
Abstract
Objectives:
The Gulf War Registry monitors related health conditions of veterans returning from the Persian Gulf Region. Enrollment consists of two phases: Phase I—veterans meet with their local VA Environmental Health Coordinator and complete the self-reported Gulf War Phase I Worksheet (VA Form 10-9009A). Phase II involves a physical exam, medical history review, and laboratory test analysis conducted by a licensed physician. The providers’ documentations are frequently referred for exposure assessment and benefit claim. We conducted an initial comparison assessment to ascertain any potential disparity in exposure reporting between the applicants in Phase I and the providers in Phase II.
Methods:
With institutional human subject committee approval, a list of veterans with a Gulf War Registry electronic medical note from the VA San Diego Healthcare System (2013–2015) was obtained. Comparing Phase I with Phase II reports allows three distinct reporting group combinations for each of the 21 exposure categories. Group I: both the patients and the healthcare personnel provided the same report for the respective exposure. Group II: healthcare personnel but not the patients reported the exposure. Group III: only the patients but not the healthcare personnel reported the exposure.
Results:
A total of 178 (of 367) subjects had both the medical note from the healthcare provider and a physical copy of their Phase I Worksheet available, and therefore were eligible to be included in the overall one-way and subsequent pair-wise chi-square analyses. The results indicate that Group I reporting pattern had a significantly (p < 0.01) lower prevalence in nine exposure categories compared to Group III.
Conclusion:
The findings suggest that the medical documentation from the healthcare providers does not consistently and accurately reflect the patients’ report in near 50% (9/21) of assessed exposure categories. Potential remedies addressing this exposure reporting disparity, such as a standardized template or electronic upload, are further discussed.
Introduction
The Gulf War Registry was nationally established in 1994 to monitor the health conditions of the veterans returning from the Persian Gulf Region and provides medical justification for policy that may have significant impact on their entitlement of healthcare benefits. 1 Veterans who previously served in the Persian Gulf War region between 1990 and the present day are eligible to apply to the Gulf War Registry through the Environmental Health and Benefits and Enrollments Office at any Veteran Affairs Hospital site. More importantly, the medical documentation provided by the healthcare personnel in the electronic medical record systems relevant to the registry often serves as a database for investigations in assessing the cause of neurological or other illness-related symptoms, such as fibromyalgia, chronic headaches of unknown etiology, irritable bowel syndrome, and chronic fatigue due to environmental or chemical exposures. 2
Enrollment into the Gulf War Registry consists of two phases. Phase I is the screening appointment in which the Gulf War veteran meets with their local VA Environmental Health Coordinator and has their completed self-reported Gulf War Phase I Worksheet (VA Form 10-9009A) evaluated. During this phase, environmental exposures are discussed and documented into the Gulf War Registry, then relevant laboratory tests are ordered. Only government officials with appropriate security clearance are permitted to access the Gulf War Registry. Phase II is scheduled approximately 3 weeks after the screening appointment and involves a physical exam, medical history review, and laboratory test analysis conducted by a licensed physician to determine eligibility for the Gulf War Registry. At the conclusion of the interview, the physician records the visit in the electronic medical record system, which is then locally accessible to other healthcare professionals. Phase I and Phase II reports are linked using the patient’s name and social security number to ensure accuracy. The Veteran Benefits Administration reviews the Gulf War Registry reports and supporting documentation to determine service-connected benefits. This process is the standard national procedure for enrollment into the Gulf War Registry. 3
Findings during the Phase II visit with healthcare providers are documented in the Computerized Patient Record System (CPRS) which serves as the official medical record for the veterans’ health conditions. 4 To this date, numerous studies have relied on information extracted from the CPRS in assessing the causality nature of the exposures to the documented symptomatology.5,6 However, the CPRS system across all the VA facilities handling the registry visits lacks a uniform approach and medical record template. This trend of provider preferred formats of documentation in the CPRS could potentially lead to a significant problem in the accuracy of the medical record and result in a significant confounding factor for investigations aiming to assess the causal effect of environmental or chemical exposure in the development of illnesses. Currently, no study has been conducted to assess whether the information documented in the CRPS accurately reflects the exposure information collected from the patient in Phase I. Here, we conducted an initial comparison assessment to ascertain any potential disparity in exposure reporting between registry participants and the healthcare providers.
Methods
With institutional human subject committee approval, a list of veterans participating in the Gulf War Registry at the Veteran Affairs San Diego Healthcare System (VASDHS) from July 2013 to June 2015 was obtained. These veterans visited VASDHS for the registry process but did not necessarily reside within San Diego. Only 178 (out of 367) subjects had both the medical note and a physical copy of their self-reported intake worksheet reviewed by the Environmental Health Coordinator available. Demographic information was also extracted from the CPRS for this population and is shown in Table 1. Those who did not qualify for the Gulf War Registry, due to not being deployed to the Persian Gulf or having a service duration in the Persian Gulf prior to 1990, were not included in the 367-subject pool. Furthermore, there were no hard-copy records available for review prior to 2013 or for 189 of the 367 subjects. The eligible 178 subjects were then included in the subsequent evaluation steps.
Veteran demographics.

Coding of exposure from patient reports
The standardized Gulf War Phase I Worksheet (VA Form 10-9009A) details 21 different environmental and chemical exposure categories (see Tables 3 and 4). Each of the exposure categories allows the patient to circle “Yes,” “No,” or “Unknown.” In some cases, the patient may have missed the question and therefore it would be coded as “Skipped.” “Unknown” and “Skipped” have been coded together in analysis.
Coding of exposure information reported by healthcare providers
The Gulf War Registry medical note is submitted through the CPRS by the physicians conducting the Phase II physical exam. Among the patients’ health record and lab results, the physicians are to report possible Gulf War exposures. The providers either reported the exposure categories by manually typing the information in a standardized Gulf War template or they did not report them. Therefore, for each exposure category, either “Yes” or “No” was coded.
Coding of patients’ and healthcare providers’ exposure reporting discrepancy
Comparing Phase I (patient) with Phase II (healthcare providers) reports allows three distinct reporting pattern group combinations between patients and healthcare providers for each exposure category. Group I consisted of accurately reported cases in which both the patients and the physicians provided the same report for the respective exposure category. Group II contained cases in which only the physicians but not the patients reported the exposure in one or more exposure categories. Group III comprised cases in which only the patients but not the physicians reported the exposure (see Table 2).
Grouping criterion based on patient and physician reporting response.

Data analysis
Frequency counts were obtained for each exposure item on both the Gulf War Phase I Worksheet and the CPRS Gulf War Registry Note. After coding and classifying the reporting of each exposure item into the three groups, the data were then analyzed using overall one-way main and then subsequent pair-wise chi-square comparisons with SPSS Version 23 (see Figure 1).
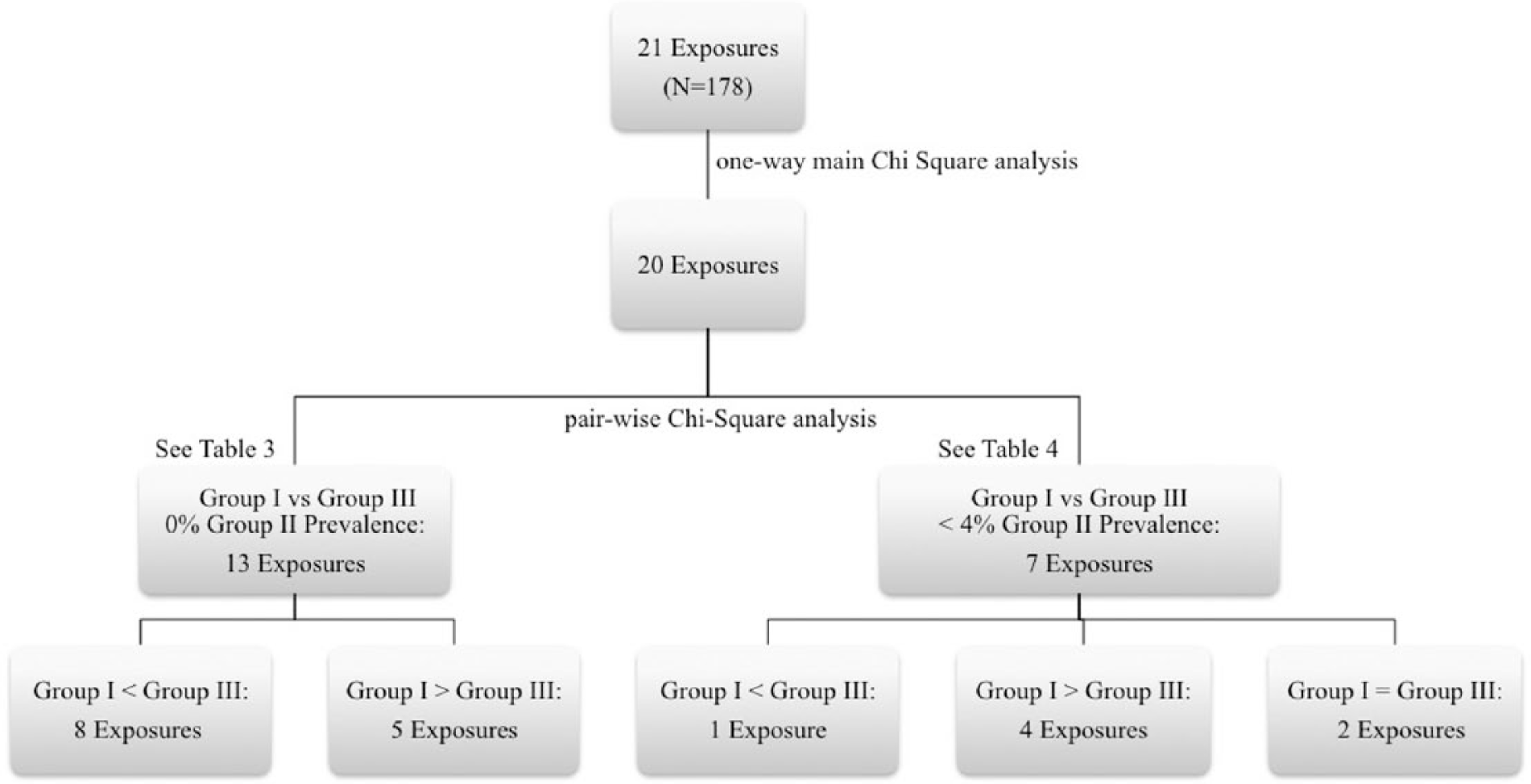
Data analysis flow chart.
Results
A total of 178 (out of 367) patients’ records were selected for group coding in each exposure category. With the exception of “bathed in water other than provided by armed forces,” all 20 exposure categories demonstrated significant (p < 0.01) differences in the overall one-way main chi-square analysis among all three groups of reporting pattern combinations (see Tables 3 and 4). Since Group II reporting pattern overall demonstrated zero prevalence in 13 categories within the main analyses, subsequent pair-wise comparisons were only conducted between Group I and III reporting patterns in these categories. The results indicate that Group I consisted of a significantly (p < 0.01) lower reporting pattern prevalence in eight exposure categories: cigarette smoke (11.2% vs 88.8%), diesel fumes (9.6% vs 90.4%), burning trash (30.9% vs 69.1%), skin exposure to diesel (24.2% vs 75.8%), paints (29.2% vs 70.8%), personal pesticide use (41.0% vs 59%), food other than provided by armed forces (24.7% vs75.3%), and immunization against anthrax (21.3% vs78.7%) in comparison with the Group III reporting pattern. However, a higher reporting prevalence of Group I was noted in the remaining five exposure categories: pyridostigmine (60.1% vs 39.9%), mustard gas (88.2% vs 11.8 %), contaminated food (61.2% vs 38.8%), bathed in contaminated water (65.7% vs 34.3%), and immunization against botulism (70.2% vs 29.8%) in comparison with the Group III reporting pattern (see Table 3).
Exposure categories with 0% Group II prevalence.

– Ineligible for subsequent analysis.
Low accuracy: significantly low prevalence of Group I in comparison with Group III; high accuracy: significantly high prevalence of Group I in comparison with Group III.
Exposure categories with small Group III prevalence.

Low accuracy: significantly low prevalence of Group I in comparison with Group III; high accuracy: significantly high prevalence of Group I in comparison with Group III.
Similarly, very low percentages of prevalence were found in Group II reporting pattern within the remaining seven exposure categories: smoke from oil fires, smoke from fumes, Chemical Agent Resistant Coating (CARC), microwaves, uranium, nerve gas, and other exposures at 2.8%, 3.9%, 2.2%, 0.6%, 0.6%, and 0.6%, respectively (see Table 4). Subsequent paired chi-square comparisons were only conducted between Group I and Group III and demonstrated a significantly (p < 0.01) higher reporting prevalence for Group I in four out of seven exposure categories: CARC (64.6% vs 33.1%), uranium (73.6% vs 25.8%), nerve gas (82.0% vs 17.4%), and other exposures (68.0% vs 31.5%) categories, but a lower reporting pattern prevalence in smoke from oil (38.2% vs 59.0%), and no difference in microwave and smoke of fumes in comparison with Group III.
Therefore, overall Groups I and III are found to be the main exposure reporting patterns among patients and healthcare providers while the Group II reporting pattern is highly uncommon. More importantly, the current case study suggests that Group I reporting pattern is significantly lower in nine (exposure to diesel, burning trash, skin exposure to diesel, paints, personal pesticide use, food other than provided by armed forces, immunization against anthrax, cigarette and smoke from oil fires), but higher in eight (pyridostigmine, mustard gas, bathed in contaminated water, immunization against botulism, CARC, uranium, nerve gas and other) exposure categories in comparison with Group III reporting pattern. These findings highly suggest that the medical documentation from the physicians does not consistently and accurately reflect the patients’ report in close to 50% (9/21) of assessed exposure categories.
Discussion
According to the results of this comparison study, numerous exposure categories (close to 50%) are underreported in the physicians’ Gulf War Registry report. Furthermore, less than 4% of exposure categories for each subject were overreported. These discrepancies could be explained by the absence of a standardized medical record template with exposure categories matching VA Form 10-9009A for the providers to complete during Phase II of the registration process. A possible solution would be for the self-reported documentation to be either uploaded to the patients’ medical record or completed by the patient on a secure network in order to have a reliable electronic reference. In this format, the patient’s documentation, which would still be reviewed for accuracy and completion by the VA Environmental Health Coordinator, could be added with ease to both their medical record and the Gulf War Registry. This would ensure that the self-reported information would be consistent across databases. Another solution is to match healthcare providers’ visit template in the CPRS with the patients’ intake survey form so that the providers can verify any self-reported exposure categories including the “unknown” or “skipped” exposure items with the patients.
The requirement of the physical copies of the patients’ intake forms for comparison limited the sample size of this study. Increasing the sample size by incorporating other VA locations would help ascertain the scope of the inconsistencies across different VA facilities handling the Gulf War Registry. In addition, patients who are applying for the Gulf War Registry may be suspected of over-reporting exposure categories for benefit purposes, however not only are they asked to support their claim with physical and anecdotal evidence, the official Gulf War Registry website states that entitlement to benefits is dependent on certain health diagnoses and not solely exposure reporting. These checking measures decrease the likelihood of false reporting; however, the matter of accuracy between patient and healthcare provider reports still exists.
Overall, this study suggests that there are discrepancies between healthcare provider documentation and patient reporting in the history of environmental and chemical exposures related to deployments in the Persian Gulf Region. These inconsistencies may affect the patient’s entitlement to their benefits as well as the epidemiological understanding of their health problems with regard to their exposure history. Finding a viable solution for minimizing reporting discrepancies can streamline the verifying process as well as help veterans along the way.
Footnotes
Acknowledgements
Trial registration is not applicable because of it being a record review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Human Subjects (IRB), Research Safety (SRS) and R&D with study ID: H160094.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the VA Rehabilitation and Research Development SPIRE Award and Department of Defense Congressionally Directed Medical Research Program Grant.
Informed consent
Informed consent was not sought for this study because it was a record review study. No intervention was given or patient interaction was conducted.