
Abstract
Background:
The number of Japanese expatriates has increased, many of whom undertake lifestyle changes to improve their health.
Purpose:
We aim to clarify the health-promoting lifestyles of middle and older age Japanese expatriates.
Methods:
This is a cross-sectional study. Participants comprised 95 long-term Japanese expatriates residing in popular destinations: the Philippines and Thailand. Health behavior was evaluated using a Japanese version of Health-Promoting Lifestyle Profile II and participants were compared with a group living in Japan. Multiple linear regression analyses were used to examine the factors that correlate with the score of physical activity, a Health-Promoting Lifestyle Profile II subscale.
Results:
The expatriates had significantly higher scores of physical activity and nutrition than the group living in Japan. Factors positively related to physical activity were communicative literacy, information on health management before leaving Japan, no history of hypertension, and sufficient English proficiency.
Conclusion:
The Japanese expatriates we studied were physically active and were careful about nutrition. To further increase their physical activity, better access to health information and enhancement of communicative literacy and of English proficiency are desired.
Keywords
Introduction
With rapid worldwide globalization, the number of Japanese expatriates has increased and Asian countries have proven to be a location of choice for many seeking to live abroad. 1 Residing in foreign countries is notably popular among Japanese retirees, especially when they reach 60 years of age. 2 The most common reasons retirees give for the desire to live abroad include a warmer climate, lower living costs, and a desire to experience another culture.3–5
When retirees live in a country different from their own, adapting to diverse cultures and local medical services can sometimes be problematic. Previous reports have described expatriate healthcare experiences, including dilemmas regarding choice of healthcare, availability of insurance, and quality of the care. 6 Many Japanese expatriates have therefore undertaken lifestyle changes to reduce the necessity of visiting local medical facilities, because local healthcare environments can differ from those in Japan. 7 Issues may emerge when visiting medical agencies, for example, such as language difficulties and problems with health insurance.3,4 Exactly how Japanese expatriates modify their health-related habits, behaviors, and activities has not been widely reported.
Such modifications to lifestyle may be affected by factors such as gender, age, marital status, medical history, and any present health issues. We suggest that to engage in favorable health behavior abroad, it is necessary to obtain information on local health management before leaving Japan and/or during the time abroad. The ability to comprehend and utilize such information is also necessary. 8 We propose that factors related to favorable health behaviors may be different from those in Japan, leading to the necessity for specialized health education and information services.
This cross-sectional study aims to clarify health behavior and to examine the related factors in middle and older age Japanese expatriates. This information could be used to inform what kind of health education and information services are relevant and useful for Japanese expatriates and with the aim of making their time in the destination country easier.
Participants and methods
Target areas and population
This cross-sectional study focuses on Asian areas that have experienced a notable increase in Japanese expatriates, within which Japanese retirees are believed to reside. In October 2016, the Philippines was home to 11,770 Japanese expatriates, with 1733 of these living in Cebu. 1 In Thailand, there were 68,908 Japanese expatriates, 3188 of whom were based in Chiang Mai. 1 As these cities were notably home to so many Japanese expatriates, we selected Cebu and Chiang Mai for this study.
The target population was all members of a Japanese circle aged ⩾50 years in the two cities. It was limited to Japanese expatriates who had been resident in the respective cities for longer than 3 months. 1 Japanese circles are membership-based organizations that foster mutual friendship among members and interaction with the local community. In each of the two community circles, the number of such members was anecdotally estimated to be nearly 150 people from the membership list at the time of the survey. This was initially an estimate because some registered members were thought to be actually living in Japan, and others may have delayed in becoming a member several months after moving to the country.
As this study focuses on clarification of the health behavior of middle and older age Japanese expatriates, all such members were targeted in this study, regardless of occupational/social status.
Data collection
The aims and procedure of the study were explained to the president of each Japanese circle. With their agreement, our anonymous questionnaires were distributed and collected through a volunteer member who handed out or mailed the questionnaires to all the members in the targeted age range. Questionnaire recipients numbered 151 members in Cebu and 148 in Chiang Mai. The survey was conducted between February and July 2017.
Variables
Health behavior
Health behavior was defined as an optional and continual individual activity considered to be beneficial to physical and mental health in daily life, regardless of the participant’s actual health condition. 9
It was evaluated using the Japanese version of the Health-Promoting Lifestyle Profile II (HPLP II).10,11 This has 52 items and six subscales: health responsibility, spiritual growth, physical activity, interpersonal relations, nutrition, and stress management. The respondent selected one answer from four categories for each question item. Each selected answer was rated from 1 to 4 points. A higher score indicates better health-promoting behaviors.
Socio-demographic attributes
The questionnaire asked for gender, age, employment status, information on family members living in the same house, English proficiency, the number of trips to a country other than Japan, the number of visits lasting 3 months or longer, and the length of stay at the present place (years).
For the answer to the question of family members living in the same house, participants could select multiple answers: “alone,” “Japanese partner,” “non-Japanese partner,” “children,” and “others.” For English proficiency, the answer options were “daily conversation,” “basic greetings,” “a few words,” and “none.”
Health literacy
Health literacy was defined as cognitive and social skill necessary to obtain, comprehend, and utilize health information, to make individual decisions, and to change one’s environment in order to improve and maintain good health. 12
It was evaluated using the 14-item Health Literacy Scale (HLS-14),13,14 which consists of five items on functional literacy, five items on communicative literacy, and four items on critical literacy. Answers were the level of agreement using a 5-point Likert-type scale ranging from 1 (disagree strongly) to 5 (agree strongly). A high score indicates a high ability to comprehend healthcare.
Social environmental factors
Personal medical conditions asked were self-reported notable history (hypertension, high cholesterol, and diabetes mellitus), use of medication(s) (antihypertensive, antihypercholesterolemic, triglyceride-decreasing, and antihyperglycemic), comorbidity and health issues while residing in the destination country, experience of visiting a medical institution, experience as an inpatient or outpatient, and source of local information (acquaintances, websites of government agencies, websites of private organizations, TV programs broadcast from Japan, and travel publications).
Medical support from Japan
The questionnaires also ascertained personal health conditions before leaving Japan. We also sought information and issues that were investigated or searched for before leaving Japan (examples include ability to use Japanese language in a local clinic/hospital, information on medical and surgical disorders, local medical expenses and health insurance in the destination country, local infection diseases, and possibility or availability of transport back to Japan in case of emergency).
The sources of information on the destination country used before leaving Japan were also asked (examples include acquaintances, websites of government agencies, websites of private organizations, and travel publications).
Data analyses
The number of respondents was 41 in the Philippines and 63 in Thailand, for a total of 104 (average response rate: 34.8%). Nine individuals did not adequately answer the question on age, and after their exclusion, the final number of valid respondents was 95 (effective response rate: 31.8%).
The data of the participants residing in the two countries were combined into one group (expatriate group) for the following three reasons: (1) this study aims to evaluate the health behavior of Japanese expatriates, (2) the number of participants analyzed would be insufficient if they were analyzed as two separate regions, and (3) health behaviors appeared to be similar despite differences in the local healthcare systems, because the results of our preliminary analysis indicated that there were few items among the 52 items of HPLP II showing a significant difference in the mean score between participants residing in the Philippines and those in Thailand.
In a previous study, there was no difference in occupation (fulltime or part-time/non-working) between the exercise and the non-exercise groups in Japanese residents in Malaysia (20 years of age or older). 15 In this study, we therefore used all the participants, regardless of their employment status.
To compare the health behaviors of the expatriate group with those of Japanese people living in Japan, our original database of 399 people was used to make the control group. 16 From the database, 190 people were matched two to one by gender and age (±10 years) with the expatriate group. The matching was performed four times, but the main results remained the same. Data from the first matching were therefore used in this study.
The original database was the result of our research to elucidate whether experience of Japan’s specific medical checkup system is associated with a health-promoting lifestyle, health literacy, and social capital by type of healthcare coverage. 16 It consisted of males and females randomly selected from 10-year age groups (forties, fifties, sixties, and seventies) living in “Kinokawa City,” Japan. “Kinokawa City” is located in the northern part of Wakayama Prefecture, Japan. The population was 62,616 in 2015 and there is one public hospital in the city. Data were collected via an anonymous self-administered mail questionnaire survey similar to the one used in this study. The purpose of the survey was different, so this database contains the current HPLP II and HLS-14, but it does not include the other question items from the study.
Non-responders were excluded from each analysis. Student’s t test was used to examine the difference in mean scores of the six subscales of HPLP II between the two groups and the effect size (Cohen’s d) was calculated in each subscale. 17
In the comparison of the two groups, the scores of physical activity and nutrition were significantly higher in the expatriate group. The effect size of the physical activity score was larger than that of the nutrition score. The main purpose of this study is to understand and promote health behavior, of which physical activity is very important.18,19 Wide variation was expected between participants regarding healthy diet, which is subjective, so we focused our investigation on physical activity. Consequently, only physical activity was selected for further analysis to examine the factors related to the health behavior.
Multiple linear regression analyses were used to examine the factors that correlate with the physical activity score. Regarding question items on socio-demographic attributes, social environmental factors, and medical support from Japan, the answers were divided into two categories and a dummy variable (0 or 1) was created. As for the language ability, “daily conversation” and “basic greetings” were divided into “no problems in daily life” and the other answers into “problems in daily life.” The number of trips to a country other than Japan was divided in relation to a cutoff point of 10 times, ⩾10 times being considered as “many times.” The number of visits lasting 3 months or longer was divided with a cutoff of two times and ⩾two times was considered as “many times.” For length of stay at the present place, 9 years was the cutoff and ⩾9 was considered as “longer.”
In the analyses, two models were set. The first model (Model 1) individually investigated the relationship to the physical activity score after adjusting for age and gender. The second model (Model 2) was used for variable selection based on the stepwise method after entering 17 items that showed a significant relationship to the physical activity score in the first model.
All statistical analyses were performed using SPSS Ver.24 for Windows (SPSS Japan). p < 0.05 was considered statistically significant.
Ethical consideration
Anonymous questionnaire sheets were forwarded to the participants, including a cover letter that explained the study aims and procedures, the protection of personal information and answers, that participation was voluntary, and that there was no disadvantage in non-participation. Submission of the questionnaire was considered to be consent to inclusion in the study. This protocol was approved by the Wakayama Medical University Ethical Committee (No. 1944).
Results
Socio-demographic attributes
The number of males in the expatriate group was 63 (66.3%) and their average age was 67.4 ± 8.3 (mean ± standard deviation) years. The average age of the 190 participants in the control group was 67.0 ± 7.5 years. There were 126 males (66.3%) (Table 1).
Socio-demographic attributes of the expatriate and control groups.
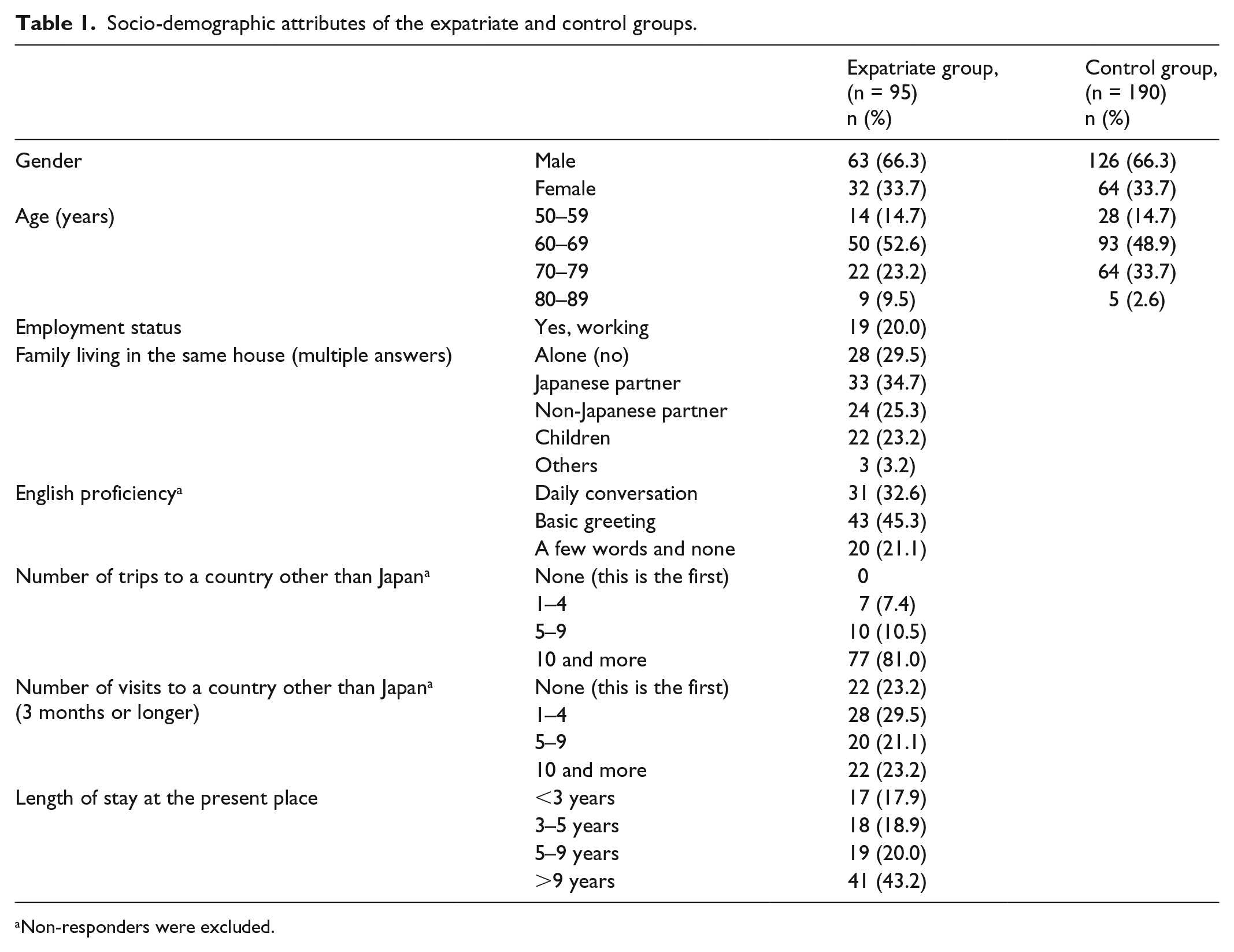
Non-responders were excluded.
In the expatriate group, 19 participants (20.0%) were working, 9 of whom were aged between 50 and 59 years. The number of participants living with a Japanese partner was 33 (34.7%), and 24 (25.3%) were living with a non-Japanese partner. For English proficiency, the number of participants who answered “daily conversation” was 31 (32.6%), while 43 (45.3%) answered “basic greetings.” The number of participants who had traveled 10 times or more was 77 (81.0%). The number of participants who had been for 3 months or more to a country outside of Japan 10 times or more was 22 (23.2%), and 41 (43.2%) had stayed at their present place for ⩾9 years.
Health behaviors
The scores in the expatriate group were higher than those in the control group, and the scores of physical activity and nutrition showed a significant difference, especially physical activity showed the medium effect size (Table 2).
Scores of six subscales of HPLP II in the expatriate and control groups.
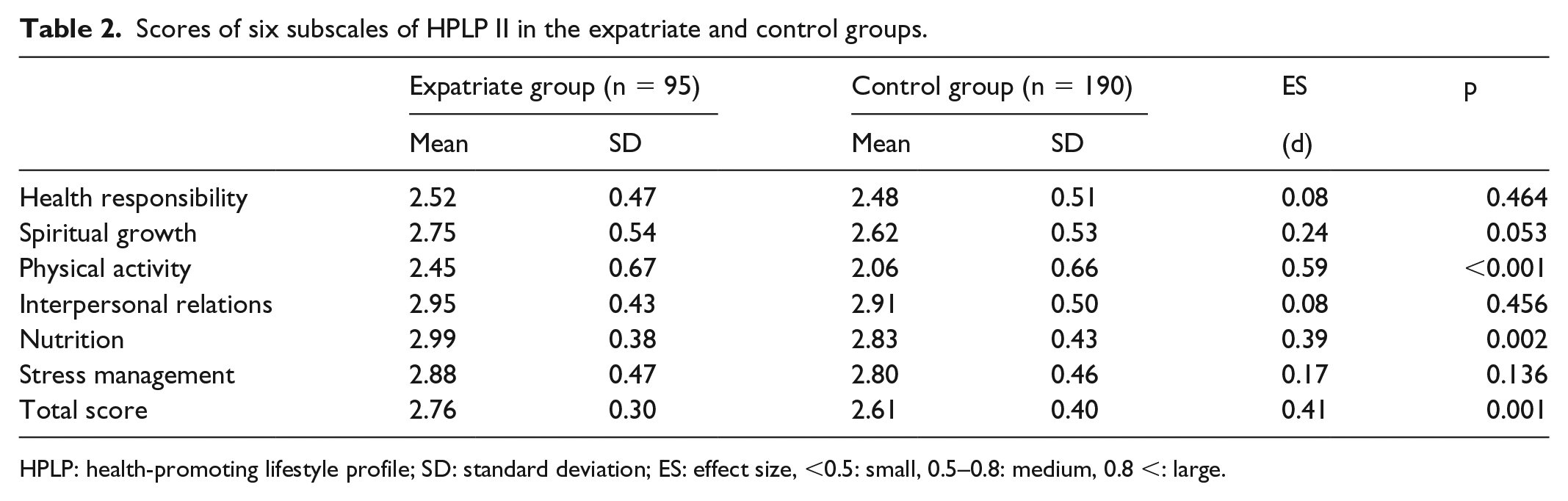
HPLP: health-promoting lifestyle profile; SD: standard deviation; ES: effect size, <0.5: small, 0.5–0.8: medium, 0.8 <: large.
Health literacy
The scores of functional literacy were 20.5 ± 4.7 points (n = 84), those of communicative literacy were 18.9 ± 4.7 points (n = 86), and those of critical literacy were 14.4 ± 3.6 points (n = 87).
Social environmental factors
Some participants had lifestyle-related diseases (hypertension 34/35.8%; high cholesterol 29/30.5%; diabetes mellitus 11/11.6%) and some used medication (antihypertensive 29/30.5%; antihypercholesterolemic 13/13.7%; triglyceride-decreasing 7/7.4%; antihyperglycemic 7/7.4%).
Some participants had age-related disease (eye diseases, ear diseases, joint diseases, urinary diseases such as prostatic hypertrophy and erectile dysfunction, and gynecological diseases, 32/33.7%), while 79 participants (83.5%) had visited a medical institution as an outpatient (61/64.2%) and/or as an inpatient (29/30.5%)
The participants obtained local information from acquaintances (47/49.5%), TV programs broadcast from Japan (22/23.2%), and from the websites of private organizations (21/22.1%).
Medical support from Japan
Some people had searched the ability to use Japanese language in a local clinic/hospital (35/36.8%), information on medical and surgical disorders (35/36.8%), local medical expenses and health insurance in the destination country (33/34.7%), local infection diseases (14/14.7%), and the possibility/availability of transport back to Japan in case of emergency (5/5.3%).
Some participants obtained local information before leaving Japan from acquaintances (34/35.8%), and websites of private organizations (21/22.1%), but few (11/11.6%) from websites of government agencies.
Factors related to the score of physical activity
Table 3 shows the items that had a significant correlation with the physical activity score after adjusting for age and gender (Model 1). Among the attributes, three items (living with a non-Japanese partner, no problems in daily life regarding English proficiency, and 9 years or more of staying at the present place) showed significant partial regression coefficients. Significant partial regression coefficients were shown in communicative literacy, eight items among the social environmental factors (hypertension, diabetes mellitus, antihypertensive, antihypercholesterolemic, triglyceride-decreasing, experience of visiting a medical institution, experience as an outpatient, and obtaining local information from websites of private organizations), and five items among the medical support from Japan (searching for local medical expenses and health insurance, searching for local infection diseases, searching for possibility/availability of transport back to Japan in case of emergency, obtaining local information before leaving Japan from websites of government agencies, and obtaining local information before leaving Japan from the websites of private organizations).
Relationship, adjusted by age and gender, of physical activity with socio-demographic attributes, health literacy, social environmental factors, and medical support from Japan.

No-respondents were excluded.
β: standardized partial regression coefficient.
Variable selection was performed using these 17 items (n = 86) (Model 2). Four factors were selected as independent factors related to the physical activity score (Table 3). They were communicative literacy, obtaining local information before leaving Japan from the websites of government agencies, having a history of hypertension, and having no problems in daily life regarding English proficiency.
Discussion
Characteristics of the expatriate group
Participants had considerable experience of living abroad. Among the expatriate group, 81% had traveled to a country other than Japan 10 times or more and 23% had been abroad 10 times or more.
In the earlier studies on the scores of HPLP II in Japan, the participants were relatively young, university students, 20 and people 18–64 years of age. 21 In earlier studies of non-Japanese people who were residing in a country other than Japan,22,23 participants had cultural features different from Japanese people, such as lifestyles. Thus, in this study, our original database was used to make the control group for the purpose of comparing their scores with those in the expatriate group, because of there being few earlier studies with Japanese subjects aged ⩾50.
The expatriate group was not especially health conscious. There was no significant difference in health responsibility score between the two groups. The score in the expatriate group was not so high compared with the score from hypertensive patients living in Japan aged >50 years (2.72 ± 0.49). 21
Physical activity was defined in this study as any bodily movement produced by skeletal muscles requiring expenditure of energy. Regular moderately intensive physical activity such as walking, cycling, or participation in sports has significant health benefits. 24 The expatriate group regularly engaged in healthy behavior. Their physical activity score was significantly higher than that of the control group. The score was also significantly higher than that of Japanese aged between 50 and 64 years (1.73: calculated from the table), 21 and that of Japanese people with hypertension aged >50 years (2.12 ± 0.63). 25
Health behavior can directly affect health outcomes. Health behaviors such as exercising and eating sensibly lower the risk of conditions such as cardiovascular disease and diabetes mellitus. 26 In the elderly, physical activity is recommended from the viewpoint of comprehensive health promotion, since physical activity has the possibility to reduce the risk of deterioration of daily function and to live longer with independence. 19 In this study we therefore focused on physical activity, and examined its related factors.
Factors related to physical activity
In multiple linear regression analysis, factors related to physical activity were communicative literacy, obtaining local information before leaving Japan from the websites of government agencies, having history of hypertension, and having no problems in daily life regarding English proficiency.
As the R2 is generally lower in attempts to predict human behavior, it was not high enough (0.300) in this study either, but the model shows that changes in the adopted four variables are associated with those in physical activity.
Communicative literacy is the ability to adapt to the changing environment using new information, 12 and the individual ability to enhance willingness and self-confidence to engage in activities based on advice from friends and acquaintances. 27 In an earlier report, health literacy was also positively related to health behaviors such as exercise, 8 a healthy lifestyle such as exercise frequency, 28 and good health status such as low level physical exercise aimed at health. 29 Thus, communicative literacy may very well play a key role in the promotion of physical activity.
Most Japanese people obtain information on medical conditions abroad from websites and travel companies before leaving Japan. 30 Among such sources of information, governmental websites are assumed to possess higher reliability. Accessing health information is important for positive health behavior and health status. 8 We suggest that those who use governmental websites appropriately may have access to health information and be more likely to engage in physical activity.
History of hypertension was negatively associated with physical activity score. Regular physical activity to an adequate degree reduces the risk of hypertension in adults. 24 Insufficient levels of physical activity when in Japan may have led to hypertension. Ideally, those with hypertension should undergo more physical activity while residing abroad.
Higher English proficiency may facilitate information acquisition by allowing better communication with local medical staff. As acquisition of health information from multiple resources is related to good health behaviors, 27 it may be easier for participants who display high English proficiency to become involved in physical activities.
Among the social environmental factors in Model 1, there was a negative association with physical activity in respondents who had diabetes mellitus, those who were given oral medication for hypertension, high cholesterol and/or high natural fat, and those who had experience of visiting a medical institution. Taken together, this could mean that more physical activity may successfully lead to better health condition 24 and reduce the necessity to visit a medical institution onsite or take an oral medicine. 24
Japanese travelers including expatriates obtain health information from guidebooks, websites, the local community, magazines onsite, and booklets in a medical institution. 29 In this study, those who searched local medical expenses and health insurance, local infection diseases, and possibility/availability of transport back to Japan in case of emergency before leaving Japan may have had greater awareness of health management, and thus were more conscious of health behaviors when they arrived in their destination country.
Necessity of an education and information service to live a healthy life abroad
In a medical environment different from that of the home country, it is especially important to actively pursue a healthy daily life. Since better communicative literacy may produce more physical activity, education to enhance communicative literacy is desired. The experience to act according to the obtained information or advice enhances its literacy. 31 We also recommend that participants have positive communication with friends and neighbors, and participate in Japanese circle activities.
Medical personnel are suggested to encourage those who will stay abroad to obtain suitable local information by every available means before leaving Japan. Many sources of information, such as governmental and medical institution websites, use English, but for medical purposes it is often difficult for the general public to understand. Medical personnel, thus, need to communicate such content in a comprehensible way. It is also important for the expatriates to improve their English proficiency in order to facilitate conversation with non-Japanese people, but the same could also be said for other, local languages.
Limitations
Asia is very large and has huge variation in culture. The participants in our study may not therefore be ideal representatives of Asia as a whole. In this study, the participants from two areas were combined and then analyzed. As a precaution, when HPLP II was compared among the groups after the expatriate group was divided into two groups, there were no significant differences in eight items of physical activity between participants residing in the Philippines and Thailand. In this trial, physical activity scores in both the Philippines and Thailand were significantly higher than those of the control group. The score of nutrition in Thailand was also significantly higher than that of the control group. These data suggested that the participants from the two countries conducted similar physical activities, but that nutrition could be influenced by the diet of the residential area.
The number of participants was insufficient, although the researchers endeavored to collect as many of the questionnaires as possible using various means, including sending reminders and by postponing deadline dates. Consequently, those who are highly conscious of health may respond, so health behavior indication may be disproportionately high. Those who do not respond may have low health awareness, and may not be performing health-promoting behavior.
The number of subjects analyzed in the multiple linear regression model was 86. The number of subjects per variable is required to be 10 or more in the logistic regression analysis and 2 or more in the linear regression analysis. 32 Although the number of subjects analyzed in this study was insufficient, the number of subjects per variable exceeded 20.
The utility of these results may be limited, but this study provides a base for further study concerned with support for the health of Japanese expatriates. Prospective research using a larger number of participants in more diverse areas is needed to establish detailed intervention programs.
Conclusion
Japanese expatriates residing in the Philippines and in Thailand had significantly higher scores of physical activity and nutrition among six subscales of HPLP II than the control group of Japanese people living in Japan. Factors positively related to physical activity were communicative literacy, obtaining local information from governmental websites before leaving Japan, having no history of hypertension, and having sufficient English proficiency. To further increase physical activity of Japanese expatriates, education to enhance communicative literacy and facilitation of higher level of access to health information, such as to reliable websites and enhancement of English proficiency are desired.
Footnotes
Acknowledgements
We sincerely appreciate the cooperation of the representatives of the Japanese circles in Cebu and Chiang Mai, the participants of this study, and many people involved in this study. We acknowledge proofreading and editing by Benjamin Phillis at the Clinical Study Support Center, Wakayama Medical University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Wakayama Medical University Ethical Committee (No. 1944).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI, Grant No. JP 16K01794.
Informed consent
A cover letter explaining the study aims and procedures, the protection of personal information and answers was forwarded to the participants with anonymous questionnaire sheets. It stated that participation was voluntary and that there were no disadvantages to non-participation. Submission of the questionnaire was considered to be consent to participation in this study.