
Abstract
Objective:
To describe substances, clinical manifestations, treatment, and medical outcomes of substance abuse exposures among older adults in Thailand.
Method:
This is a retrospective study of individuals aged 60 years or older with intentional abuse exposures reported to the Ramathibodi Poison Center from 1 January 2010 to 31 December 2017.
Results:
Forty-four cases were reported. The most common manifestation was somnolence (20, 45.5%). The most common substance used was kratom. There were 12 severe and fatal cases. Only one died due to methadone abuse. The most frequent manifestation among severe cases was respiratory failure (8 of 12 cases, 66.7%). Two cases had severe metabolic acidosis and were treated with hemodialysis. Three cases received norepinephrine.
Conclusion:
Substance abuse in the elderly is a serious problem that is often overlooked. Health personnel should promptly recognize and address this issue in order to reduce morbidity and mortality in the elderly population.
Introduction
Substance abuse is defined as hazardous use of psychoactive substances, resulting in dependence syndrome. 1 These psychoactive substances include illicit substances, alcohol, and some prescribed and over-the-counter medications (opioids, benzodiazepines, and sedatives).2,3 Thailand is an aging society, with 15% of the population aged 60 years or older. 4 The prevalence of substance abuse in the elderly has been estimated to be as high as 16%; however, this issue has received very limited attention and is often underreported. 5 A previous study by Duncan et al. 6 revealed that substance abuse in the elderly involved illicit substances (including cocaine, marijuana, inhalants, and methamphetamine) to a greater degree compared to alcohol and prescribed medications. The risk factors for substance abuse among older adults are chronic illness, polycomorbidities, physical disabilities, concurrent psychiatric problems, bereavement, and social isolation. In addition, substance abuse has negative health outcomes, leading to morbidity and mortality due to health issues, including cardiovascular diseases, arrhythmias, hypertension, cardioembolism, falls, and nutritional deficiencies.7,8 Severity of substance abuse in elderly populations may be different from that of younger populations, due to a higher number of comorbidities, and other age-related physiologic, pharmacokinetic, and pharmacodynamic changes. 9 Moreover, there is strong evidence to support associations between substance abuse and mental health problems, such as depression, hallucinations, sleep disorders, and dementia. 10 In Thailand, there is no study on substance abuse in the elderly population. This study aimed to describe the incidence, substances used, clinical manifestations, treatment, and medical outcomes of substance abuse among older adults in Thailand.
Materials and methods
Study design and data collection
The study is a retrospective review of adults, 60 years or older, with intentional abuse exposures, reported to the Ramathibodi Poison Center from 1 January 2010 to 31 December 2017.
The Ramathibodi Poison Center is the first poison control center in Thailand. It has been receiving consultations from across the country for 22 years. There are approximately 20,000 consultation calls per year. Calls are received and tracked by specialists in poison information (SPIs) whose training includes 30 h of didactic and 20 sessions of supervised practical instruction. Advanced consultations for more complicated cases are also available from medical toxicologists. Follow-up calls are made to provide ongoing recommendations and determine medical outcomes. These data are recorded in the poison center database.
Cases of elderly individuals with intentional abuse exposures were extracted by senior poison center information scientists with experience in using the poison center database. The search term “intentional abuse” was utilized. Demographic data, lists of substances and ingredients, duration from exposure to medical attention, clinical effects, initial severity, treatment, and clinical outcomes were reported. The severity of the case was determined using the IPCS/INTOX Poison Severity Score. 11
Statistical analysis
The data were analyzed and presented using descriptive statistics. Categorical data were described as number and percentage. Mean ± standard deviation (SD) or median and interquartile range (IQR) was used for describing continuous data. All statistical analyses were performed with SPSS for Windows Software Package, Version17 (SPSS Inc., Chicago, IL, USA).
Ethical considerations
The study was approved by the Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Protocol Number: ID 01-61-30. As the study involved retrospective secondary analysis of existing collected data from routine care without reporting of identified data, exemption from the requirement of informed consent was obtained from the Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University.
Results
During the study period, 44 cases of adults aged 60 years or older with intentional abuse exposures were reported, which included 28 (63.6%) males and 16 (36.4%) females (Table 1). The mean age was 68.5 years (SD = 6.7). The most common comorbidity was hypertension (four cases, 9.1%). Oral exposure was the most common route (41 cases, 93.2%). Four inhalation exposures were reported including two opium use, one toluene use, and one amphetamine use. There were two intravenous (IV) exposures, including one methamphetamine use and one with heroin. The most common category of exposed substance was illicit substances (61.4%), including kratom (31.8%) (Table 2). The most common initial severity of substance abuse was minor (37 cases, 84.1%). Thirty-two cases (72.7%) reported time of exposure. The median duration from exposure to initial medical assessment was 9.5 h (IQR: 1–42 h). Only 10 cases (22.8%) reported exposure to more than one substance.
Characteristics of substance abuse in the elderly reported to the Ramathibodi Poison Center during 2010–2017.

SD: standard deviation; COPD: chronic obstructive pulmonary disease; IQR: interquartile range.
Types of substance exposure reported to the Ramathibodi Poison Center.

Common clinical effects were somnolence (20, 45.5%), agitation (13, 29.5%), dyspnea (11, 25%), and hypertension (9, 20.5%) (Table 3). Reported tachyarrhythmias included sinus tachycardia (7, 15.9%), atrial fibrillation with rapid ventricular response (1, 2.3%), and supraventricular tachycardia (SVT) (1, 2.3%). There were eight cases (16.8%) with respiratory failure, eight cases (16.8%) with acute kidney injury, four cases (9.1%) with first seizure, and four cases (9.1%) with myoclonus. First, episode seizure was reported in cases of tramadol (one case), kratom (two cases), and opium (one case) abuse. Myoclonus was reported in cases of kratom (three cases) and ethanol (one case) abuse.
Clinical effects of substance abuse cases reported to the Ramathibodi Poison Center.
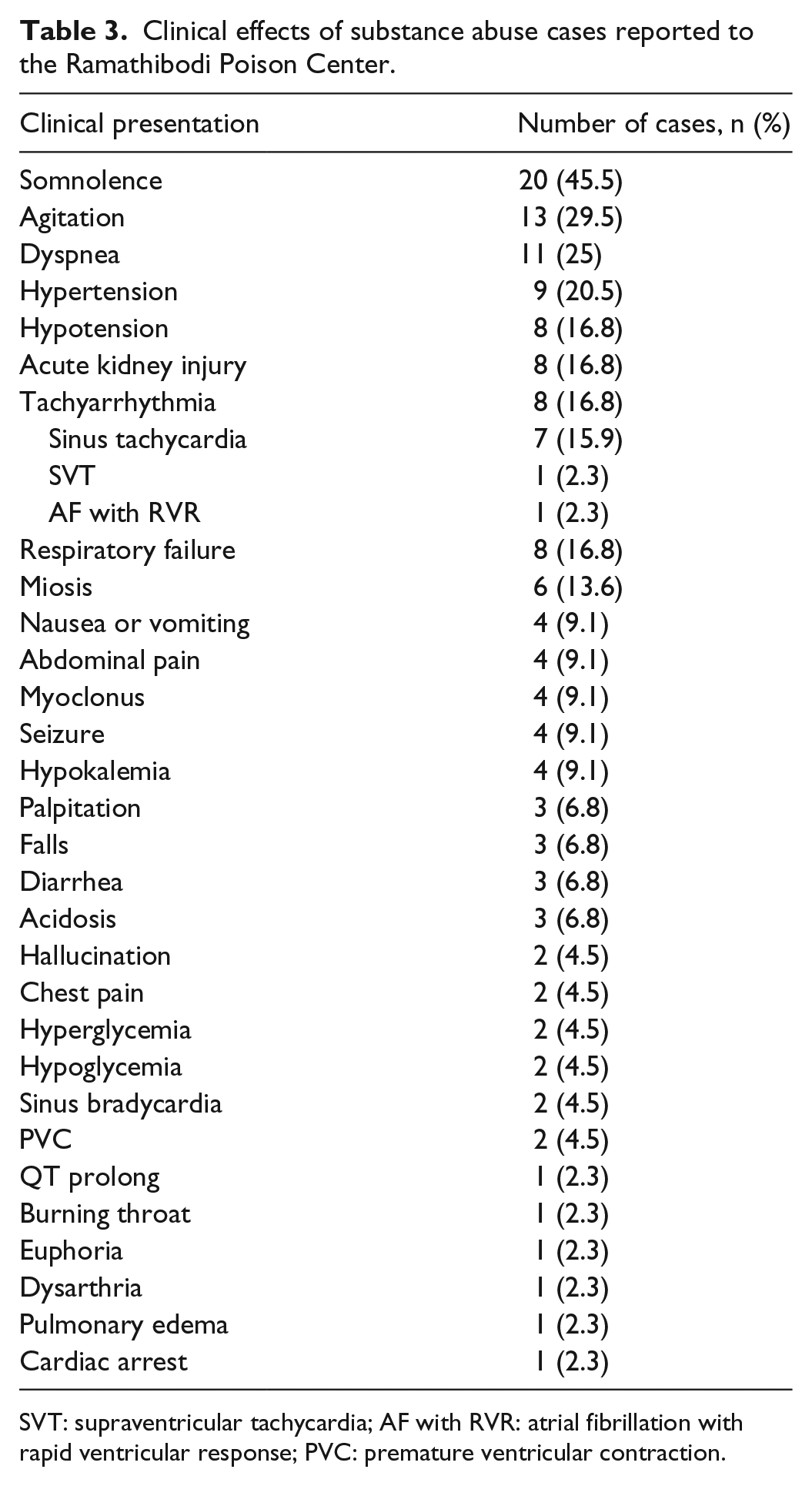
SVT: supraventricular tachycardia; AF with RVR: atrial fibrillation with rapid ventricular response; PVC: premature ventricular contraction.
Common treatments were oxygen supplement (16, 36.4%), IV fluids (14, 31.8%), benzodiazepines (14, 31.8%), antibiotics (13, 29.5%), intubation and ventilator support (8, 16.8%), and vasopressors (5, 11.4%) (Table 4). The prescribed vasopressors were norepinephrine (3, 6.8%) and dopamine (2, 4.5%).
Treatment of substance abuse reported to the Ramathibodi Poison Center.

There were 11 cases (25%) with severe outcomes and one death (2.3%) (Table 5). All severe and fatal cases were admitted to the intensive care unit (ICU). The most common category of substance use in severe cases was illicit substances. The details of cases with severe and fatal outcomes are as follows (Tables 6 and 7):
Case 1. One fatal case was a 69-year-old female with an unknown period of methadone exposure who developed respiratory failure, SVT, severe hypotension, comatose state, and later cardiac arrest. She was treated with IV fluid resuscitation and intubation with ventilator support.
Cases 2 and 3. Two cases involved opium use. Case 2 developed severe acidosis, renal failure, severe hypotension, and respiratory failure and was managed with hemodialysis, intubation, and norepinephrine (NE). Case 3 used opium in combination with IV heroin. He had miosis and was comatose. He was treated with naloxone, which is an opiate antidote.
Cases 4 and 5. Two cases involved methamphetamine abuse. Case 4 was comatose, had respiratory failure, and developed venous sinus thrombosis as complications. Case 5 used crystal methamphetamine and developed severe hypotension, acidosis, renal failure, and an abdominal infection. This patient was treated with NE, antibiotics, and hemodialysis.
Cases 6–11. Six cases used kratom. Five cases (cases 6–10) developed kratom intoxication. Case 11 presented with kratom withdrawal. One of kratom intoxication cases had concurrent ethanol use and developed comatose, respiratory failure, and ischemic stroke. In five severe cases with kratom abuse, clinical effects were respiratory failure (three cases), hypotension (two cases), seizure (two cases), comatose status (two cases), acute kidney injury (one case), and miosis (one case). In terms of treatment, one case received phenytoin and another case received NE. The kratom withdrawal case had hypotension, agitation, and respiratory failure. She was treated with benzodiazepines, IV fluids, and intubation and ventilator support.
Case 12. Case 12 inhaled toluene and presented with hypotension and pneumonitis. He received IV fluids, oxygen supplement, and antibiotics.
Clinical outcomes and complications of cases associated with substance abuse reported to the Ramathibodi Poison Center.

Clinical effects of severe and fatal elderly cases due to substance abuse reported to the Ramathibodi Poison Center during 2010–2017.

AKI: acute kidney injury; SVT: supraventricular tachycardia, ST: sinus tachycardia, PVC: premature ventricular contraction; HCF: healthcare facility.
All were admitted to ICU.
Treatment of severe and fatal elderly cases due to substance abuse reported to the Ramathibodi Poison Center during 2010–2017.

HCF: healthcare facility; ET: endotracheal tube; IV: intravenous; NaHCO3: sodium bicarbonate; ATB: antibiotic, BZD: benzodiazepine; HD: hemodialysis; NE: norepinephrine.
Discussion
This study describes substance abuse cases in older adults aged 60 years or older, who reported to a poison center. In our study, the incidence of substance abuse in Thai elderly individuals is 0.06 per 100,000 person-years (44 cases among 9.3 million Thai elderly population, in 8 years).4,12 The majority of the cases were male, which is consistent with previous studies.13–15 Most common exposed substance in Thai elderly was illicit substances including kratom, methamphetamines, opioids, and marijuana. Blow and Barry 5 reported the incidence of substance abuse in American elderly. The incidence in our study is lower, which may be due to underreporting, as drug use is often stigmatized in Thai culture.
In this study, there were 12 severe (27.3%) cases that were treated in ICU. Substances associated with severe and fatal outcomes were kratom, opioids, methamphetamines, and toluene. In a Brazilian study, alcohol (77%) was the most common substance associated with severe outcomes. 16 The common clinical effects in our population were somnolence and agitation. According to the reviewed literature, 5 the correlated clinical effects with substance use were neurological problems, cardiovascular disease (hypertension, hypotension, and arrhythmias), renal and respiratory failure, and psychobehavioral health problems, which is consistent with this study.
Five severe cases involved kratom, which is commonly seen in Southeast Asian countries. This substance is often used as a stimulant.17,18 Moderate to high doses of kratom have opioid-like effects. Clinical effects of kratom include agitation, hypertension, tachycardia, seizures, and opioid-like effects, such as drowsiness, respiratory distress, and coma.17,18
In this study, opioid subtypes related to severe outcomes were methadone, opium, and heroin. Opioid poisoning effects include the clinical triad of pinpoint pupils, central nervous system depression, and respiratory distress, as well as other effects including bradypnea, severe bradycardia, and hypotension. Specific treatment of opioid overdose is naloxone, an opioid antagonist. Even low doses of opioids in the elderly can lead to opioid poisoning due to pharmacokinetic or pharmacodynamics changes.
Most methamphetamine-overdose cases present with agitation, palpitations, and tachycardia, which is consistent with findings in this study.19,20 One common severe manifestation of methamphetamine toxicity is stroke. In this study, one individual developed venous sinus thrombosis, which corresponds with a study by Mendez-Sanchez. 21
Toluene, an aromatic hydrocarbon, is a colorless and volatile liquid at room temperature. Toluene inhalation results in respiratory symptoms, including bronchospasm, pneumonitis, and acute lung injury. 22 Central nervous system effects from toluene exposures were headache, ataxia, euphoria, and dizziness. Gastrointestinal effects include nausea, vomiting, and abdominal pain. According to our report, one case presented with hypotension and pneumonitis.
Limitation
As a retrospective study of poison center data, this study has some limitations, including incomplete data and selection bias. Due to nature of voluntary report data, the number of cases in poison center study can be underreported. Substance abuse cases who do not reach healthcare facilities may not be detected. The cases consulted to poison center may be more severe.
Conclusion
From a single poison center study, Thai elderly were mostly likely to be exposed to illicit substances including kratom, methamphetamines, opioids, and marijuana. Common clinical effects were somnolence, agitation, and dyspnea.
Footnotes
Acknowledgements
The authors would like to thank the staff members of the Ramathibodi Poison Center. The authors would like to thank Melissa Kerkelis, BS, The University of Queensland, for suggestions for the manuscript and language support.
Declaration of conflicts interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University (Approval Number: ID 01-61-30).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
As the study involved retrospective secondary analysis of existing collected data from routine care and further patient contact and reporting of identifying data was not required, exemption from requirement of informed consent was obtained from the Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University.