
Abstract
Background:
Intravenous thrombolysis is one of few evidence-based treatments for acute stroke. Treatment uptake is low outside major stroke care centres. There is a need for greater understanding of barriers encountered by clinicians when seeking to increase thrombolysis rates.
Aim:
The aim of this study is to describe physicians’ and nurses’ perceptions regarding thrombolysis for acute stroke at hospitals in the earlier stages of thrombolysis implementation.
Methods:
A cross-sectional paper survey completed by physicians’ and nurses’ was distributed to 1127 staff at stroke care units, emergency departments or equivalent stroke care facilities at 19 Australian hospitals, as part of a cluster randomised controlled trial for thrombolysis implementation and systems improvement.
Results:
Of 1127 potential participants, 503 (148 physicians and 355 nurses) completed surveys (45% response rate). Over 90% agreed that thrombolysis improved the odds of independent survival. However, 42% to 58% agreed that there were limitations in the evidence base. A small proportion of staff indicated deficits in technical competencies. Interactive or competency-based training was reported by less than two-thirds of the sample. Challenges such as quick bed availability were identified. Emergency department physicians were less positive towards the treatment compared with nurses (p < 0.001), stroke care unit physicians were more positive than nurses (p = 0.047) and older clinicians were more positive than younger clinicians (p = 0.007).
Conclusion:
Australian hospitals seeking to address barriers to stroke thrombolysis implementation may benefit from the availability of interactive and competency-based training, staff performance feedback, support to make beds available quickly and bypass arrangements to quickly deliver acute stroke patients to appropriate facilities.
Introduction
Every year, 15 million people worldwide have a stroke, leaving 5 million people with a permanent disability. 1 In 2012, 6.7 million people worldwide died from stroke. 2 In Australia, stroke is a leading cause of long-term adult disability 3 with around 12,000 stroke deaths recorded in 2012. 4 In the United States, there are 795,000 strokes every year. 5 Ischaemic stroke is estimated to cost $140,048 over a lifetime with projections of direct medical stroke-related costs increasing from US$71.6 billion in 2012 to US$184.1 billion in 2030. 6 In the United Kingdom, there are 100,000 strokes every year with 40,000 people dying from their stroke and 65% of survivors leaving the hospital with a disability. 7 The annual National Health System and social care cost for stroke in the United Kingdom is around £1.7 billion. 7 The majority of stroke cases are admitted to hospital 8 with more than 35,000 stroke hospitalisations recorded in Australia in 2009 to 2010. 9 Intravenous (IV) tissue plasminogen activator (tPA) treatment administered to eligible ischaemic stroke patients within 4.5 h of onset is one of few evidence-based treatments for stroke in the acute phase.1,10
Appropriately administered thrombolysis treatment has proven to be cost-effective.11,12 The benefits of stroke thrombolysis treatment within 4.5 h of stroke onset have been endorsed by the United Kingdom’s Commission on Human Medicines, 13 and tPA is supported by national and international guidelines.14–18 The Model of Resource Utilization, Costs and Outcomes for Stroke study reports savings of 155 disability adjusted life-years 12 in a group of 256 eligible stroke patients, with an Australian study reporting savings of 0.02 life-years and 0.04 quality-adjusted life-years per person over a 1-year time period post treatment. 19 Despite its benefits, tPA administration rates remain relatively low: 20 3.4% in the United States, 21 11.4% in the United Kingdom 22 and 7% in Australia. 22
Several barriers to the implementation of thrombolysis for acute stroke have been identified in the literature.23–26 Pre-hospital barriers include lack of community knowledge about stroke, stroke sufferers calling a primary care physician (rather than ambulance), mode of transport to hospital, failure to seek help urgently, 27 and admission to a non-academic hospital. 28 Bunch et al. 29 reported that the main barrier to tPA treatment for in-hospital strokes is the delay in stroke recognition by staff. A systematic review by Kwan et al. 23 highlights inefficient processes for emergency stroke care and delays in obtaining treatment consent. At a hospital level, increasing the use of IV tPA treatment is possible 30 but requires multiple practice changes. Grol and Wensing’s 31 theoretical model underpinned the survey.
The Individual health care provider factors are a significant determinant of low tPA treatment rates. 23 A common barrier is the inappropriate triage of patients by emergency and ambulance.23–25 Physicians’ uncertainty of the impact and administration of thrombolysis, familiarity with and motivation to adhere to recommended guidelines, are barriers to treatment uptake. 26 Scott et al. 32 report that characteristics associated with favourable clinician attitudes towards tPA included non-emergency medicine board certification, older age and a smaller hospital environment. Several studies reveal inefficient in-hospital processes for managing emergency stroke patients,23,24 lack of appropriate infrastructure, staffing and hospital capacity. 24 The National Stroke Audit Report 2017 found that 25% of stroke patients do not have access to thrombolysis and 75% had an established stroke care unit (SCU). 33 Cadilhac et al. 34 reported that SCU access varied significantly in Australia with 3% access reported in rural areas versus 77% in metropolitan areas.
While existing data provide an indication of barriers faced by hospitals, a more focussed perspective and targeted efforts are needed to improve tPA use. This study primarily aims to explore barriers and facilitators to change among Australian hospitals in their early stages of stroke thrombolysis implementation, and to explore the association between the proportion of patients thrombolysed at each hospital and the attitude of staff towards IV stroke thrombolysis.
The primary aim of this study is to:
(a) Describe physicians’ and nurses’ perceptions regarding key barriers and facilitators to increased tPA use within their hospital.
The secondary aims of this study are to:
(b) Describe characteristics associated with positive attitudes towards tPA treatment.
(c) Assess the association between the actual proportion of patients thrombolysed at each hospital and average staff score on staff attitude towards tPA treatment.
Method
The study was approved by Human Research Ethics Committees in New South Wales, Victoria and Queensland. Implied consent was obtained from each participant by reading the Information Statement accompanying the staff survey and then completing and submitting the anonymous survey.
Study design
A cross-sectional survey was used to assess staff attitudes, personal characteristics and hospital characteristics associated with stroke thrombolysis. 35
Participants
The survey was distributed to staff involved in either assessment or treatment of potential stroke patients at 19 Australian hospitals enrolled in a cluster randomised controlled trial. 36 Metropolitan, regional, public and private hospitals in their early stages of stroke thrombolysis, with an ED (emergency department) and an SCU or equivalent capacity, were eligible to participate. All selected hospitals met the requirements for providing thrombolysis (trained staff, clinical facilities), and all but one had already provided thrombolysis treatment to stroke patients. Hospitals were selected from National Stroke Foundation audit records and state-based clinical SCU networks. Eligible staff were physicians and nurses who worked in the SCU, the ED or equivalent capacities and were rostered to work during the 1-month survey period.
Procedure
Prior to survey distribution, agreement was reached with the site coordinator regarding which staff were eligible to participate based on providing either assessment of potential stroke, further assessment of suspected stroke patients or delivery of thrombolysis. The anonymous pen-and-paper survey was distributed in 2012 to 2013 prior to implementation of the trial intervention. It was distributed by a stroke clinician or stroke nurse at each hospital. A record was kept regarding the estimated number of eligible staff (e.g. emergency and stroke unit doctors and nurses rostered to work during the survey month), surveys distributed and surveys returned. The timing of the data collection was dependent on staff availability to distribute and collect surveys for 1 month during a 12-month window (mid-2012 to mid-2013).
Measures
Staff survey
Surveys were modified from a previous survey developed by Grady et al. for ED staff 37 and pilot-tested for readability, clarity and comprehensiveness of survey items by a team of behavioural researchers (n = 5), stroke clinicians (n = 2), ED physicians (n = 2) and stroke nurses (n = 2) at the University of Newcastle and Hunter New England Local Health District. The survey assessed thrombolysis practices, hospital characteristics, personal characteristics, individual provider context, social professional context and health system context.
Attitudinal items were developed from literature regarding knowledge implementation 31 and a prior survey.35,37 Respondents were asked to rate agreement with a series of statements. Participants were asked to rate their level of agreement with each survey item using a four-point scale of ‘strongly disagree’, ‘disagree’, ‘agree’ and ‘strongly agree’ with a ‘not applicable’ option. Three versions were created allowing tailoring of items to the roles of SCU physicians, ED physicians and nurses.
The Individual health care provider context involved skills and experiences, including five items common to all providers, two nurse-only items and seven physician-only items, and attitudes towards thrombolysis. The Professional social context included leader opinions and practices and the presence of innovators, and workplace culture. The Health system context addressed hospital-level policies and practices.
In addition, Personal characteristics included principal role, gender, age group and years of experience in emergency and/or stroke care.
Survey scoring
The categories of strongly agree/agree were collapsed for all scoring as were the strongly disagree/disagree categories. Where an item was positively framed, responses of ‘strongly agree’ or ‘agree’ were given a score of 1 and all remaining responses a score of 0. Reverse scoring was used for negatively framed items. ‘Not applicable’ responses were excluded from the analysis. Domain scores were calculated for the domains of individual provider context, social context and health system context. Eight attitudinal items were used to create an attitude score by summing the number of positive responses. A higher score indicated a more positive attitude towards tPA. Factor analysis and internal consistency of the survey items were calculated and are reported in the results.
Hospital-level data
Categorisation of hospitals as metropolitan versus non-metropolitan was based on the classification used by available online health department information.
Statistical methods
Participant characteristics (profession specific and combined) are presented as frequencies and percentages for categorical variables, and means and standard deviations for continuous variables.
The primary aim is to descriptive statistics including frequencies and proportions were produced to desribe physicians’ and nurses’ perceptions regarding key barriers and facilitators to increased use of tPA within their hospital. The secondary aims re as follows. (a) Multivariable linear regression was used to explore characteristics associated with attitudinal items (within the individual provider context) towards tPA treatment. Coefficient estimates are presented with 95% Wald confidence intervals (CIs). The p values resulting from F tests are also presented for each variable in the model. No variable selection methods were used. Referent categories for the nominal variables are listed in the tables. (b) To assess the association between the proportion of patients receiving thrombolysis at each hospital and the average staff attitude score towards tPA treatment, case data were obtained from the study database and hospital International Classification of Diseases-10 reports over the baseline data collection period, to determine what proportion of stroke patients received thrombolysis at each hospital.
All statistical analyses used SAS, version 9.4 (SAS Institute, Cary, NC, USA). All participant responses were included in the analyses regardless of whether they agreed with the clinical evidence regarding thrombolysis in order to retain a complete picture of the perceptions of all relevant staff. We estimated for the worst-case scenario regarding prevalence of any one item being 50%, a sample size of 384 would give a precision of ±5% with an alpha = 0.05.
Results
Response rate and participant characteristics
A total of 503 out of 1127 potential participants from 19 hospitals completed the surveys (45% response rate). The response rate was 67% for SCU physicians (85/126), 32% for ED physicians (63/194) and 44% for nurses (355/807). Hospital response rates varied from 16% to 100% (Table 1). The sample contained both metropolitan and regional hospitals.
Participant characteristics.
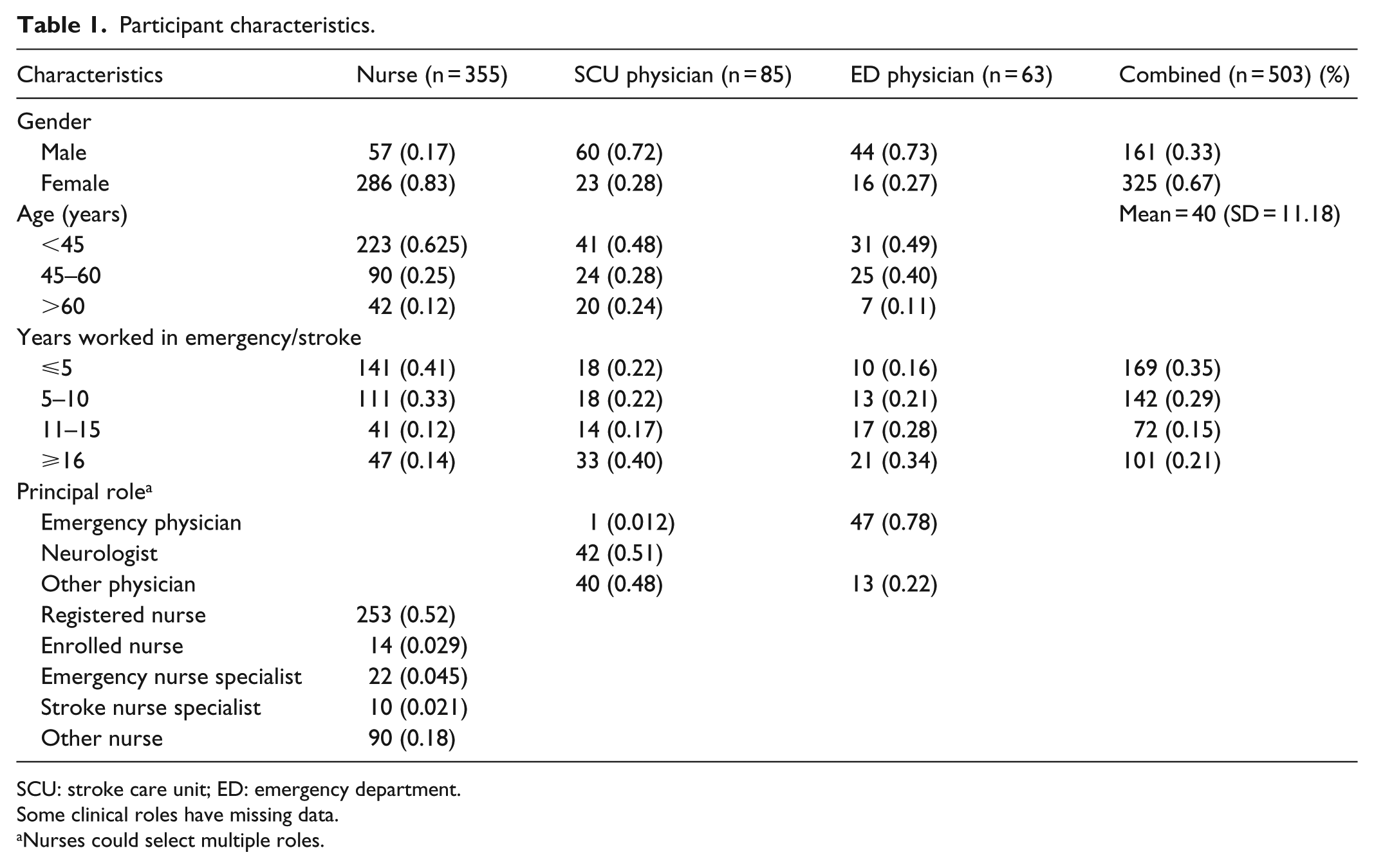
SCU: stroke care unit; ED: emergency department.
Some clinical roles have missing data.
Nurses could select multiple roles.
Perceptions regarding individual, professional and health system contexts
Individual health care provider context and attitudes to acute stroke care
Physicians’ and nurses’ reported skills and experiences are listed in Table 2, including nurse-specific and physician-specific items. The mean domain score for the common items was 8.08 (SD = 2.43, maximum score 13) for nurses and 8.75 (SD = 2.58, maximum score 13) for physicians.
Individual health care provider context and attitudes to acute stroke care.

tPA: tissue plasminogen activator.
Number of respondents who completed that item.
Refers to difficulties using the data extracted from the Safe Implementation of Thrombolysis in Stroke tool for monitoring thrombolysis care outcomes.
Reverse scoring.
Professional social context
Responses relating to the professional context are listed in Table 3. The mean score for the common items was 12.21 (SD = 3.53, maximum score 17) for nurses and 13.03 (SD = 3.79, maximum score 17) for physicians.
Professional social context.

tPA: tissue plasminogen activator.
Number of respondents who completed that item.
Physician only item.
Health system context
Responses to the health system items are listed in Table 4. The mean score for the common items was 10.50 (SD = 2.59, maximum score 12) for nurses and 9.29 (SD = 2.39, maximum score 12) for physicians.
Health system context.
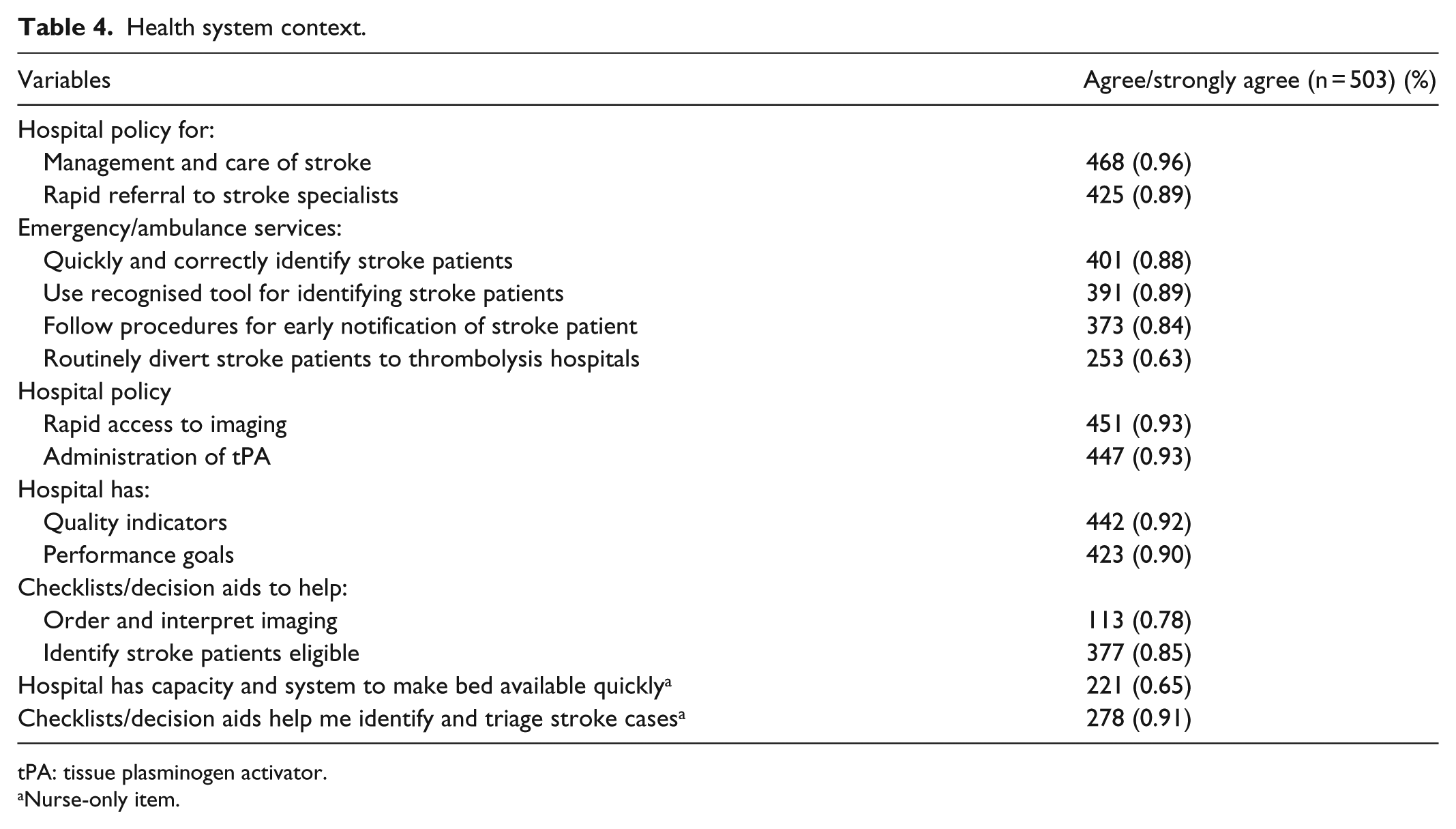
tPA: tissue plasminogen activator.
Nurse-only item.
Personal and hospital characteristics associated with attitude score
A multivariable linear regression was used to identify whether participant and hospital characteristics were associated with attitude score for the 191 participants with complete data on all survey items. This model explained 25% of the variation. The internal consistency of the eight items constituting the attitude score was acceptable (Cronbach’s α = 0.7). An exploratory factor analysis (principal factor method) using only these items found evidence for only one domain (eigenvalues for the factors were <1) and the items in the domain explained 93% of the variance of that domain. ED physicians reported a significantly less positive attitude towards tPA treatment than nurses (coefficient = –1.6, 95% CI = (−2.3, −1.0)), whereas SCU physicians reported a slightly more positive attitude than nurses (coefficient = 0.59, 95% CI = (0.01, 1.18)). Older clinicians were slightly more positive in attitude towards tPA treatment (coefficient = 0.03, 95% CI = (0.01, 0.06)). All other predictors were non-significant (see Table 5). A multivariable linear regression including SCU and ED physicians indicated that physicians who reported a higher proportion of patients being treated with tPA also had a slightly (although non-significant) more positive attitude towards tPA treatment (coefficient = 0.73, 95% CI = (−0.074, 1.53), p = 0.075) than other physicians.
Attitude scores.

CI: confidence interval; ED: emergency department; SCU: stroke care unit.
Multivariable linear regression with attitude score as the outcome including variables common to all staff types as predictors (n = 191, R2 = 25.3%).
The p values are from F tests assessing reduction in error sums of squares due to adding variable to the model that includes all other variables.
Correlation between the actual proportion of patients thrombolysed and staff attitude towards tPA treatment
At baseline, one of the hospitals had a zero thrombolysis rate, eight hospitals had rates between 0% and 4%, eight hospitals had rates between 4% and 10% and two hospitals had rates between 10% and 15% of stroke cases. A non-significant positive correlation (Spearman = 0.117, p = 0.64; Pearson = –0.09, p > 0.05) was found between the actual proportion of patients thrombolysed and staff attitudes towards thrombolysis (see Figure 1, Supplementary Material).
Discussion
Although stroke thrombolysis has been an approved and guideline-recommended treatment for eligible ischaemic stroke patients in Australia since 2003, thrombolysis rates remain low. This study provides some insights regarding in-hospital staff-related reasons as to why Intra Venous Thrombolysis rates remain low in Australia and challenges associated with achieving improved implementation.
Few staff indicated deficits in technical competencies such as being able to accurately identify those eligible for tPA (17%) or confidently interpret brain imaging (17% of physicians). Given the moderate study response rate, it is conceivable that staff with lower competence or confidence may have avoided the survey. Therefore, there is potential benefit from further decision-making training relating to thrombolysis. Less than two-thirds endorsed receiving interactive or competency-based training. The majority of physicians (63%) had not participated in competency-based assessment for acute stroke protocols, although 98% could accurately identify stroke patients, including those eligible for tPA (83%). Interactive and competency-based approaches may enhance staff ability to confidently make decisions regarding challenging cases, 38 with greater access to training potentially optimising staff competence and confidence in stroke care.
There was strong support for tPA as an evidence-based treatment. Over 90% of participants supported items regarding improving odds of independent survival, strength of evidence when administered within 3 h (91%) and evidence that the benefits outweigh the risks (92%). However, 42% to 58% of participants agreeing with statements regarding evidence-based limitations and risk of patient complications is telling. For example, 42% reported that increasing thrombolysis rates would increase rates of poor outcomes, and 42% reported that benefit was difficult to achieve in practice. As negative outcomes often receive significant attention, staff at the early stage of thrombolysis implementation may be particularly influenced by cases with poor outcomes, possibly resulting in reduced treatment of further cases. The opportunity to discuss the evidence base for thrombolysis with more experienced stroke physicians and obtain timely expert review of all cases may be especially valuable for early-stage stroke thrombolysis teams.
Most participants responded favourably to questions regarding the professional context of stroke thrombolysis at their hospital, with more than 80% agreement with leadership and supervision items, with the exception of personal performance monitoring (75% agreement). Workplace culture and practice opportunities appeared positive, although only 35% reported regular performance feedback, 51% reported individual performance goals for stroke and 68% of nurses reported opportunities to develop stroke care skills.
System-related responses were generally positive, with more than 80% agreement with items regarding appropriate policies and processes. The less positive aspects were as follows: availability of checklists or decision aids (78% agreement), diversion of eligible patients to appropriate hospitals (63%) and capacity to make beds available quickly (65%). The latter two are likely to be a hindrance, given the time urgency surrounding this treatment.
Although there was a positive correlation between attitude score and thrombolysis rates, this association was not significant. The study had limited power due to the relatively small number of sites and relatively little variability in average attitude scores between sites (11% power to detect a correlation of 0.1 at 5%).
Stroke care physicians were more positive than nurses and it was clear that emergency physicians were not positive about thrombolysis, as has been reported elsewhere. 37 Emergency physician attitudes are reflected in the Australian College for Emergency Medicine commissioning a review 39 of the evidence for IV thrombolysis to guide a national position statement. 40 Future studies may identify whether this difference relates to perceptions about the evidence or is a result of patient experiences. Given that emergency and stroke physicians thrombolysing more patients had more positive attitudes towards the treatment, older clinicians were more positive than younger clinicians and that performance feedback was generally not included in the training or monitoring that participants received, it is important to clarify how the evidence and personal experience interact to influence practice.
Limitations
It is possible that those with an interest in stroke thrombolysis were more likely to respond to the survey; thus, study results may present a slightly more positive picture of the perceptions regarding stroke thrombolysis. The psychometric properties of the survey have not been tested; therefore, it is possible that there may be potential for bias or inaccuracy. The high proportion of missing data limited the ability of the study to examine characteristics associated with attitude scores. There was no evident pattern to which the participants answered any particular items and no particular item was found to have a relatively high rate of missing data; therefore, this may limit the generalisability of the secondary aims.
Conclusion
Australian hospitals seeking to address barriers to stroke thrombolysis implementation may benefit from the availability of interactive and competency-based training, staff performance feedback, support to make beds available quickly and bypass arrangements to quickly deliver acute stroke patients to appropriate facilities. Given the survey response rate, there is also a need to further explore staff interpretation of the evidence and their stroke thrombolysis experience.
Supplemental Material
Figure_1_correlation_image_1 – Supplemental material for Staff perspectives from Australian hospitals seeking to improve implementation of thrombolysis care for acute stroke
Supplemental material, Figure_1_correlation_image_1 for Staff perspectives from Australian hospitals seeking to improve implementation of thrombolysis care for acute stroke by Christine Paul, Catherine D’Este, Annika Ryan, Amanda Jayakody, John Attia, Christopher Oldmeadow, Erin Kerr, Frans Henskens, Alice Grady and Christopher R Levi in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge the staff at each site who assisted with data collection and analysis. They would also like to express sincere appreciation for the staff members who complete surveys and the Thrombolysis ImPlementation in Stroke Study Group as a whole.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Hunter New England Human Research Ethics Committee is accredited to be a lead committee for ethical approval (Reference Number: 10/06/16/4.03, HREC approval number: HREC/10/HNE/132). Additional approvals were provided by Human Research Ethics Committees in Victoria and Queensland.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is related to a National Health and Medical Research Council (NHMRC) partnership grant (ID569328) and is part-funded by a Translating Research Into Practice fellowship, with collaborative funding from Boehringer Ingelheim and in-kind support from the Agency for Clinical Innovation Stroke Care Network/Stroke Services NSW, Victorian Stroke Clinical Network, National Stroke Foundation and NSW Cardiovascular Research Network–National Heart Foundation, Hunter Medical Research Institute and the University of Newcastle. Christine Paul is supported by an NHMRC Career Development Fellowship (APP1061335). None of these funding sources have had any involvement whatsoever with regard to the concept, development, writing or publishing of this paper.
Informed consent
Participants in the staff survey provided implied consent by completing the anonymous survey. This process for indicating implied consent was approved by the Hunter New England Human Research Ethics Committee. The data on proportion of patients thrombolysed at each hospital were provided in de-identified form under a waiver of consent, which was approved by the Hunter New England Human Research Ethics Committee.
Trial registration
The Thrombolysis ImPlementation in Stroke Project was registered on the Australian New Zealand Clinical Trials Registry (ACTRN12613000939796) and obtained a UTN number (U1111-1145-6762).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.