
Abstract
Objective:
The study examined the determinants of being hospitalized for pneumonia in a large cohort of drug users.
Methods:
Information of 4817 clients seeking treatment for illicit drug use was linked with the Finnish hospital discharge register to identify those who were hospitalized with main/primary diagnoses of pneumonia during 1997–2013. Cox regression models were used to examine the association between age, gender, homelessness, and route of drug administration of the primary drug at initial clinical consultation and pneumonia hospitalization. Findings were presented as adjusted hazard ratios and 95% confidence intervals.
Results:
There were 354 persons diagnosed with pneumonia, with a total of 522 hospitalizations at the end of 2013. The univariate Cox models revealed that being over 44 years of age, male gender, homelessness, and intravenous drug use at initial clinical consultation increased the risk of being hospitalized for pneumonia. In the fully adjusted multivariate model, being over 44 years was the strongest factor independently associated with pneumonia hospitalization (adjusted hazard ratio: 2.67, 95% confidence interval: 1.56–4.57, p < 0.001), followed by homelessness (adjusted hazard ratio: 1.75, 95% confidence interval: 1.38–2.22, p < 0.001) and intravenous drug use (adjusted hazard ratio: 1.27, 95% confidence interval: 1.01–1.59, p = 0.041). Of the 354 clients hospitalized for pneumonia, 31.9% (n = 113) were rehospitalized within 30 days of being discharged. One-third of the reasons for the 30-day rehospitalization were pneumonia-related.
Conclusion:
Vaccination, measures addressing housing instability, safe injecting and good hygienic practices, and treating underlying drug use problems could help to reduce morbidity for pneumonia in this cohort.
Introduction
Illicit drug use is a serious public health problem. According to recent global estimates by the United Nations Office on Drugs and Crime (UNODC), a quarter of a billion people or about 5% of the world population aged 15–64 years had used illicit drugs at least once in 2015, and 29.5 million of these users had drug use problems requiring treatment. 1 In the Nordic region, lifetime prevalence of illicit drug use among 15–64 year olds differs among countries, for example, cannabis use ranges from 36.5% in Denmark, 16.2% in Norway, 14.3% in Finland, and 12.5% in Sweden. 2 In Finland, estimates for other drugs included 1.1% for cocaine, 2.2% for amphetamines, 1.6% for ecstasy, and 1.1% for lysergic acid diethylamide. 2
Illicit drug use has been associated with adverse health consequences. 3 Pulmonary complications are commonly reported in drug users and these complications vary with the specific drug used, the route of administration, and the presence of adulterants.4–6 Pneumonia and tuberculosis were the leading pulmonary complications reported in the study by O’Donnell et al. 7 Other pulmonary complications commonly reported among drug users include cardiogenic and non-cardiogenic pulmonary oedema, excessive bronchial reactivity, emphysema, pulmonary arterial hypertension, pulmonary granulocytosis, and others. 5
Pneumonia is particularly important because it is the most common reason for hospitalization among drug users. 8 Incidence of pneumonia ranges from 4.4 to 14.2 per 1000 person-years for HIV-negative drug users and 47.8 to 90.5 per 1000 person-years for HIV-positive drug users. 8 In a study of 4236 former injecting drug users (IDU) in Italy, the overall incidence rate for pneumonia was 35.3 per 1000 person-years. 9 Pneumonia (especially community-acquired pneumonia) tends to be more frequent in drug users than in the absence of drug use. 5 Similarly, Hind 10 reported that the annual attack rate for pneumonia caused by Streptococcus pneumoniae was 21 per 1000 among IDU compared to 0.7–2.6 per 1000 for the general population.
Illicit drugs can affect all anatomical lung compartments to produce diverse immunological and morphological alterations. 11 These changes compromise local immunity and can predispose to lung consolidation, including infectious pneumonia and aspiration with secondary bacterial pneumonia. 12 Aspiration pneumonia often results from impairment of consciousness and alteration of gag reflexes which can occur with the use of heroin, cocaine, amphetamine, and possibly marijuana. Pulmonary infections result from impairment of alveolar macrophage function with secondary embolization of valve vegetation or infected thrombi. This can occur with heroin or cocaine use. 5 Similarly, opiate abuse is associated with interference with pathogen replication and alteration or suppression of the functionality of various cell types involved in both innate and adaptive immunity, resulting in increased susceptibility to infections, including pulmonary infections. 13 Ruiz et al. 8 also cited weakened immunity due to malnutrition and persistent antigenic stimulation as one of the factors that contribute to drug users’ increased susceptibility to pneumonia.
In the general population, S. pneumoniae is the most common pathogen for pneumonia, but other agents could be involved depending on the patient’s age and the clinical context. 14 Viruses also cause pneumonia in adults, but they constitute a greater burden in children. 14 In illicit drug users, infectious pneumonia can also be caused by bacteria and viruses. Common viral pneumonia pathogens include respiratory syncytial virus, influenza virus, adenovirus, and parainfluenza virus. Commonly isolated bacterial pneumonia pathogens include gram-positive cocci, gram-negative rods, and anaerobic bacteria in aspiration pneumonia. However, specific epidemiologic patterns vary across geographical regions.5,7,15 In addition, illicit drug use has been reported to be associated with higher risk for infection with resistant bacteria like community-acquired methicillin-resistant Staphylococcus aureus16,17 and greater severity of pneumonia resulting in higher rates of intensive care unit admission. 18
High rates of long-term morbidity, additional healthcare visits, and rehospitalizations have been reported in patients with pneumonia in the general population.19,20 This constitutes significant demand on healthcare resources and suggests a need for increased preventive strategies, discharge planning, and closer follow-up of patients.19,20 These measures are particularly important in drug users who tend to experience diverse forms of health problems. 3 Several factors have been associated with the likelihood of having pneumonia including older age, 21 being homeless, 22 intravenous drug use,10,23,24 inhalation of drug, 25 and having HIV infection.9,24,26 Understanding the determinants of pneumonia hospitalizations among drug users will form a basis for effective targeted control of pneumonia in this population.
Although many of the existing international studies on pneumonia were conducted using subjects drawn from general population, a few studies have focused exclusively on pneumonia among illicit drug-using populations.7,9,25 However, these few studies had limitations such as being a case report of only one illicit drug user, 25 and being too old and having short follow-up periods.7,9 In Finland, pneumonia morbidity among illicit drug users is less studied. Brander and Tukiainen 27 had previously published a research paper about a 24-year-old illicit drug (heroin) user hospitalized and treated for acute eosinophilic pneumonia. However, the study was a case report based on one single drug user and it is very old. More research studies possibly using a larger dataset are still needed. The main objective of this study was to assess the determinants of hospitalization for pneumonia in a cohort of treatment-seeking drug users in Finland during 1997–2013. The secondary objective was to describe rehospitalization that occurred within 30 days of being discharged for pneumonia during the same period.
Methods
Study design and population
The study population consisted of 4817 drug-using clients aged 11–65 years who sought drug treatment from the Helsinki Deaconess Institute (HDI) in Helsinki, Finland, between 31 January 1997 and 31 August 2008. Their primary drugs of abuse at baseline ranged from opiates (30%), stimulants (28%), cannabis (19%), alcohol (21%), prescription drugs (2%), and other drugs (1%). The proportion of any polydrug use (i.e. use of two or more drugs) was 91%. Structured clinical interviews were conducted at each client’s initial visit as part of routine procedures. The clinicians collected clients’ demographic information, self-reported history of drug use, and their social, medical, and psychiatric histories. For a more detailed description of data collection and the study population, see Onyeka et al. 28 Clients’ information was linked to the Finnish national hospital discharge register (FHDR) and the linkage was done using unique personal identifiers which are assigned to all residents of Finland. They were followed up from the first day of their first visit to 31 December 2013 to identify clients whose main/primary hospital discharge diagnosis was pneumonia. Finland has administrative health and social register system which has good coverage and validity. 29 The FHDR covers inpatient care provided at all hospitals and municipal health centres in Finland since 1969 and contains admission and discharge dates, discharge diagnoses (main/primary diagnosis and 1–3 additional/secondary diagnoses), personal identity codes, and other information. 30 In FHDR, diagnoses were recorded using the 10th version of the International Classification of Disease (ICD-10) codes. Only anonymized client data were released for this research.
Measurements
Pneumonia was described as ICD-10 codes J12–J18. The main outcome variable was pneumonia hospitalization (hospitalized vs censored). Predictor variables included baseline sociodemographic variables such as age (<45 years vs ≥45 years) and gender (male vs female); presence of immune suppressing condition such as HIV (yes vs no); conditions that lead to exposure to unsanitary conditions such as homelessness (yes vs no); and the route of administration of the primary drug (intravenous vs non-intravenous). We chose 45 years cut-off because the study by Woodhead et al. 31 revealed that community-acquired pneumonia tend to be more severe with increased mortality risk after 45 years. The secondary outcome was 30-day rehospitalization defined as rehospitalization that occurred within 30 days of being discharged for pneumonia. Reasons for rehospitalization were categorized as pneumonia-related (i.e. ICD-10 codes that fell within J12–J18) and unrelated to pneumonia (i.e. any other ICD-10 codes).
Statistical analysis
Statistical Package for the Social Sciences (SPSS) software version 21 for windows (IBM Corporation, Armonk, NY) was used for all analyses. Differences in baseline characteristics between those hospitalized for pneumonia versus the other clients in the cohort were assessed using chi-square test or Fisher’s exact test for categorical variables. Cox proportional hazards regression analysis was used to examine baseline variables that were associated with being hospitalized for pneumonia, first in univariate models and then in a multivariate model. Variables with p-value ≤0.05 in the univariate analyses were included in the multivariate model. Results were presented as hazard ratios (HRs) and adjusted hazard ratios (aHRs), and predictor variables with p-value ≤0.05 were considered statistically significant.
Ethical consideration
The research ethics committees of the Kuopio University Hospital and the Helsinki Deaconess Institute, the Ministry of Social Affairs and Health of Finland, and appropriate municipal authorities gave approval for the study.
Results
Differences in baseline characteristics
Differences in the baseline characteristics of the clients are presented in Table 1. Compared to the other clients in the cohort, those hospitalized for pneumonia had statistically significant higher proportions of persons aged 45 years and above (5.1% vs 2.2%, p = 0.001), and higher proportions of men (74.9% vs 69.5%, p = 0.033), homelessness (35.3% vs 21.0%, p < 0.001), and intravenous drug use (53.2% vs 44.7%, p = 0.003). Both groups were statistically similar in terms of their HIV status (p = 0.270).
Baseline characteristics of clients hospitalized for pneumonia versus other clients in a cohort of 4817 Finnish drug users followed up via register linkage during 1997–2013.

p-values: chi-square test or Fisher’s exact test.
Route of administration of the primary drug of abuse.
Pneumonia hospitalizations
Information from the hospital discharge register revealed that 354 persons had main/primary diagnoses of pneumonia at the end of 2013. As seen in Table 2, these 354 persons contributed a total of 522 hospitalizations, and the pneumonia hospitalization rate was 9.9 per 1000 person-years. The organisms that caused pneumonia were not specified for most of the hospitalizations – ICD-10 J18.9. However, for those whose causative organisms were specified, the numbers of pneumonia hospitalizations caused by viruses were far less common than those caused by bacteria.
Observed number of hospitalizations by ICD-10 diagnosis for the 354 Finnish drug users hospitalized for pneumonia during 1997–2013.
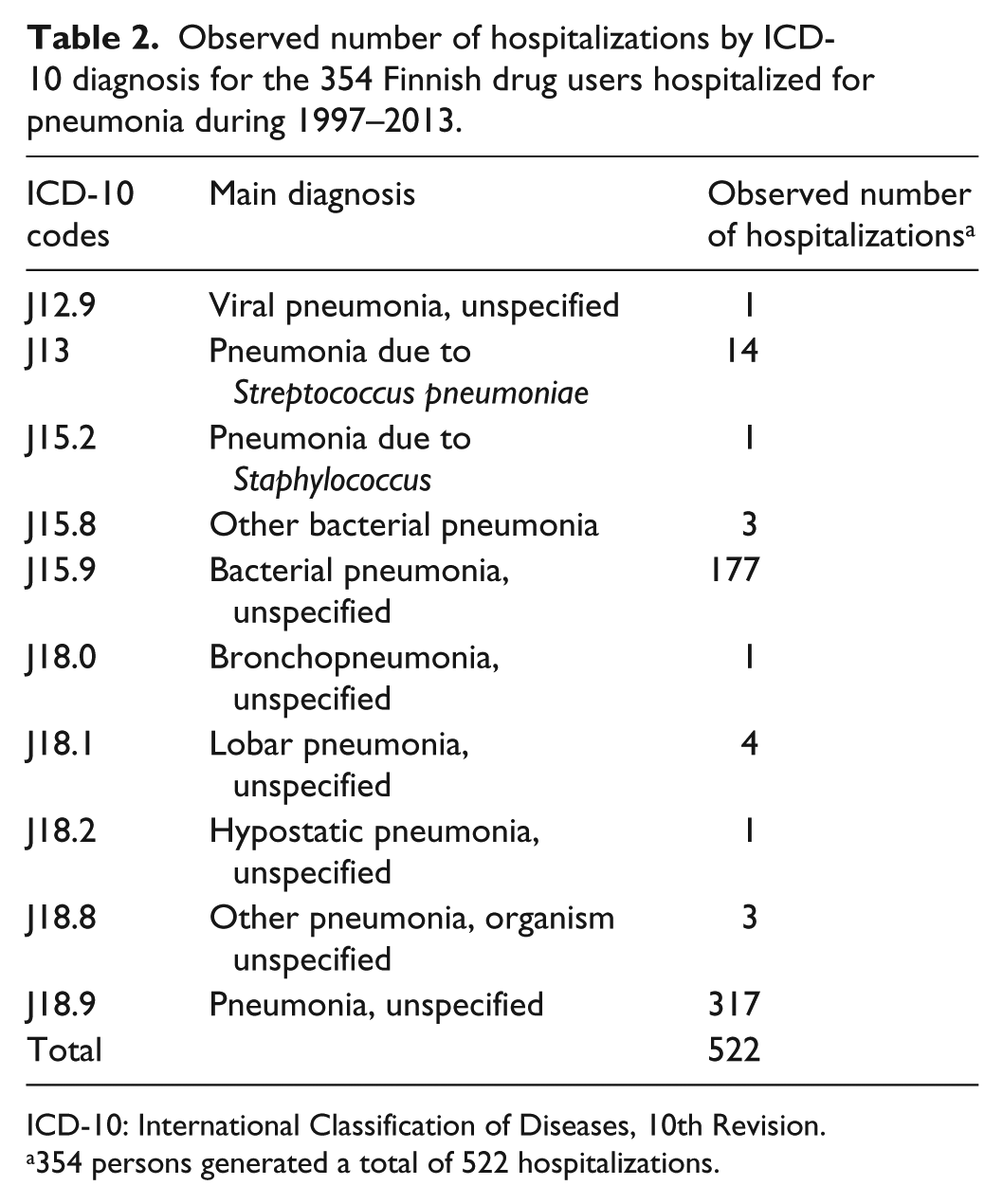
ICD-10: International Classification of Diseases, 10th Revision.
354 persons generated a total of 522 hospitalizations.
Determinants of pneumonia hospitalizations
The Cox regression analyses showing the association between baseline variables and being hospitalized for pneumonia are presented in Table 3. In the univariate models, being 45 years and older, male gender, homelessness, and intravenous use of the primary drug increased the risk of being hospitalized for pneumonia. In the full multivariate model, being 45 years and older was the strongest factor independently associated with pneumonia hospitalization (aHR: 2.67, 95% confidence interval (CI): 1.56–4.57, p < 0.001). Other factors associated with pneumonia hospitalization included being homeless (aHR: 1.75, 95% CI: 1.38–2.22, p < 0.001) and using primary drug intravenously (aHR: 1.27, 95% CI: 1.01–1.59, p = 0.041).
Determinants of pneumonia hospitalizations in a cohort of 4817 Finnish drug users followed up via register linkage during 1997–2013.
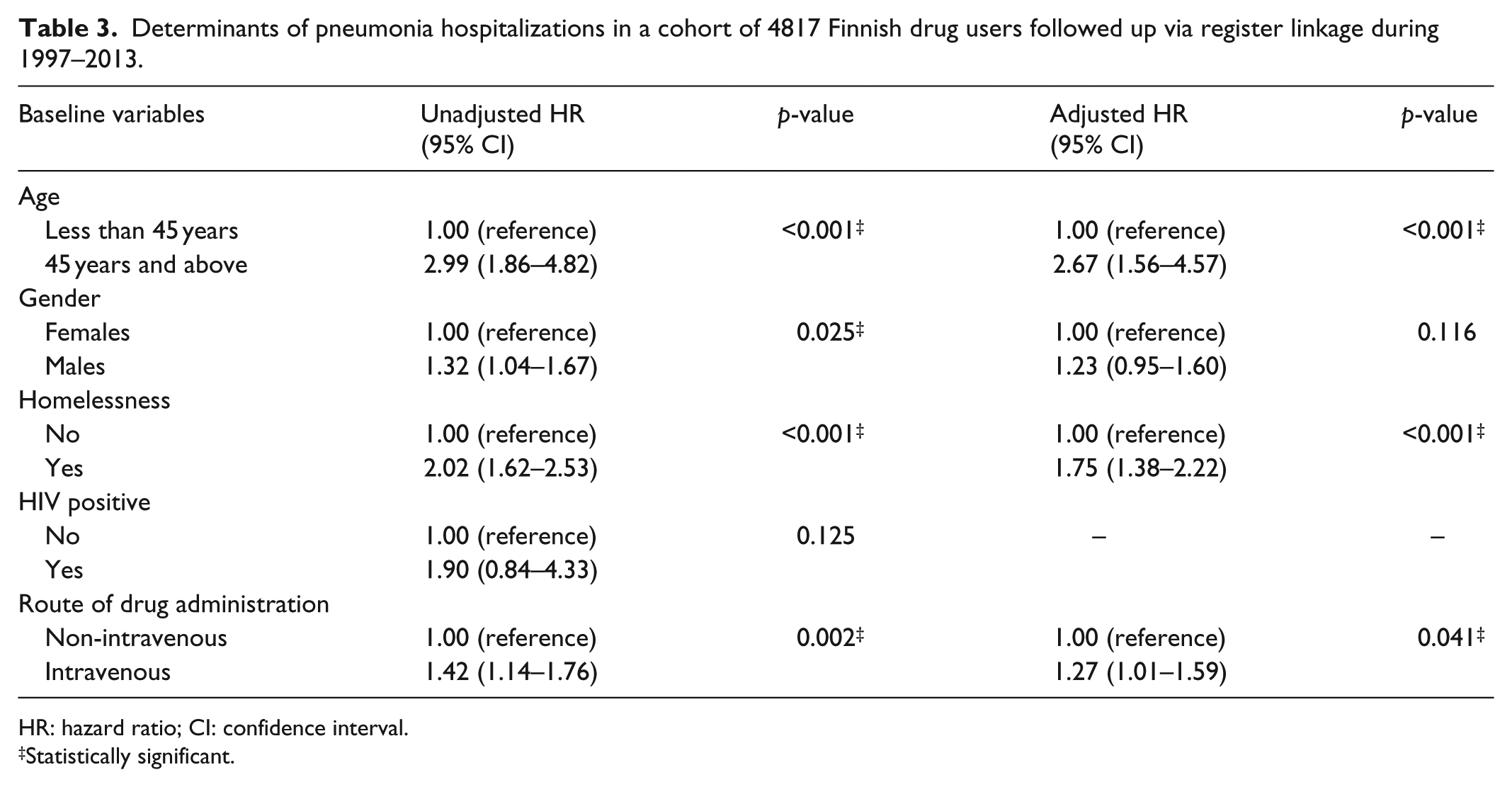
HR: hazard ratio; CI: confidence interval.
Statistically significant.
30-day rehospitalizations
Of the 354 persons who were hospitalized for pneumonia, 113 persons (31.9%, n = 113/354) were rehospitalized within 30 days of the initial discharge. These 113 rehospitalized persons accumulated a total of 154 rehospitalizations. The main diagnoses or reasons for rehospitalizations are presented in Table 4. Altogether 33.8% (52/154) were pneumonia-related. Mental and behavioural disorders were the predominant non-pneumonia-related reasons with a total of 41 rehospitalizations; 22 of them were mental and behavioural disorders due to psychoactive substance use and the remainders were schizophrenia and other types of mental disorders.
Reasons for 30-day rehospitalization in a subset of 113 Finnish drug users previously hospitalized for pneumonia during 1997–2013.

Of the 354 persons hospitalized for pneumonia, 113 persons (31.9%, n = 113/354) were rehospitalized within 30 days of the initial discharge. These 113 rehospitalized persons generated a total of 154 rehospitalizations.
Discussion
In this study, we assessed the determinants of hospitalization for pneumonia in a cohort of 4817 treatment-seeking illicit drug users in Finland during 1997–2013, and we described the rehospitalization that occurred within 30 days of being discharged from pneumonia hospitalization. We found that 354 persons were hospitalized with main/primary diagnoses of pneumonia during the follow-up period. Being 45 years and older, being homeless, and intravenous use of the primary drug were independently associated with pneumonia hospitalization. Our finding that age 45 years and above was associated with higher risk of hospitalization for pneumonia is consistent with results from a general population study which found that pneumonia increased with age. 21 Our finding might also be partly explained by age-related immunological changes that influence susceptibility to infection by S. pneumoniae 32 which further complicates the impaired immunity in illicit drug users. 13
Our result indicated that illicit drug users who are homeless were at higher risk of pneumonia hospitalization. This compares well with findings from previous studies. In a study of patients treated for pneumonia in Salt Lake City, USA, it was found that homeless patients had higher hospitalization risk than non-homeless patients. 22 In a different study in Toronto, Canada, Plevneshi et al. 23 found that homeless persons with invasive pneumococcal disease were more likely than others to be intravenous drug users.
In this study, those who consumed their drugs intravenously were at higher risk of being hospitalized for pneumonia. An older study reported that intravenous drug users have a significantly increased risk of community-acquired pneumonia. 10 More than 80% of the hospitalized patients in Madeddu et al.’s study were IDUs. 26 Although the exact mechanisms that lead to the increased prevalence of pulmonary infection in intravenous drug users are not completely understood, potential explanations include the use of contaminated drugs, needles, and syringes. Bacteria/pathogens introduced into the body through injection of contaminated drugs or through infections occurring at injection sites circulate to the lungs via the blood stream. The use of illicit drugs such as opiates depresses the normal coughing and sneezing reflexes and bacteria/pathogens introduced into the lungs through inhalation of foreign materials could cause aspiration pneumonia.4,33
Our results demonstrated that some of the drug users had multiple hospitalizations and a third of those rehospitalizations were pneumonia-related. These findings were consistent with previous studies that reported high rates of rehospitalization for pneumonia34,35 and suggested that a third of the rehospitalizations may be reduced by improved pneumonia management. The other reasons for rehospitalization were unrelated to pneumonia and may be reduced by recognizing and treating comorbidities in addition to managing drug use problems.
Major strengths of our study were the large sample size, long follow-up period and register linkage to obtain reliable information regarding hospitalization, and the availability of background information of the clients. The limitations of our study need to be acknowledged. This study was conducted using secondary data. Being a cohort of treatment-seeking drug users, our study findings may not be generalizable to non-treatment seekers. Due to the register-based nature of the follow-up, we did not have data for other known risk factors for pneumonia such as vaccination status, trauma or injury, taking immune-depressing medication, and other relevant information. However, despite these limitations, our study findings offer useful insight into pneumonia morbidity among drug users.
Conclusion
Our study revealed that 354 persons were hospitalized with main/primary diagnoses of pneumonia during the follow-up period. Being 45 years and older, being homeless, and intravenous use of the primary drug were independently associated with pneumonia hospitalization. Findings from this study suggest a need for measures to reduce morbidity for pneumonia in order to reduce healthcare resource utilization. This is pertinent because pneumonia is one of the most common reasons for hospitalization among drug users. 8 When the morbidity for pneumonia goes down, the need for hospitalization goes down, and human suffering caused by the sickness will also go down. Preventive measures targeting older drug users, injectors and homeless drug users are necessary to address increased risk of pneumonia hospitalizations in these subgroups. Vaccination with both influenza vaccine and polyvalent pneumococcal vaccine and counselling on maintaining good overall personal hygiene could reduce the risk of pneumonia infection in these subgroups. It is important to address the underlying drug use problems and to provide assistance to persons experiencing housing instability.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approvals were obtained from the Research Ethics Committee of the Kuopio University Hospital and the Ethics Committee of Helsinki Deaconess Institute. Permissions were obtained from the Ministry of Social Affairs and Health of Finland and from appropriate municipal authorities of all Greater Helsinki area communities where clients resided.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Academy of Finland (grant number 118584). We thank the staff members of the Helsinki Deaconess Institute for their collaboration and the data managers at the University of Eastern Finland.
Informed consent
Informed consent was not necessary because Finnish legislation permits the use of medical records (without personal identifiers) for medical and health research with permission from government/institutional authorities.