
Abstract
Objective:
This study evaluated the perception of users of complete dentures (successful cases) provided by the public health service throughout the course from tooth loss to rehabilitation.
Methods:
A total of 11 individuals who received their complete dentures through the public health service were interviewed according to a qualitative approach based on three pre-established topics: (1) tooth loss, (2) living without teeth, and (3) living with dentures. The obtained material was submitted to content analysis.
Results:
Individuals associated the socioeconomic status with lifelong oral health experiences and difficulty to access oral treatment. Tooth loss was the solution to pain and sometimes perceived as a natural event of life. Living without teeth was a negative surprise that resulted in physical and psychological impairments. The period of adaptation to dentures represented suffering and required psychological efforts to be successful.
Conclusion:
The dentures represented a reward for the suffering and recovered normal function, appearance, and socialization.
Introduction
The prevalence of edentulism in the global population has declined over the last few decades, with a 45% reduction between 1990 and 2010, but it remains a public health problem in Brazil and several parts of the world, affecting 2.3% of the world population in 2010, corresponding to 158 million people. 1 In 2010, countries such as Brazil, Turkey, Iran, Mexico, and New Zealand showed a prevalence for severe tooth loss (<9 permanent teeth) significantly higher than the global average. 1
Edentulism is an essential marker for evaluating oral health policies and is associated with the health conditions of the population. 2 However, this condition is not yet seen socially as an issue deriving from wasteful programs and policies, but as a typical lifelong process that is influenced by fatalistic beliefs about the inevitable loss of teeth with age, acting negatively on the acceptance of dental treatment.3,4
Dental absences can be considered a devastating and biologically disturbing event that can lead to the impairment of oral functions and ensuing psychological problems, with lower self-esteem, lower social integration,4–6 and a feeling of disadvantage for many individuals. 7 In this context, rehabilitation with a dental prosthesis is seen as a replacement of part of the missing body because it can recover the compromised oral functions and is a return to socially accepted standards and rejuvenated self-image.4,8,9
There are many studies about the perception of tooth loss2,3,5,10 and feelings involving prosthetic rehabilitation.4,9,10 However, qualitative studies that investigated the feelings of edentulous individuals throughout the course from tooth loss to prosthetic rehabilitation carried out among successful cases of rehabilitation with complete dentures were not identified. The reconstruction of this course can contribute to the comprehension of the connections among different feelings involving tooth loss and dental rehabilitation. In addition, the recognition of subjectivity is vital for the care plan of individuals and can guide the choice of approach that provides improved well-being and contributes to more qualified and humanized care.
In this context, this study aimed to evaluate the perception and feelings of users of complete dentures (successful cases) provided by the public health service throughout the course from the tooth loss to the rehabilitation.
Methods
Design
This article was reported according to the consolidated criteria for reporting qualitative research (COREQ) 11 (Supplemental material). A qualitative descriptive case study was conducted. 12 Qualitative methods are indicated to interpret phenomena that are difficult to measure quantitatively, as people’s life experiences, 13 perspectives, their beliefs, and attitudes, as well as providing an in-depth study of a specific topic, contributing to studies in the field of Dentistry. 14 In this study, the phenomenon under investigation is the perception and feelings of users of complete dentures provided by the public health service throughout the course from the tooth loss to the rehabilitation.
Research team
Six researchers (five women and one man) participated in this study, including a public oral health MSc student (L.M.L.L.d.P.), a dental prosthetist (A.A.S.), an undergraduate dental student (J.G.C.), and four researchers in public oral health (E.F.E.F., V.E.G., A.A.S., and R.C.F.). Four of the researchers (E.F.E.F., V.E.G., A.A.S., and R.C.F.) had previous experience in qualitative study designs and had no prior relations with the patients included. All the interviews were conducted by L.M.L.L.d.P.
Participants
The subjects were edentulous individuals of both genders with different age groups, marital status, and household income, who used the public oral health service. A purposive sampling was used. These individuals were intentionally selected among participants of a 7-year follow-up study that evaluated user satisfaction and the quality of complete dentures provided by primary health care (PHC) in Belo Horizonte, Brazil 15 and who used at least one of the complete dentures (successful cases), considering the individual necessity. This led to 11 participants being involved in the study.
Recruitment
The recruitment was initially conducted by phone, where the individuals were asked about the place they wanted to be interviewed and all chose their homes. The home visit was scheduled after subjects consent and took place from January to March 2018. The researchers, during the home contact session, presented themselves and explained the purpose and methods of the study to the individuals who met the inclusion criteria. The subjects were clarified as to the formation and institutional link of the researchers with the university and the confidentiality of their identities during the publication of the research results. The researchers also clarified all questions of the subjects. It is important to highlight that the interviewers had no conflicts of interest or any relationships that could bias the results of this study.
Then, it was allowed for patients to decide whether they wish to participate, and they were given a replica of the informed consent, where it was requested to provide written informed consent and permission to tape the interviews. Two selected subjects did not agree to participate in the study, arguing that they would not like to be interviewed.
Data collection
A semi-structured interview, in Portuguese, lasting about 40 min, was conducted and audio taped with each subject using an interview guide. According to the study aim, three themes were pre-established for this research: (1) tooth loss, (2) living without teeth, and (3) living with complete dentures. The interview was conducted by a researcher followed by an observer researcher. Data collection and analysis were conducted simultaneously and continued until new interviews did not provide any additional information and data already found were rich and deep for researchers (saturation strategy).16,17 The saturation strategy of responses was used to close the number of interviews and interviewees included in the study. The participant validated the summary of the data presented by interviewer shortly after the end of the interview.
Initially, a pilot study was conducted with three taped interviews with subjects selected from the same sample of the follow-up study. These interviews were transcribed and discussed among the team of researchers (interviewer, observer, and four experts in qualitative research). There was a change in the interview guide and the interviewers’ approach to ask about the participants’ feelings and perception, according to the study aim. The data obtained by these interviews were not included in the principal study.
Data analysis
The interviews were transcribed by one researcher, and the team of researchers performed the analysis. The transcribed material was read exhaustively to obtain a more in-depth understanding. 16 Subsequently, data were categorized using the MAXQDA 12 software and analyzed according to the content analysis proposed by Graneheim and Lundman, 18 where the units of meaning were identified and established through statements. In the next step, the essence of each unit of meaning was extracted, creating the condensed meaning. From then on, the analysis allowed the identification of categories referring to the pre-established themes. In this study, codes were used to represent each of the subjects (e.g. E01 and E02).
Ethical considerations
The Research Ethics Committee of the Federal University of Minas Gerais and the Municipality of Belo Horizonte approved this research (CAAE: 06781912.8.0000.5149), and all subjects signed the informed consent form before their participation in the study. The subjects were informed about the objectives and procedures of the research and about the absence of a relationship between the research team and professionals of the oral health public service where the dentures were provided, ensuring the privacy and confidentiality of the information.
Results and discussion
Seven women and four men with a mean age of 71.1 years (±6.3) participated in this study. Concerning the marital status, nine (81.8%) had a partner. Six respondents had a monthly household income of <US$253.00 (US$253.01–US$759.00: four participants; >US$759.00: one participant), reflecting the context of the Brazilian population of public health service users. Eight were using the pair of complete dentures, and three used only the upper denture.
The analysis showed that the course from tooth loss to rehabilitation with complete dentures involved positive and negative feelings (Figure 1). The socioeconomic status emerged from the subject’s statements and was not a pre-defined theme. However, it was present in several of the participants’ statements who associated it with lifelong oral health experiences, therefore, also presenting as a theme. For better elucidation, the statements were shown within each theme, highlighting their most relevant aspects (Tables 1–4).

Patients’ perceptions reported from tooth loss up to full denture rehabilitation.
Socioeconomic status
A lack of financial resources was the leading cause of tooth loss for many since it made access to dental treatment difficult. These individuals accessed only public oral health services which did not offer conservative treatments for adults.2,19 The current policy at the time they experienced their tooth losses was not based on comprehensive care that includes oral health education and promotion (Table 1). 20 The struggle for survival and other priorities (raising children, providing a home, and supporting a family) used the life and financial resources of the subjects. Thus, oral hygiene care was left on the sidelines, contributing to deteriorating oral health. The location of the health centers was a geographical barrier to access to the service, possibly due to the difficulties of moving from one place to another experienced by these subjects.
Statements related to the theme “socioeconomic status.”

Historically, in Brazil, there has been a lack of access to public oral health services for adults due to low coverage, 21 especially for individuals living far from large urban centers.22,23 The previous study showed the impossibility of oral health care by individuals belonging to a lower social class and living in inequality contexts. 2 In this context, popular practices were used as an alternative to resolving pain and suffering. Similarly, self-care with home treatment methods was a strategy for pain relief among patients with a low socioeconomic status in rural areas of India 24 and North Florida. 25
The socioeconomic status determined the choices and possibilities of treatment with complete dentures or other options for dental rehabilitation. The high cost and lack of access to oral health services were barriers between the need for and use of the dental prosthesis, keeping the edentulous condition for longer. The desire to have a prosthesis was often idealized in people’s dreams and imaginations. 2 In Brazil, the supply of complete dentures in PHC was established in 2004 through the National Oral Health Policy (PNSB).20,26 With this policy, public health service users achieved their dreams and felt grateful for the “miracle” or “received gift.” This feeling reveals that participants did not recognize oral health care as a constitutional right.
The participants’ socioeconomic status may also have influenced the acceptance of the complete dentures by them as conventional complete dentures were the only available treatment for dental rehabilitation in the public service; participants seem to accept the status quo. According to Vieira and Leles, 27 sociocultural factors may influence the subjects’ attitudes depending on their vulnerability. Although implants are an appropriate option for the retention and stability of the prosthesis, 7 few participants expressed the desire for this treatment. This may be because the participants considered the implant to be still inaccessible, and others referred to bone loss and age as a contraindication for this therapy. Among the main reasons for the refusal of treatment with implants in elderly patients were fear of pain, complications, and social embarrassment, all of which were exacerbated by age. 28
Tooth loss
Table 2 summarizes the positive and negative feelings of the theme of tooth loss.
Statements concerning the positive and negative feelings related to the theme “tooth loss.”

Extraction was the way to pain relief, the solution to dental, buccal, and systemic problems, and it was considered a natural event of life. As previously observed among individuals of a disadvantaged social class, 29 extractions were seen as the only possible and definitive solution to solve toothache. 3 Pain relief was the primary compensatory benefit for the disadvantages of edentulism. Extractions were also a solution for the appearance and embarrassment when natural teeth were big and with a large overjet due to periodontal disease. The inflammation and severe loss of tooth-supporting tissues, formerly known as “pyorrhea,” has also been previously reported30,31 as a reason for tooth extraction, because it is commonly considered to be irreversible and unavoidable. Tooth loss was also associated with improved bad breath and easier oral hygiene. Tooth extraction was a quicker and less problematic solution than other dental treatments, and it was considered a consequence of the failure of previous conservative treatments since the restorations are seen as “patches” that do not compensate. This perception can manifest previous negative or frustrating experiences or the disbelief of individuals in conservative dental practice. As already observed, 32 the participants like not having to consult the dentist anymore since with extractions, the problems would be solved in a single visit, thus being free of “engine noise” and “needles.”
The teeth were associated with the presence of systemic diseases and extracting them was the solution. Guidance from dentists and physicians has been shown to interfere in decision-making. As already mentioned by Gibson et al., 30 the decisions and actions of the dentist in the treatment through dental extractions and prostheses are perceived by the individuals as a natural solution to problems related to the teeth and gums. On the contrary, it is explicit that the previously existing mutilating practice in Brazil 19 made the dentist primarily responsible for the act and the patient a passive subject. This can be observed in the following statement: “The dentist prescribed some drugs and said: ‘come back and extract it when the inflammation wears off’” (E08).
In this study, the respondents perceived the tooth loss as a natural, inevitable, and culturally common event of life; they did not feel stigmatized by edentulism, although previously it has been seen as a marker of social inequalities. 15 The feeling that tooth loss is a natural part of aging31–33 was previously observed. Another aspect that may interfere with the perception and attitude toward edentulism concerns interpersonal comparisons and would lead someone to believe that being edentulous is normal when other family members are as well.
Those who became edentulous also manifested negative feelings since tooth loss was compared with amputation, resulting in incompleteness. This “terrible” feeling has psychosocial and physical consequences for those who recognized themselves without a part of the body. 33
Living toothless
Living toothless was considered “a negative surprise,” and the participants manifested only negative feelings (Table 3).
Statements concerning the negative feelings related to the theme “living toothless.”

Edentulism was related to disability and impairments, psychosocial implications and constraints, due to physical, biological, and emotional changes; these findings were similar to Ferreira et al. 2 The most frequent impacts felt in living toothless were on the functional losses in chewing, swallowing, and appearance, contributing to the feeling of being “badly finished,” incomplete, and unequal. Without teeth and prostheses, chewing was compromised, and food became “tasteless,” and as a coping strategy, subjects began to select or blend foods, especially those with a harder consistency which could lead to the impoverishment of daily nutritional consumption.33–35 According to previous findings,34,36 living toothless affected socialization since the embarrassment was more significant when attending events and talking with people outside of their social life and lower when relationships were within the family. Being without the prosthesis at home seemed to cause no embarrassment due to many years of a marital relationship, showing that edentulism appeared not to affect the intimate relationship with their spouses.
Living with complete dentures
The respondents experienced negative feelings during the period of adaptation to new complete denture (Table 4). In this process, the participants reported pain and discomfort, which result in impairment in oral functions, such as food selection, as previously described in the literature. 31
Statements concerning the positive and negative feelings related to the theme “living with complete dentures.”
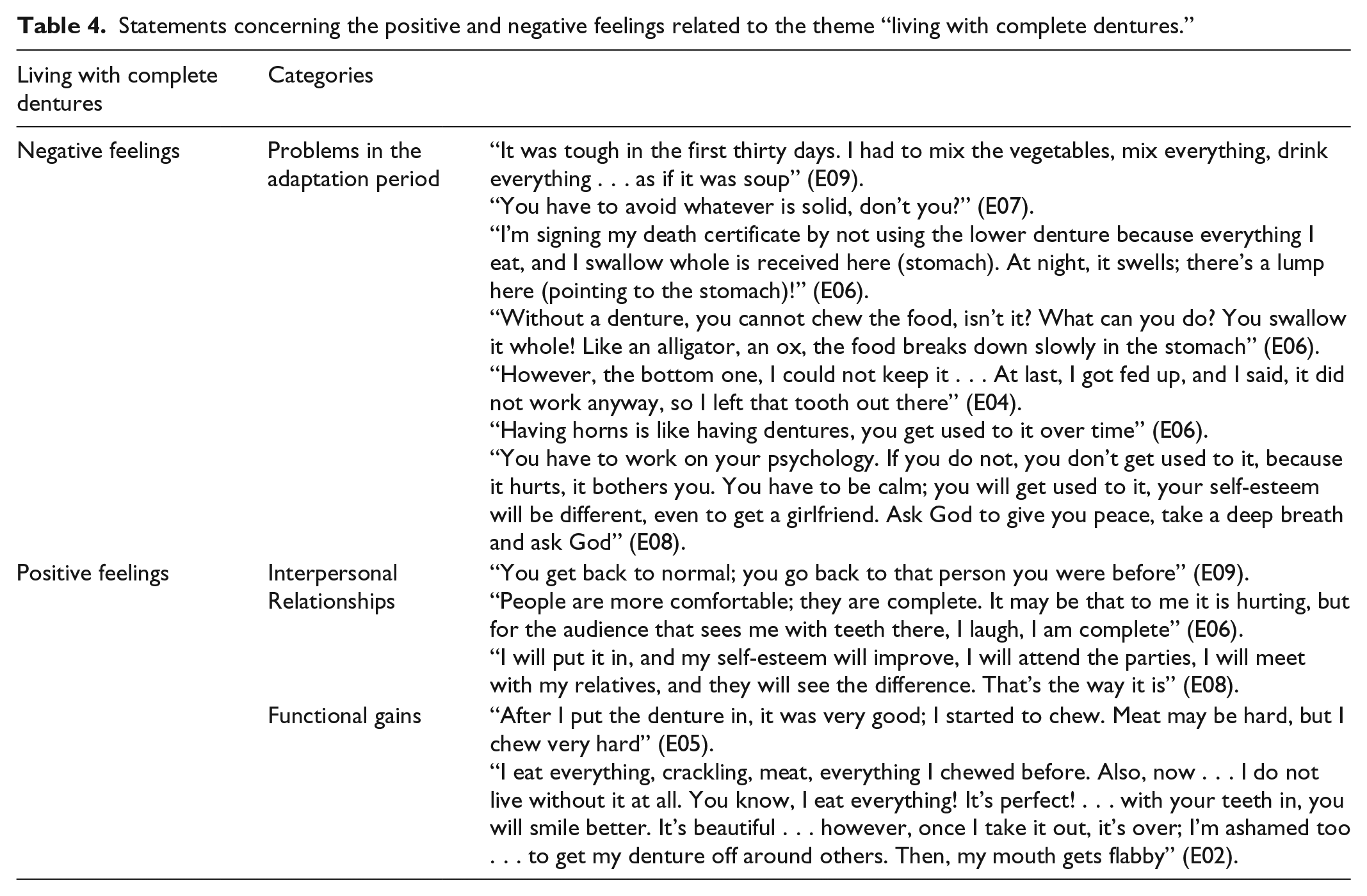
The lower dentures represented the main cause of negative feelings, and one respondent said that when he was not using it, he was “signing his death certificate” because of compromised chewing and, consequently, his general health. In some cases, discomfort caused by pain and instability of the dental prosthesis has outweighed any aesthetic and functional benefits which can often justify abandoning the use, especially of the lower complete denture. A quantitative study showed a lower percentage of use of the lower complete denture 5 years after installation. 14 These facts may reinforce the idea that the lower complete denture may not be the best substitute for teeth because it causes difficulties and discomfort. 37
Participants reported needing to get accustomed to the dentures, even if it bothers them, dealing with the psychological or seeking divine strength. This result showed that subjects presented resilience and adaptability to cope with a disability resulting from reduced oral function. 32 The resolving of problems caused by the use of the dentures showed that acceptance in the face of difficulties was also linked to religious beliefs since resorting to God contributed to the solution. In a previous study among Saudis, it was concluded that spiritual belief could significantly soften the impact of serious life events. 38 The high level of tolerance with complete dentures may also be related to acceptance of the type of rehabilitation provided in the public service since few looked at the use of an implant-supported prosthesis.
Adaptation to the use of dental prosthesis contributed to overcoming the limitations caused by the edentulism. The use of a complete denture seemed to replace the missing part of the body, and some participants felt “complete” again, returning to the person they used to be, corroborating with previous findings.9,36,38 It brought back to normal what once felt abnormal (living toothless), positively influencing self-esteem and socialization. Functionality gains were observed by reports of a resumption of chewing, with the recovery of the capacity to eat everything, the same way as when they had natural teeth. Rehabilitation also affected the appearance because the participant felt more beautiful with the prosthesis. They were able to smile better, without embarrassment. In addition, the complete denture had been seen as something that lasts forever, unlike the permanent dentition, seen as something fleeting.
The findings of this study were similar to those observed in countries of different economic levels regarding the feelings of living without teeth, suggesting that this life event similarly affects the subjects in different contexts.31–33 The choice of prosthetic rehabilitation is determined not only by the socioeconomic status but also by self-perceived oral condition and fear of suffering related to implant surgery.28,32 The adaptation to the prosthesis is an individual experience, painful for many and that needs to be supported and overcome to be successful.
This study highlights the importance of establishing a professional–patient relationship during treatment with dental prostheses. The professional should clarify the limitations inherent to the use of prosthesis and perform maintenance after its insertion, seeking to correct imperfections that make this moment less painful. The professional should be willing to listen to the patients’ expectations and complaints and advise on the need to make adjustments after the insertion of the prosthesis, which can minimize the yearnings and sufferings and demystify the pain of adaptation as necessary for success with the use of the prosthesis.
The feelings experienced during edentulism and adaptation with the prosthesis may have been attenuated over time, as participants reported on events that occurred in their history, as well as being prone to changing values throughout life. However, it is believed that the striking facts of life remain, and to this end, it is appropriate to consider the feelings reported by participants through the reconstruction of the life experience’s history.
Conclusion
The course from edentulism to rehabilitation involved positive and negative feelings, and the socioeconomic context defined the choices and ways of experiencing similar problems by people and influenced the beliefs and behaviors that resulted in edentulism as well as the resignation with the complete dentures.
Supplemental Material
Checklist – Supplemental material for The course from tooth loss to successful rehabilitation with denture: Feelings influenced by socioeconomic status
Supplemental material, Checklist for The course from tooth loss to successful rehabilitation with denture: Feelings influenced by socioeconomic status by Lara Melina Leite Lima de Paula, Aline Araujo Sampaio, Josué Gomes Costa, Viviane Elisângela Gomes, Efigênia Ferreira e Ferreira and Raquel Conceição Ferreira in SAGE Open Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Research Ethics Committee of Federal University of Minas Gerais, and the Municipality of Belo Horizonte approved this research (CAAE: 06781912.8.0000.5149).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the Postgraduate Program of the Faculty of Dentistry of the Federal University of Minas Gerais and CAPES for translation funding. They would also like to thank FAPEMIG (R.C.F. received the financial resources via the Minas Gerais Researcher Program PPM-00686-16 and PPM-00603-18).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.