
Abstract
Objectives:
This study aims to assess (1) the difference in the prevalence of headaches, pain, and other associated symptoms between Gulf War I (1990–1991) and Post-Gulf War I (1992–2015) veterans who served as active military personnel in the Persian Gulf and (2) how the durations of deployment may affect the prevalence of those symptoms.
Methods:
With institutional human subject committee approval, veterans who were accepted to the Gulf War Registry at the VA San Diego Healthcare System between July 2013 and June 2015 (N = 367) were included in this retrospective chart review study and grouped according to the Gulf War period they served under or how long they were deployed to the Persian Gulf. Chi-square was used for categorical data analyses and analysis of variance was conducted for continuous outcomes. All analyses were two-tailed, where applicable, with α = 0.05 and Bonferroni for pairwise group comparisons.
Results:
Veterans who served during Post-Gulf War I or both Gulf War I and Post-Gulf War I exhibited more pain and neurological symptoms than Gulf War I veterans (p = 0.005, p = 0.003). In addition, veterans who served ⩾12 months reported more overall pain symptoms and analgesic use than those who served less time (p < 0.001, p = 0.024).
Conclusion:
The findings suggest that the length of deployment and Persian Gulf deployment period may play a role in acquiring headaches, pain, and other associated symptoms with increased analgesic consumption.
Introduction
Public concern for Persian Gulf veterans stems from the exhibited multitude of medical and psychiatric conditions and symptoms that manifest years following their return from the Persian Gulf (1990–present). In 1994, the Gulf War Registry (GWR) was nationally established in the Veteran Affairs Healthcare System to address these symptom complaints of veterans returning from deployment in the Persian Gulf region by providing support through treatment plans or service-connected benefits. 1 As part of the Registry enrollment process, a licensed physician reviews six major fields of symptoms associated with the health profile of a Persian Gulf veteran. These fields include neurological, gastrointestinal, respiratory, and dermatological problems, as well as pain and fatigue. 2
Even though there is an overall consensus categorizing and recognizing the first cohort of Persian Gulf veterans as Gulf War I (GWI) veterans (Operation Desert Shield: 1990–1991; Operation Desert Storm: 1991), a second cohort of Persian Gulf–deployed veterans (Post-GWI: Operation Iraqi Freedom: 2003–2010 and Operation New Dawn: 2010–2011) are often overlooked when investigating a cause for the multitude of health issues. 3 The attention disparity between these two eras of Persian Gulf veterans may have limited the understanding of the possible causes of the pain, fatigue, neurological, gastrointestinal, respiratory, and dermatological symptoms that affect millions of military personnel today.
Comparisons between the two eras are complicated by their distinct war profiles, illustrating the differences in healthcare approach when treating GWI versus Post-GWI veterans. In GWI, military personnel were exposed to environmental or chemical exposures, which has been a factor of interest in explaining the manifestation of the relevant symptomatology. Post-GWI veterans were not subject to the same environmental and chemical exposures but faced longer deployment durations, repeated deployments, and changes in enemy warfare tactics that incorporated improvised explosive devices (IEDs) and increased hostile fire.4,5 These factors are the basis for focused treatment of traumatic brain injuries and post-traumatic stress disorder (PTSD) in this population. Other notable differences between the two cohorts include an increased number of deployed troops and more women in the later Gulf War periods. 6 While numerous studies have been conducted to assess the role of environmental or chemical exposures in 1990–1991 Gulf War veterans and combat exposure in Post-GWI veterans, 7 few have investigated periods of war or the duration of Persian Gulf deployment for their impact on the development of the six fields of symptoms assessed during GWR enrollment.
To address the knowledge gaps in the current understanding of these multi-symptom complaints and to further provide validity for healthcare providers in managing this patient population, this study aims to assess the prevalence of pain, fatigue, neurological, gastrointestinal, respiratory, and dermatological issues by controlling for Persian Gulf deployment periods and duration of deployment in that region.
Methods
With institutional human subject committee approval, a list of veterans who had a documented GWR computerized medical record note between July 2013 and June 2015 was obtained from the Veteran Affairs San Diego Healthcare System (VASDHS) and included in the study. Informed consent was waived due to the nature of the study being a chart review. Data were then extracted from the veteran’s GWR medical note. The data categories included basic demographic information, dates of active duty in the Persian Gulf, documented health problems, active medication usage, as well as their Numerical Pain Rating Score (NPRS). The NPRS is the overall pain level (0–10) of the patient recorded by a healthcare professional. 8 Veterans were only enrolled in the GWR if they served specifically in the Persian Gulf region, thus excluding veterans who were deployed to Afghanistan during Operation Enduring Freedom from 2001 to 2014. Utilizing this electronic medical record note for the GWR, we could classify Gulf War veterans based on which deployment period they served under or how long they were deployed. Deployment periods were grouped as GWI, 1990–1991 (Group A), Post-GWI, 1992–2015 (Group B), and both war periods (Group C). Duration of deployment was grouped as less than or equal to 7 months (Group X), greater than 7 months and less than 12 months (Group Y), or greater than or equal to 12 months (Group Z). The durations of deployment were separated according to the average single tour length for military members (7 months).6,7,9
Symptom domains were based on the six fields of symptoms found in the GWR note in the computerized patient record system (CPRS). The six domains are as follows: fatigue, pain, neurological, gastrointestinal, respiratory, and dermatological symptoms.10,11 Pain and neurological symptom categories are further classified into three and five subfields, respectively. The symptoms were coded as either yes or no for each subject.
Total pain symptoms accounted for all available pain outcomes including any chronic pain conditions, joint pain, and muscle pain. The joint pain category alone included knee, ankle, shoulder, or wrist pain, while the muscle pain category alone encompassed leg, arm (away from joints), or back pain in either an acute (<3 months) or chronic (⩾3 months) condition. Chronic (⩾3 months) pain conditions included but were not limited to chronic joint and muscle pain conditions reported explicitly in the subject’s medical record. Total neurological symptoms were computed per subject from the total score of all available neurological outcomes (headache, memory and attention, mood, visual and hearing, and neurological sleep). The subcategory of mood included anxiety, depression, or other mood disorders, visual and hearing consisted of visual obstruction complaints and sensorineural hearing loss, and neurological sleep encompassed insomnia or hypersomnia.
The remaining four domains (fatigue, gastrointestinal, respiratory, and skin) did not include subfields. Fatigue symptoms included fatigue from chronic fatigue syndrome or fatigue from sleep apnea or insomnia. Constipation, diarrhea, abdominal pain, gastrointestinal esophageal reflux disease, and irritable bowel syndrome were all classified as gastrointestinal symptoms. Respiratory symptoms covered wheezing, coughing, asthma, bronchitis, and obstructive sleep apnea. Skin symptoms consisted of problems such as rashes, eczema, psoriasis and dermatitis. Documented diagnoses of PTSD based on a VA clinician’s assessment through the Clinician-Administered PTSD Scale for DSM-5 (CAPS) were also recorded and grouped. 12 For medication usage, documented use of analgesics included narcotic and non-narcotic pain medications, comprising but not limited to tricyclic antidepressants, anticonvulsants, triptans, non-steroidal anti-inflammatory drugs (NSAIDs), and selective serotonin reuptake inhibitors (SSRIs). These medications are documented by healthcare professionals and pharmacy technicians into CPRS for each veteran and were subsequently grouped by the research staff according to their drug classes for statistical analyses. The preliminary data were standardized for input into SPSS version 23.
Statistical analysis
These groups were compared using chi-square for categorical data and analysis of variance (ANOVA) for the continuous outcomes using SPSS version 23. All analyses were two-tailed, where applicable, with α < 0.05 and Bonferroni for pairwise group comparisons with the p-value adjusted in each domain. All data and variables were also analyzed for predictability using a logistic regression model. Subanalysis was conducted using chi-square or ANOVA to adjust for covariates including age, gender, race, ethnicity, PTSD, military branch, military occupational specialty (MOS), number of deployments, alcohol usage, and body mass index (BMI). All covariates could not be simultaneously adjusted under a chi-square model due to the small sample size, so these covariates were analyzed individually through stratification. Categorical covariates were coded as follows: gender as male or female; race as Caucasian, African-American, Asian, or other; ethnicity as Hispanic or non-Hispanic; PTSD as yes or no; military branch as the Navy, Marines, Army, or other; and military occupation specialty as combat or non-combat. The remaining covariates, which consist of age, number of deployments, alcohol usage, and BMI, were continuous variables analyzed using ANOVA. Alcohol usage was measured as the number of drinks consumed per day. Statistical tests were conducted to find significant differences in these covariates between groups. Where there were significant differences, the initial analyses on symptom and medication prevalence were repeated while adjusting for those covariates. In categories where there were an insufficient number of subjects to stratify by each group, the main analyses were repeated for the majority groups only. Subjects with missing data were excluded from that category for analysis.
Results
Part I: based on deployment period
Demographic information
Groups A, B, and C consisted of 164, 156, and 47 veterans, respectively. The overall gender difference between groups was significant (p < 0.01) with Group B (n = 27) having a significantly higher female population (p < 0.01) compared with Group A (n = 10). The age differences (mean (SD)) between groups were significant (p ⩽ 0.001) with Group B (40.6 (8.4)) being significantly younger in age compared with Group A (52.5 (7.0)) and Group C (51.9 (6.1)) (Table 1). The distribution between groups for ethnicity was significant overall (p < 0.05) with more Hispanic veterans in Group B (30.1%) compared to Group A (14.6%). The distribution of military branches was also significant between all groups (p < 0.001). In Group A, the majority of veterans were in the Marines (47.0%) followed by the Navy (32.9%) and Army (17.1%) branches. In Group B, most veterans were in the Navy (44.2%) and Marine (32.1%) branches with the fewest in the Army (19.9%). An even higher percentage of Group C identified as Navy veterans (68.1%) followed by a smaller percentage who identified as Marine (21.3%) or Army (6.4%) veterans. The effects of these covariates on symptom prevalence and medication usage are addressed and adjusted in Table 7. Average deployment duration (months) was significantly longer (p < 0.001) in Group C (35.7 (46.2)) than Group B (15.2 (13.3)) and Group A (8.0 (4.5)), with Group B also significantly longer (p < 0.001) than Group A. The number of deployments was significantly higher (p < 0.001) in Group C (2.9 (2.3)) than in Group B (1.6 (0.9)) and Group A (1.0 (0.1)), with Group B also significantly higher than Group A (p < 0.001). Deployment duration and number of deployments were found to be highly correlated (p < 0.001). There was no significant difference between groups in terms of race, MOS, BMI, or alcohol usage.
Demographic information of groups based on deployment periods.
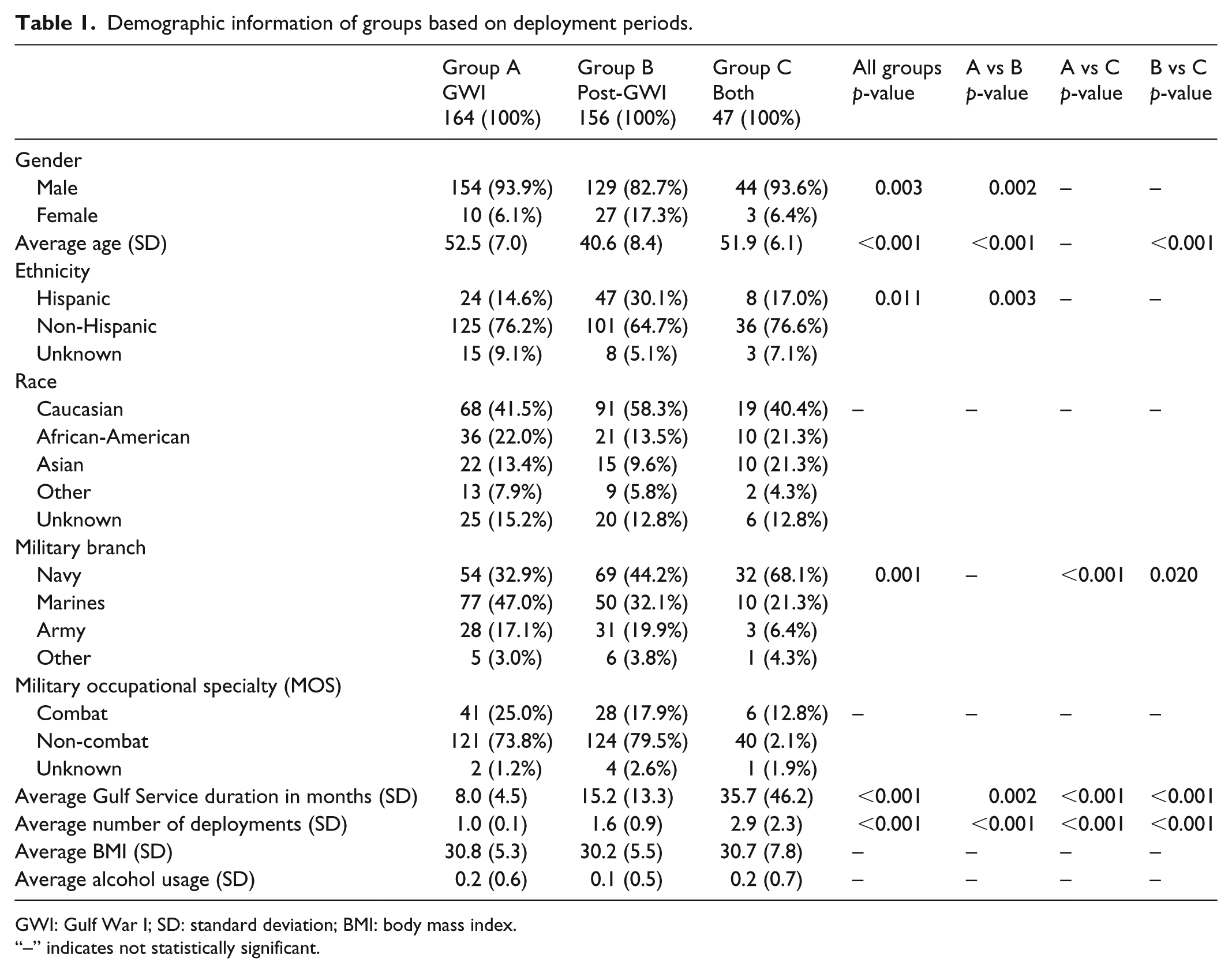
GWI: Gulf War I; SD: standard deviation; BMI: body mass index.
“–” indicates not statistically significant.
Deployment period and overall symptoms
The overall war period–based group comparison demonstrated a significant (p ⩽ 0.001) difference among the groups with both Group B (83.3%) and Group C (91.5%) showing significantly (p < 0.01) higher overall pain symptom prevalence than Group A (70.1%) (Table 2). Additional analyses in the joint pain category also resulted in a significant (p < 0.01) group difference with Groups A, B, and C demonstrating a prevalence of 47.6%, 60.9%, and 72.3%, respectively. Pair comparison in joint pain prevalence indicated that both Group B (60.9%) and Group C (72.3%) consisted of a significantly (p < 0.05 and p < 0.01, respectively) higher prevalence than Group A (47.6%). While both Groups B and C demonstrated an upward trend in overall chronic pain (p = 0.158 and p = 0.336, respectively) or muscle pain (p = 0.234 and p = 0.134, respectively) in comparison to Group A, the results were not statistically significant in either group or pair comparisons.
Symptoms of groups based on deployment periods.

GWI: Gulf War I; PTSD: post-traumatic stress disorder; NPRS: Numerical Pain Rating Score.
“–” indicates not statistically significant.
The overall group analyses in neurological symptoms demonstrated a significant (p < 0.05) difference among the groups with Group B (76.8%) showing a significantly higher prevalence than Group A (64.0%) in the pair comparison. In addition, Group B showed significantly (p < 0.05) higher prevalence in both headache (44.2%) and mood (44.2%) complaints than Group A (32.9% and 31.7%, respectively). While no overall group prevalence difference was detected, compared to a 46.2% prevalence in Group B, a significantly (p < 0.05) higher distribution of Group C (63.8%) experienced fatigue symptoms. The remaining three domains of symptoms (gastrointestinal, skin, and respiratory) did not yield statistically significant differences in either overall group or pair comparisons.
When observing for PTSD, a significant (p < 0.05) group difference was noted with Group B (42.3%) showing a significantly (p < 0.05) higher prevalence of PTSD diagnosis than Group A (28.7%). There were no significant differences among the groups in their overall NPRS reported at GWR visits.
An analysis under the regression model yielded similar results, with pain symptoms serving as a predictor of the war period served. Those who suffered from overall pain symptoms were most likely to be in Group B (p = 0.006) or in Group C (p = 0.006). Joint pain also predicted war period, with Group B (p = 0.017) and Group C (p = 0.003) having the strongest associations. No additional associations were found using the regression model in this category.
Medications
No significant differences were found in overall group or pair comparisons for specific medication usage based on war periods (Table 3). Additional analyses conducted using the logistic regression model also did not show any significant findings.
Medication usage of groups based on deployment periods.

GWI: Gulf War I; NSAID: non-steroidal anti-inflammatory drug; SSRI: selective serotonin reuptake inhibitor; GI: gastrointestinal.
“–” indicates not statistically significant.
Part II: based on durations of deployment
Demographic information
Groups X, Y, and Z consisted of 141, 55, and 171 veterans, respectively. The overall average age (mean (SD)) differences among groups were significant (p < 0.05) with Group X (49.0 (9.1)) being significantly older in age than Group Z (45.9 (9.4)) (Table 4) in the pair comparison. No other statistically significant differences between groups in ethnicity, race, military branch, MOS, BMI, or alcohol usage were found.
Demographic information of groups based on duration of deployment.

SD: standard deviation; BMI: body mass index.
“–” indicates not statistically significant.
Deployment duration and overall symptoms
The overall deployment duration–based group comparisons demonstrated a significantly (p ⩽ 0.001) higher overall pain symptom prevalence in Group Z (86.5%) in comparison to Group X (68.8%). Additional analyses for other chronic pain conditions and muscle pain demonstrated a significant (p < 0.05) difference with Group Z having a higher prevalence (70.2% and 62.6%) than Group X (58.7% and 49.3%) in both categories of pain. However, no statistical difference was detected in either group or pair comparisons for the joint pain category. Likewise, no significant differences were found in neurological symptoms among the three groups (Table 5).
Symptoms of groups based on duration of deployment.

GWI: Gulf War I; PTSD: post-traumatic stress disorder; NPRS: Numerical Pain Rating Score.
“–” indicates not statistically significant.
Overall, a significant (p < 0.01) group difference was found in veterans who exhibited half or more of the six fields of symptoms with Group Y (61.8%) having significantly (p < 0.01) higher prevalence of a majority of symptom categories than Group X (53.6%) in the pair comparison (Table 5). There were no statistically significant differences in the prevalence of PTSD in either the overall group or paired comparisons. In addition, there were no significant differences between groups in their overall NPRS reported at the GWR-related visits.
Results under the logistic regression model reiterated the association between certain symptoms and duration of deployment. For example, veterans who suffered from overall pain symptoms were most likely to be in Group Z (p = 0.000). The development of muscle pain also predicted the duration of deployment, with Group Z (p = 0.019) having the strongest association with that symptom. A diagnosis of at least three out of six fields of Gulf War illness symptoms served as another strong predictor of a deployment duration greater than or equal to 12 months, or Group Z (p = 0.002). No additional associations were found using the regression model in this category.
Medications
Group Z (46.8%) demonstrated a significantly (p < 0.05) higher prevalence of analgesic use compared to Group X (34.1%) (Table 6). In the analgesic subset NSAIDs, there was an overall significantly (p < 0.05) higher usage in Group Z (37.4%) in comparison with Group X (21.0%). For the remaining categories of medication use, there were no significant differences for both the overall and pair comparisons.
Medications of groups based on duration of deployment.

NSAID: non-steroidal anti-inflammatory drug; SSRI: selective serotonin reuptake inhibitor; GI: gastrointestinal.
“–” indicates not statistically significant.
Under the regression model, NSAID usage was a strong predictor of deployment duration served, with those who take NSAIDs most likely to be in Group Z (p = 0.002). There were no additional findings for associations between the remaining medications and deployment duration.
Part III: adjusting for covariates
Deployment period and overall adjusted symptoms
The analysis was repeated after significant differences in gender, PTSD, military branch, and ethnicity were found between war period groups. Significant differences in gender were identified by adjusting the analyses to males only. Out of the 14 significant differences in symptom prevalence in the original analyses found in Table 2, 11 findings remained significant, while 4 were no longer significant. The comparisons that lost significance include neurological symptoms overall, headache between Groups A and B, neurological sleep overall, and fatigue between Groups B and C. The pairwise comparison between Groups B and C for PTSD was not previously significant, but became significant after adjusting gender with more male veterans in Group B having PTSD compared to Group C (p < 0.05).
When adjusting the comparisons between war periods by removing veterans who were diagnosed with PTSD from the main analyses, 4 out of the original 14 significant differences were no longer significant. These include neurological symptoms overall, joint pain between Groups A and B, headache between Groups A and B, and fatigue between Groups B and C.
When adjusting for military branch, only three categories of symptoms were found to have significant differences when looking between the Navy, Marines, and Army branches. There was a significant difference in joint pain prevalence in the Marines (p < 0.05) and Army branches (p < 0.05) but not the Navy branch. On the contrary, fatigue (p < 0.05) and respiratory (p < 0.05) symptom prevalence were significant in the Navy branch, but not Marine or Army.
Since ethnicity was significantly different between Groups A, B, and C, the analyses were repeated to adjust for this covariate. Two separate analyses were conducted to adjust for ethnicity: one for the Hispanic population and one for the non-Hispanic population. In both analyses, pain symptoms overall (p < 0.05) was significantly different between groups. Significantly more non-Hispanic veterans in Group B were also diagnosed with PTSD than in Group A (p < 0.05) and Group C (p < 0.05) (Table 7).
Adjusted symptoms of groups based on deployment periods.

PTSD: post-traumatic stress disorder; GWI: Gulf War I; NPRS: Numerical Pain Rating Score.
“–” indicates not statistically significant.
p < 0.05; **p < 0.01.
Adjusted medications
When adjusting for the gender difference by removing the female population, Group C was more likely than Group A to take medications for dermatological symptoms (p < 0.05). When adjusting for the PTSD difference by removing the population with PTSD, there was a significant difference overall in triptan usage (p < 0.05). Specifically, significantly more veterans in Group B were more likely to take triptans compared to those in Group C (p > 0.01). While these two results were significant, the small effect size due to a sample size of 11 subjects in these categories suggests that a larger sample may be required to fully appreciate the statistical power (Table 8).
Adjusted medication usage of groups based on deployment periods.
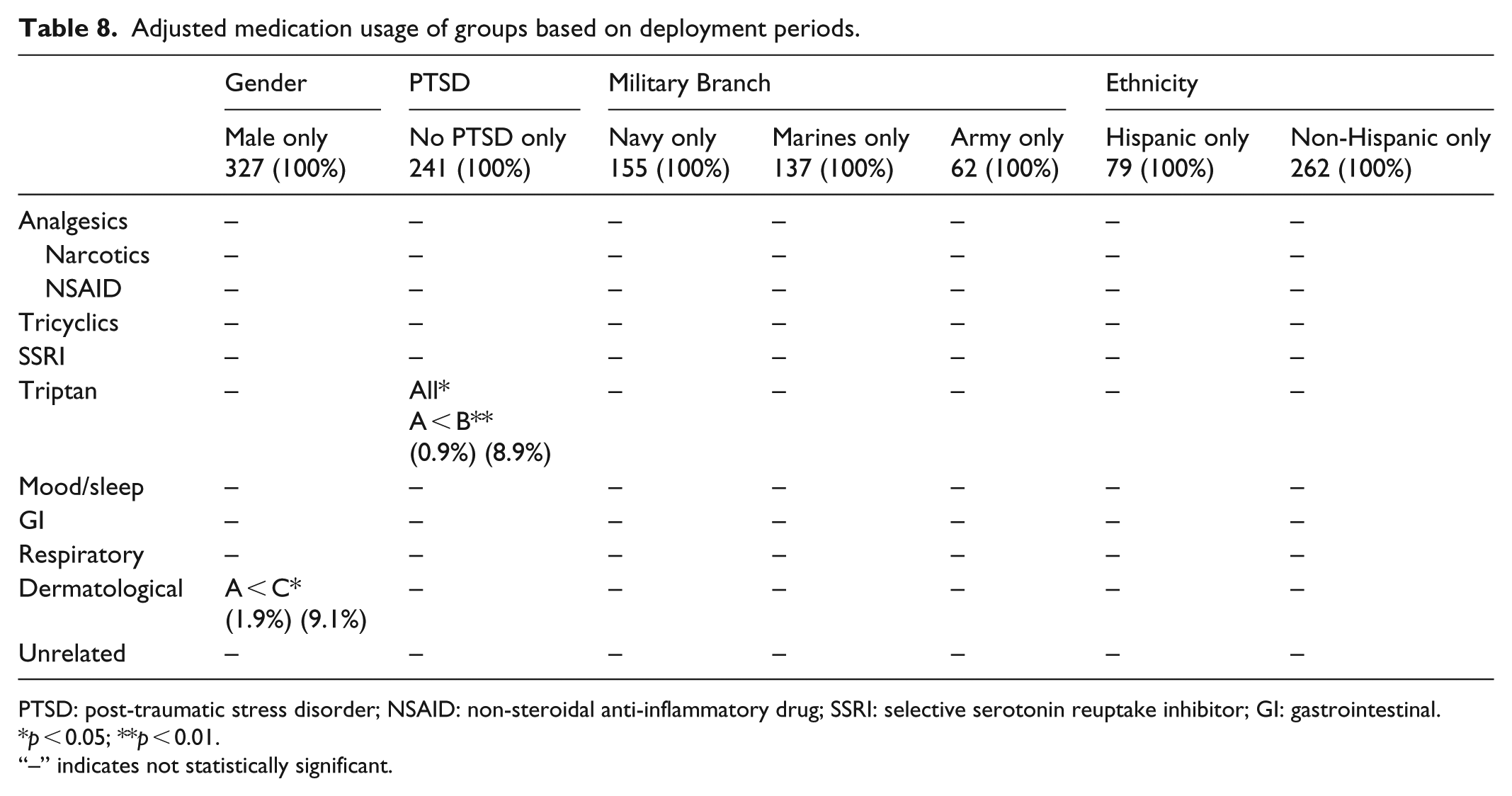
PTSD: post-traumatic stress disorder; NSAID: non-steroidal anti-inflammatory drug; SSRI: selective serotonin reuptake inhibitor; GI: gastrointestinal.
p < 0.05; **p < 0.01.
“–” indicates not statistically significant.
Deployment duration and adjusted symptoms and medications
The analyses were not repeated for the groups based on deployment duration because there were no significant differences between groups in gender, ethnicity, race, military branch, MOS, BMI, alcohol usage, or PTSD.
Discussion
While the six fields of symptom complaints continue to be a major health issue for military personnel who have served in and returned from the Persian Gulf, current understanding in the causalities of this health profile still is not well defined. While some studies have suggested that certain environmental or chemical exposures may play a role in the development of the six fields of symptoms assessed in the GWR, none of these findings have established a definitive causal relationship for the illness.13–20 Therefore, other relevant and important factors including the period of war and duration of deployment, which can theoretically contribute to the development of pain, fatigue, neurological, gastrointestinal, respiratory, and dermatological issues should be assessed.
The results of this preliminary study suggest that veterans who have served in the region during and after GWI experience more headaches, pain, and other associated symptoms than their counterparts who served only in the GWI period. While the association between Post-GWI and pain symptoms was confirmed with additional analysis under the regression model, the relationship could have been due to the duration of deployment differences between the two Gulf War periods. Therefore, in this study, the second analysis was conducted to assess how the duration of deployment in the Persian Gulf affects the prevalence of those symptoms. The results indicate that veterans serving ⩾12 months overseas experienced more overall pain symptoms, analgesic (NSAIDs) usage, and overall symptoms than those who served ⩽7 months in the same region. Regression analysis further validated the relationship between longer deployment duration and overall pain symptoms with NSAID usage. This is a unique finding, as previous studies have not addressed how the overall length of service may in fact contribute to the symptom expression. Those who served in Post-GWI were also more likely to be diagnosed with PTSD than GWI veterans, which may have been due to the increased use of IEDs and hostile fire that defined this Persian Gulf deployment period. These lines of information can be valuable for both correlating with their relevant environmental or chemical exposure and determining how long a military member should serve in the region to decrease the likelihood of increased health complications.
In addition to the deployment duration, there are other covariates that could have contributed to the differing prevalence of symptoms between veterans of GWI, Post-GWI, or both wars. Possible covariates that may account for the significantly higher symptom prevalence in Post-GWI veterans could be due to age, gender, ethnicity, race, branch of service, combat or non-combat roles, level of alcohol usage, PTSD prevalence, BMI, deployment duration, and number of deployments. When the subjects were grouped based on war period, the groups differed in age, gender, PTSD levels, ethnicity, military branch, deployment duration, and number of deployments, which could have contributed to the prevalence numbers reported. However, after adjusting for those covariates, the majority of the findings still held true. Although education level was not available in the GWR medical notes for analysis, it is another possible covariate that could account for the results seen. Future studies with access to these records would help corroborate the findings by analyzing education levels between veterans in different Persian Gulf deployment periods.
The notable differences that could be confounding the data include those due to gender, PTSD, or military branch. After adjusting for gender, the prevalence comparisons suggest that there may be a gender effect in neurological symptoms such as headaches and sleep issues, as seen by the loss of significance after removing the female population. On the contrary, the female population from Post-GWI may be disproportionately affected in terms of neurological symptoms compared to their male counterparts. While this finding may be due to the psychological consequences of a hostile war, it can also be because there are fewer GWI females applying for the GWR. An increased sample size may resolve these differences. In subsequent analyses, PTSD is shown to affect joint pain and headache prevalence in Post-GWI veterans, while service branch is associated more with joint pain or respiratory issues compared to other branches. Overall, the differences in prevalence numbers caused by covariate adjustment suggest that symptom prevalence could be associated with underlying comorbid conditions or occupational hazards. However, the stratified analysis was performed using only a fraction of the entire study population, so the adjusted results may have been caused by a smaller number of samples rather than PTSD or military branch. In all cases, further studies including a larger population would more definitively address these concerns.
The average age differed between Groups A, B, and C, but age adjustments were not conducted because there were little to no medical records from GWI veterans dated 10 years ago that would have been needed to conduct a comparison. Post-GWI veterans applying for the GWR were on average 12 years younger than GWI veterans, but the symptoms in the study were extracted from the GWR medical note during the same 2-year period between 2013 and 2015. A comparison of older health records from GWI veterans with current health records of Post-GWI veterans would remove the possibility of symptom prevalence due to age differences. However, these older records were not readily available for comparison since only a small number of GWI veterans were enrolled and evaluated in the VASDHS immediately following their return from deployment. Interestingly, previous studies also suggest that increased age is highly correlated with pain, and older adults are more likely to report pain symptoms than younger adults.21,22 The results from this study show the opposite, with the younger veterans of Post-GWI being more likely to experience pain than the older veterans of GWI. As a result, age adjustment was not performed.
Since deployment duration and number of deployments also differed between groups, with Post-GWI veterans serving longer than GWI veterans, a secondary adjusted analysis based on duration was conducted to ascertain the differences in symptom prevalence. Since the number of deployments was highly correlated with the deployment durations, no additional adjusted secondary analyses were required. When veterans were grouped based on duration, there were no significant differences between the groups in gender, race, ethnicity, military branch, MOS, BMI, alcohol usage, or PTSD levels. However, the analyses showed that those who served longer than 12 months were more likely to experience pain than those who served fewer than 7 months. This suggests that deployment duration may be a factor in the development of pain symptoms in addition to the war period served. This is an important finding as previous studies have primarily focused on the impact of chemical, environmental, or combat exposure on the development of pain and other associated symptoms. Since deployment duration is a common factor between all wars in all time periods and locations, more emphasis should be placed on duration as a possible indicator for veterans’ health. Additional studies on deployment duration while adjusting for all other covariates would help in corroborating these findings and providing further evidence to influence military policy.
Furthermore, in defining the study population, war period for GWI is clearly defined in the current literature, but no clear definition has been provided for subsequent deployments to the same region. This impacts the ability for future researchers to effectively compare the patient populations. In fact, most studies focused solely on GWI, refraining from mentioning a following war period.10,23,24 Other studies have made no distinction between Gulf War I Desert Shield/Desert Storm and Post-Gulf War I Operation Enduring Freedom/Operation Iraqi Freedom and therefore termed it the “Gulf War era.”25,26 Finally, some avoided the classification all together and compared based on the military operation name, which may have overlooked the environmental exposures that both operations had in common based on their deployment to the Persian Gulf.3,27,28 Our study specifically classifies the war periods as GWI (1990–1991) and Post-GWI (1992–2015). In the absence of any prior classification, this study made specific distinctions on deployment periods and where they were deployed for the ease of data grouping and analyses. In the future, a scientific community consensus would be useful for the research topic as a whole.
A weakness in the current study lies in the sample size being 367 and obtained solely from a single VA healthcare facility, affecting its external validity. The results are not representative of GWI or Post-GWI veterans as a whole because the VASDHS is more likely to enroll veterans who are from the Navy or Marine branches of the military due to the number of bases located in San Diego County. Recruitment of additional Army veterans into future analyses would be a more accurate reflection on the two cohorts of veterans deployed to the Persian Gulf. However, the result of this study does serve as a stepping stone for future studies in assessing these avenues of causal relationship in the development of the six fields of symptoms associated with deployment to the Persian Gulf. Expanding to other VA or military healthcare facilities and increasing the sample size for data extraction would be useful in ensuring a more accurate proportion of each military branch with respect to their operation, increasing statistical power, and corroborating the results obtained already. Furthermore, including a control group of veterans who did not serve in the Persian Gulf during either GWI or Post-GWI but had served a similar duration nonetheless would narrow down the causality of location-specific factors that could contribute to the symptoms expressed. Since the listed symptoms were extracted solely from the GWR medical note of those who participated in the GWR application process, there is a possibility that those prevalence numbers are conflated or biased as those who applied for the GWR may be more likely to experience health complications than those who did not apply. The addition of a second control group of veterans who served in the Persian Gulf War but did not apply for the GWR would help reveal the true prevalence of symptoms in Gulf War veterans as a whole.
Additional limitations to the study include bias due to self-reported symptoms at a medical visit occurring decades after the return from deployment. Veteran enrollment into the GWR has gained traction in the more recent years. The pattern of registration is multifactorial but may be connected to media attention, veterans’ symptom severity, or increasing knowledge about the Registry’s existence. In the period following GWI, there was increased media attention surrounding the possible exposures in the Persian Gulf, highlighting similarities between these current exposures to Agent Orange during the Vietnam War that affected thousands of American veterans. The headlines may have caused an increase in veteran symptom reporting to the Veteran Affairs Healthcare System. In the process of influencing veterans to enroll, the media attention may have led to recall bias in which veterans are more likely to report symptoms that they are reminded of, rather than the symptoms they actually have. However, it is possible that their symptoms were caused by other health conditions or personal events within the period of time after the war but preceding the GWR visit. In addition, veterans who enrolled in the GWR at its inception may not be similar to veterans who enrolled during the period of data collection (2013–2015) for this study. GWI veterans who signed up for the Registry could have had more severe symptoms, prompting them to document their exposures as quickly as possible, whereas those who enrolled later may have done so because their symptom severity was more manageable. Therefore, the time between deployment and enrollment into the Registry can have an effect when determining the homogeneity of veterans’ profiles during their grouping for the study. While media attention and symptom severity are conceivable biases that have an effect on the results of the study, these biases are actively limited by the standard of practice held by the Veteran Affairs Healthcare System during symptom reporting at the GWR visit and the time frame in which data were collected during the study. The symptoms found in the computerized medical record system are often chronic, well documented, and assessed for validity by physicians during the enrollment visit, which would remove the possibility of false reporting. In addition, the data for this study were extracted from veterans who enrolled in the GWR between 2013 and 2015, so the difference in symptom severity between 1990–1991 GWI veterans who enrolled in 2013 may not be significantly more severe than those who enrolled in 2015. However, deployments for Post-GWI occurred between 1992 and 2015, so symptom severity, which can be represented by the time between deployment and enrollment, plays a stronger role in assessing the homogeneity between veterans of this cohort. An additional study with a larger sample size than provided by this study that focuses solely on Post-GWI veterans and the manifestations of their symptoms in relation to years since deployment would properly address the homogeneity of this group. Finally, the spike in enrollment to the Registry may have been caused by an accumulation of national recognition through word of mouth, website postings, or hospital advocacy, similar to marketing advertisements that gain traction over time.
In short, this single-sited study suggests that veterans who served in the later deployment periods and those with longer durations of service in the Persian Gulf War region may be more likely to suffer from headaches, pain, and other associated symptoms with increased analgesic usage. Additional studies are required to further investigate the aforementioned relevant issues.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Human Subjects (IRB), Research Safety (SRS) and R&D with study ID: H160094.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the VA Rehabilitation and Research Development SPIRE Award and Department of Defense Congressionally Directed Medical Research Program Grant.
Guarantor
A.L. is the guarantor of this study.
Informed consent
Informed consent was waived for this study as it was a record review study. No intervention was given or patient interaction was conducted.
Trial registration
Trial registration is not applicable for this study because of being a record review.