure its consistency. The questionnaire was adapted and developed after reviewing different literature.8,12,15–18 The questioners were grouped into four sections: sociodemographic variables, work-related variables such as health and safety training, characteristics of injury such as the source of injury, and behavioral factors such as drinking and chewing habits. For the qualitative study, checklists for work environment observations and the key informant interview guide were used. Information depth was determined by reaching the point of saturation. A face-to-face interview was used to obtain some descriptive information from the key informants. Quantitative data were collected by two trained nurses who had experience and a better understanding of data collection while qualitative data were collected by a master’s holder public health expert. The qualitative data collection was done using an audio recorder at the key informants’ office during working hours in the absence of anyone. To ensure the quality of data, 2-day training was given for data collectors mainly on the purpose of the study, the quality of data, and the data collection techniques to be followed. Besides, the questionnaire was also pre-tested. Supervision and data quality checking were done during and after data collection time.
Statistical analysis
After data collection, each questionnaire was checked for accuracy, uniformity of questionnaires, logical completeness, and consistency. Then, it was entered and analyzed using EpiData Version 3.1 and SPSS Version 23.0, respectively. After data exploration, descriptive statistics such as frequency distribution, mean, and percentage calculation were done for most of the variables. Those variables that fulfilled the chi-square assumption were included in logistic regression (bivariate and multivariate logistic regression) analyses to identify factors affecting occupational injuries. To measure the degree of association between the dependent and explanatory variables, the odds ratio was calculated. Those variables with a p-value < 0.25 on bivariate analyses were a candidate for multivariate analysis and those variables with a p-value of less than 0.05 were considered as statistically significant. Multicollinearity assessment was conducted using the means of variation inflation factors (VIFs) on the linear regression method (VIF = 1.00) which indicated that there was no significant collinearity between explanatory variables in the logistic regression model. The goodness-of-fit test (Omnibus Tests of Model Coefficients) of the final model was checked and it was significant (p-value < 0.05) and the Hosmer and Lemeshow goodness-of-fit test was not significant (p-value = 0.317) as indicators of model appropriateness. The final results were explained and presented with the adjusted odds ratio (AOR) and the 95% confidence interval (CI). The qualitative data recorded from the in-depth interview were transcribed verbatim and translated from the local language into the English language. The transcribed data were read carefully, categorized, and summarized in thematic areas, and then triangulated with the quantitative data.
Results
Sociodemographic characteristics
Out of the total 334 sampled employees, 330 were interviewed and included in the analysis with a response rate of 98.8%. The mean (±standard deviation (SD)) age of respondents was 36.1 ± 6.94 years. Most of the respondents (70.3%) had a diploma and above with their educational status. Nine-tenths of the respondents were earning a monthly income of up to 10,000 Ethiopian birr. More than half of the study participants (58.3%) were married and more than two-thirds, 69.1%, had four family members. Most of the respondents (68.2%) were orthodox Christian by their religion (Table 1). For the qualitative study, participants had diplomas and degree holders, and they had different work experiences in different organizations. They had a duration of more than 3 years of service in their current position during the study.
Frequency of major variables among employees of the brand hotels found in Kirkos sub-city, Addis Ababa, 2019.
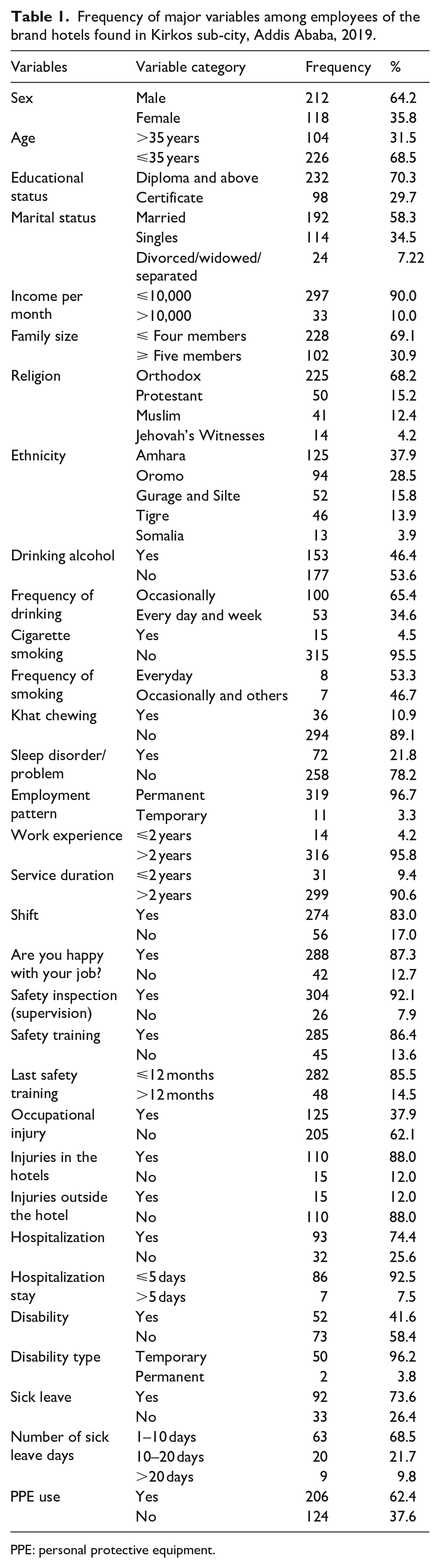
PPE: personal protective equipment.
Workers’ behavioral characteristics
The study showed that 153 (46.4%), 15 (4.5%), 36 (10.9%), and 72 (21.8%) of participants had habits of drinking alcohol, smoking cigarette, khat chewing, and sleeping problems, respectively. About two-thirds (65.4%) of workers had drunk alcohol occasionally, while 44.4% had chewed khat once per week. About 29.2% of the respondents indicated that they had sleeping difficulties due to personal issues, work burden, and working in shift and long hours which accounted for 23.6% and 47.2%, respectively, (Table 1).
In support of the quantitative study, one human resources coordinator stated that,
Most of the workers explained to be happy with their job. Most of them are engaged in different activities in different places. Some workers have habits of smoking, khat chewing, and drinking alcohol. Last time, one employee had an accident while working in a kitchen; he had sleep deprivation due to being engaged in different duties. He had an accident on his head due to loss or lack of consciousness at work. (Age 43 years, human resources coordinator)
Characteristics of the working environment
The respondents’ work experience varies from 1 to 29 years with a mean work experience of 10 years and they have stayed an average of 7 years’ service duration on their current work positions. Among the respondents, 288 (87.3%) employees mentioned that they were happy with their job. More than nine-tenths of the respondents 92.1% said that there was a workplace inspection (supervision) and the majority of the respondents, 85.5%, had taken safety training within the last 12 months (Table 1).
In support of this finding, the security officer stated,
The nature of hotel work exposes employees to different kinds of health and safety hazards. Thus, most workers prefer to use protective devices in their preferences rather than those provided for them; in particular, they use their shoes instead of using the safety shoes provided for them by the companies. Since there is no safety personnel, training is given online and safety supervision is done by the outlet supervisors. They (Hotel) are working to hire a safety officer as fast as possible. But, the Safety issues are currently being handled by the security department in terms of property safety, loss prevention, and injury recording and reporting. (Male security director)
Occupational injury characteristics
This study showed that the prevalence of occupational injury in the last 12 months was 37.9% (95% CI (32.7%, 43.8%)) in which the back 33 (26.4%), hand-finger 25 (20.0%), leg 16 (12.8%), and arms 15 (12.0%) were predominantly affected parts of the body. Similarly, strain-sprain (26.4%), fall injury (12.8%), laceration (12.0%), and burn (11.2%) were commonly seen as types of injury (Table 1).
One hotel nurse noted that,
The record for the previous year was 42–46 accidents a year. Usually, the injured employee is on sick leave for 1–3 days. The most reported type of injury is back injury due to long-standing, the lifting of heavy objects without assistance, and the pulling and pushing of heavy trolleys and objects. The majority of accidents occurring during rush hours are caused by slips, trips, and falls. The severity of injuries varies from one department to another. But, as a rule, causes are explained to be preventable and modifiable. Most of the time, injuries are reported to outlet managers and supervisors on duty, immediately after the occurrence, first aid is given on-site, and then they may be referred to hospitals. Injury investigation is done and the incidence will be documented and reported to the security department. (Age 31 years, hotel nurse)
Severity of occupational injuries
Approximately, three-fourth, 74.4%, of injured respondents were hospitalized, with 26.1% of respondents stayed in the hospital for up to 5 days. The mean length of hospital stay was 1.36 days. Similarly, more than three-fourth, 76.6%, of injured workers took sick leave days (paid sick leave) and the median sick leave taken was 7 days. As a result of the accident, the study revealed that a total of 1015 working days were lost in the last 12 months, which indicated on average 11 days lost per injured worker. The study has shown that 52 (41.6%) respondents had disabilities, in which 50 (96.2%) and 2 (3.8%) were temporary and permanent types of disability, respectively.
In support of this finding, one security officer explained,
Most of the time an injured employee is entitled to a one-day sick leave day for a baseline medical treatment and insurance issues (treatment was covered by the employer or employees had health insurance). Hand fracture, fall from a ladder, and amputation of a worker’s fingers is the most severe type of injury; but the finger amputation injury happened was the severe one which has taken more workdays for recovery and rehabilitation. (Age 46 years, security director)
Factors associated with occupational injuries
In the bivariate analysis, educational status (p-value = 0.001), income level (p-value = 0.009), ethnicity (p-value ⩽ 0.001), sleeping disorder or problem (p-value = 0.035), working department (p-value = 0.023), work experience (p-value = 0.007), workplace supervision (p-value = 0.0112), family size (p-value = 0.041), khat chewing (p-value = 0.054), frequency of khat chewing (p-value = 0.086), shift work (p-value = 0.001), and PPE use (p-value = 0.061) were factors associated with occupational injuries.
Based on the bivariate logistic regression analysis, those variables that had a p-value of less than 0.25 were kept for the multivariable binary logistic regression analysis. Family size, educational status, sleep disorder/problem, work experience, and shift work remain statistically significant with occupational injuries (p-value < 0.05). Low educational status, sleep disorder, inexperienced workers, and shift work were the predictive/risk factors for occupational injuries, but having low family size was protective (Table 2).
Multiple logistics regression analysis showing significant factors with prevalence of occupational injuries among employees of the brand hotels, Kirkos sub-city, Addis Ababa, 2019 (p-value < 0.05).

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Statistically significant variables at p < 0.05.
Discussion
This study has revealed that the prevalence of occupational injuries was 37.9% (95% CI (32.7%, 43.8%)) in which similarities were shown with a study done among workers in Etab soap and detergent factory in Hawassa, Ethiopia (38.0%) 16 and is higher than the study conducted among production workers in iron and steel industry in Addis Ababa (33.3%) 17 and small-scale industrial workers in Yashio city, Japan (35.6%). 18 It is relatively lower than the studies conducted among building construction workers in Gondar city (38.7%) 12 and Addis Ababa waste collectors (43.7%). 19 Such variations in the prevalence of occupational injuries are linked to the variation and nature of activities carried out in different sectors’ work and level of development, the status of the workforce in a given country, and the strengths of occupational health services provided in different sectors. 20
In this study, those respondents who had four and below family members were 52% less likely to be injured than those who had five and more family members (AOR: 0.48, 95% CI (0.286, 0.818)). This finding is consistent with the study conducted among Addis Ababa city solid waste collectors. 21 The possible explanation for this could be that respondents who had more family members might be pre-occupied with extra thinking and time-strapped families coping with about their children and major family events might increase the risk of occupational injuries. 22
This study also showed a significant association between educational status and occupational injuries. Those respondents with relatively low levels of literacy were about 1.5 times more to be injured than those with a higher level of literacy (AOR: 1.466, 95% CI (1.098, 1.959)). This might be due to the fact that education is more likely to increase workers’ safety and health awareness and practices that can prevent them from occupational injuries. 17
This study found that employees who were working in shifts were 2.5 times more likely in getting occupational injuries than those who were not working in shifts (AOR: 2.559, 95% CI (1.197, 5.474)). Thousands of different shift schedules may have a quite different impact on worker’s health and safety particularly with reference to the amount of night work, timing, and duration of shifts, length of shift cycle, speed and rotation of shifts, and position and length of rest days. 20 According to a study done in Japan, shift work and health have explained that shift work has a relevant interference on personal, family, and social life, which may result in psychological stress and psychosomatic disorders. 21 Another comparative study done on shift and regular day workers in India showed that shift work, in particular night work, can have a negative impact on the health and well-being of workers as it could cause disturbances of normal circadian rhythms beginning with the sleep/wake cycle. 23 Different scholars have recommended appropriate workplace design and interventions on the organization of shift schedules according to ergonomic criteria and careful health surveillance and social support for shift workers are important preventive and corrective measures that allow people to keep working without significant health impairment.
The odds of injuries were 1.065 times among employees who served for 2 years and below compared with those who served for more than 2 years (AOR: 1.065, 95% CI (1.023, 1.108)). The possible explanation by different studies has explained that those employees who served for more than 2 years could be accustomed to the working environment and it is believed that employees with more experience on the job generally make fewer mistakes and could develop consciousness of safety procedures and which drives them to comply with safety precautions including proper use of PPE. 24
A study reported that sleep disturbances such as difficulty in initiating sleep, sleeping poorly at night, sleep insufficiency, and insomnia symptoms were significantly associated with the occurrence of occupational injuries. 25 This study has also revealed that workers who had sleep problems or disturbances were 1.86 times more likely to be injured than workers who did not have sleeping problems or disorders (AOR: 1.867, 95% CI (1.101, 3.166)). This result has shown similarity with a study done among textile factory workers in Amhara regional state, Ethiopia. 26 Most occupational health and safety studies conducted in developing and developed countries strongly agreed with this finding,20,26 which is due to the fact that the majority of workers in these hotels are employed in three shifts with an 8-h working time interval which has a potential to disrupt the sleep pattern of workers. The findings suggested that poor nocturnal sleep habits were associated with self-reported occupational injury. 20 This sleeping disturbance problem affects the ability to maintain wakefulness and concentration as well as the ability to assess or watch the work environment and working conditions and perform duties safely.21,23
Although this study has many strengths, it has the following limitations. The study had a shortage of studies from similar settings for comparisons. The possibility of social desirability bias that might be introduced due to employees might report more socially acceptable responses than their actual day-to-day practice. There might be recall bias as more serious and current injuries were remembered. To minimize such biases, training on probing techniques has been given to the data collectors and supervisors. As this is a cross-sectional study, the cause–effect relationship is not established between the different exposure variables and occupational injury. Moreover, there was a lack of considering seasonality or recidivism as a variable and interpersonal violence as an occupational injury in our study.
Conclusion
The results showed that the prevalence rate was very high. The key predictors of occupational injury were family size, low educational background, work experience, sleep disorders/problems, and working in different shifts. Therefore, the provision of safety training repeatedly and reinforcing it to increase awareness and understanding of workplace risk factors are recommended. Besides, further studies need to be conducted on safety knowledge and practice among employees of the study area and similar setups.
Supplemental Material
sj-docx-1-smo-10.1177_2050312120985273 – Supplemental material for Epidemiology of occupational injuries in Ethiopian hotel industry in Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_2050312120985273 for Epidemiology of occupational injuries in Ethiopian hotel industry in Ethiopia: A cross-sectional study by Roza Abune, Hailu Merga and Embialle Mengiste in SAGE Open Medicine
Supplemental Material
sj-pdf-1-smo-10.1177_2050312120985273 – Supplemental material for Epidemiology of occupational injuries in Ethiopian hotel industry in Ethiopia: A cross-sectional study
Supplemental material, sj-pdf-1-smo-10.1177_2050312120985273 for Epidemiology of occupational injuries in Ethiopian hotel industry in Ethiopia: A cross-sectional study by Roza Abune, Hailu Merga and Embialle Mengiste in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the Jimma University for funding this research. The authors’ gratitude also goes to the Addis Ababa city administration labor and social affairs bureau for facilitating the study. The authors also thank supervisors, data collectors, and all study participants for their commitment and cooperation in responding to the questionnaire.
Author contributions
R.A. (female) involved in the conception, designing methods, analysis, interpretation, and drafting of the manuscript. E.M. (male) and H.M. (male) participated in designing, data analysis, interpretation of the findings, and write up of the findings. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Jimma University Institute of Health institution review committee (ethics approval no. JUIRB/THRPGD/21/2019), and official permission was taken from each hotel administrative body.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Institute of Health of Jimma University. The organization has no role in the designing of the study, data collection, analysis, and interpretation of data, and in writing the manuscript.
Informed consent
The hotels’ administrators were informed about the objective and purpose of the study, and verbal informed consent was taken from each study participant.
Data availability
All data generated or analyzed during this study are included in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.