
Abstract
A 79-year-old Chinese gentleman presented with unilateral acute lower limb ischaemia and received intra-arterial catheter-directed thrombolysis, initially with good result and reversal of the ischaemia. However, he developed an extensive spontaneous spinal epidural haematoma within hours of the procedure and was left with permanent paraplegia after being deemed unsuitable for decompressive spinal surgery. This report serves as a reminder of the risk of severe complications of catheter-directed thrombolysis by describing this rare but devastating side-effect that occurred even despite early detection from onset of symptoms.
Keywords
Introduction
Most centres around the world are familiar with catheter-directed thrombolysis (CDT) and typically perform it for acute lower limb ischaemia or extensive ilio-femoral deep venous thrombosis. In 2014, in the United States alone, 119,000 thrombolysis procedures were performed. 1 The risks of intracranial and gastrointestinal haemorrhage are routinely quoted during consent-taking and balanced against the risk of limb loss during decision making. Yet, the devastating complication of severe haemorrhage is often under-appreciated by both patients and physicians and comes as a shock when it occurs. This report serves as a reminder that CDT is not as benign as it seems and complications, should they occur, can be catastrophic.
Case report
A 79-year-old Chinese gentleman presented with severe right lower limb pain associated with numbness, coldness and weakness some 9 h prior to presentation. Past medical history included intermittent claudication of several years duration (which he had not consulted for before) and a 60 pack-year history of smoking, as well as well-controlled hypertension and hyperlipidaemia. He had no history of diabetes mellitus or ischaemic heart disease and denied any prior trauma or falls.
On examination, his right leg was cool and slightly dusky from mid-calf to the toes with some mild mottling of the forefoot. There was neither fixed-staining nor calf tenderness. Cutaneous sensation was preserved but diminished and power was 2/5 in ankle and foot movements. Ipsilateral distal pulses were impalpable and the anterior tibial (AT), posterior tibial (PT) and dorsalis pedis (DP) artery signals were absent on handheld Doppler examination. There were no obviously appreciable peripheral or abdominal aneurysms. Preoperative blood results were unremarkable, as was the coagulation profile (PT 9.9, APTT 25.7). Electrocardiogram showed sinus tachycardia at 120 beats per minute.
In light of the history of chronic smoking and intermittent claudication, the relatively fair condition of the limb despite a 9-h delay and the absence of a cardiac arrhythmia to suggest an embolic focus, a provisional diagnosis of acute-on-chronic right lower limb ischaemia was made. The patient was systemically anticoagulated with 5000 units of intravenous heparin and an urgent diagnostic angiogram with a view to thrombolysis was organised. The procedure was performed under local anaesthesia, without attempt to perform either spinal or epidural anaesthesia, as follows: after contralateral retrograde access via the left common femoral artery was obtained, a 6 French vascular sheath was inserted. An aortogram through a 4 French pigtail catheter showed a distal abdominal aortic aneurysm and a left common iliac artery aneurysm (Figure 1). The right common, external and internal iliac arteries were patent. There was an acute occlusion of the right superficial femoral artery (SFA) extending into the popliteal and tibial arteries (Figure 2).

Diagnostic aortogram demonstrating an abdominal aortic aneurysm and a left common iliac aneurysm.

Angiogram demonstrating acute thrombosis of the right superficial femoral artery (SFA) with a short stump of SFA proximally.
The thrombotic occlusions within the SFA, popliteal artery and tibioperoneal trunk were treated with pulse-spray thrombolysis (180,000 units Urokinase) and rheolytic mechanical thrombectomy using a 6 F Solent Proxi Angiojet© catheter. Angiogram did not demonstrate either anterior tibial artery (ATA) or posterior tibial artery (PTA) stumps after clearing the proximal occlusions and on the lateral foot runs the DP reconstituted via a mature collateral arising from the peroneal artery. The distal ATA was faintly visible and severely stenotic. As these indicated chronic occlusions of the ATA and PTA, no attempt was made to recanalize them. The distal SFA was ectatic (Figure 3(a)) and had some residual thrombus within it which was treated with balloon angioplasty, with angioplasty performed to the tibioperoneal trunk and peroneal artery as well. Flow to the foot was ultimately re-established via the peroneal artery to the DP artery and into the plantar arch (Figure 3(b) and (c)). As there were still some minor residual thrombii within the ectatic segment of the distal SFA at the adductor hiatus and popliteal artery, low-dose urokinase and heparin were administered overnight (30,000 and 900 IU/h, respectively) via a Cragg-McNamara infusion catheter positioned within the segment of nonocclusive residual thrombus (Figure 3(d)). Post-procedure the patient’s symptoms of right lower limb pain and weakness resolved along with the duskiness, and his ipsilateral DP pulse was restored.
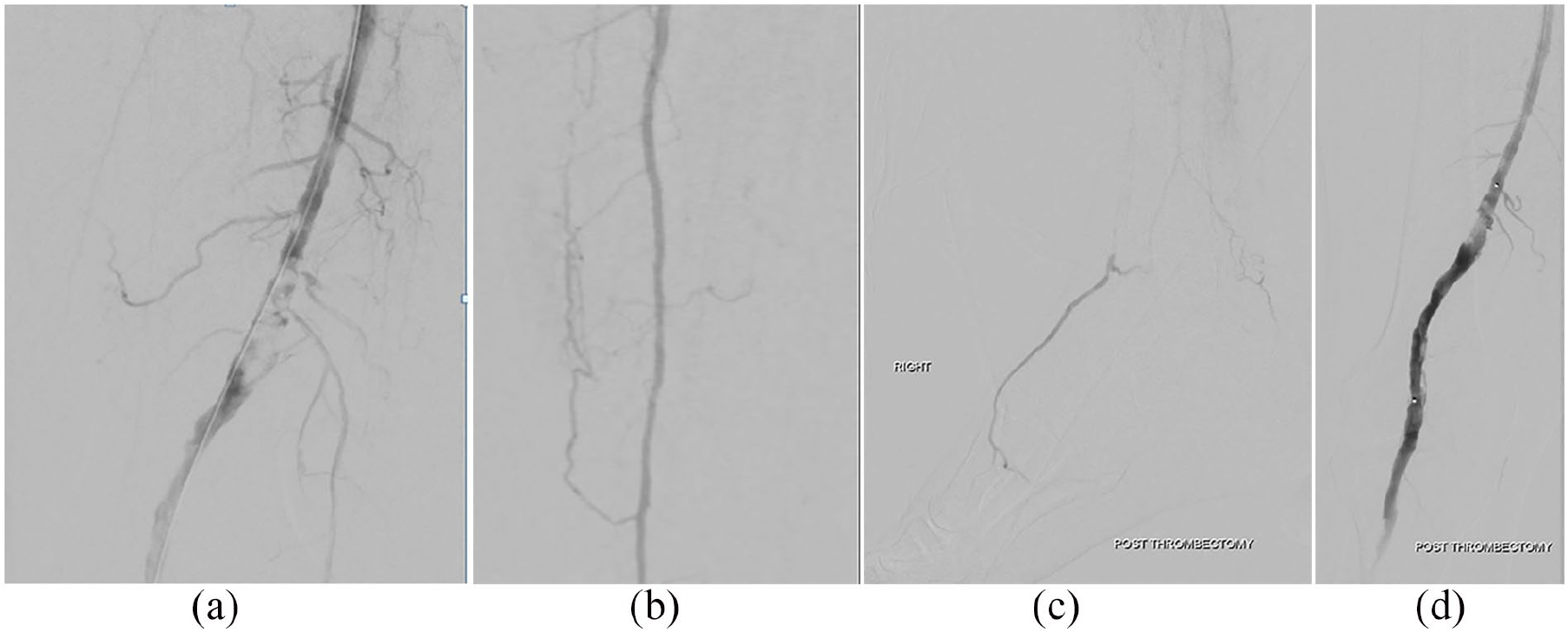
(a) Post-rheolytic mechanical thrombectomy demonstrating patency of the SFA but residual thrombus within an ectatic-appearing segment of the superficial femoral artery, (b) distally flow was re-established in the peroneal artery, (c) peroneal artery giving collateral to dorsalis pedis artery which continued to plantar arch and (d) overnight thrombolysis via Cragg-McNamara catheter positioned across residual distal SFA and popliteal thrombus.
Six hours after commencing CDT, he complained of inability to move or feel his legs bilaterally. Clinical examination revealed a T4 sensory level with a near-complete loss of bilateral lower limb motor function and anal tone. Pulses remained strong in both feet. The urokinase and heparin infusions were discontinued immediately. Urgent computed tomography (CT) brain and magnetic resonance imaging (MRI) of the whole spine were performed. CT brain demonstrated a small subarachnoid haemorrhage within the posterior fossa with blood in the foramen magnum and fourth ventricle as well as superior herniation of the brain stem. MRI spine showed extensive haemorrhage within the thecal sac from the foramen magnum to T9 involving both subdural and subarachnoid compartments with compression of the cord at multiple levels. Focal epidural haematomas were present at T2 to T3 measuring 4 mm × 5 mm and posterolateral to C5 to C6 measuring 3 mm, with anterior epidural haematoma extending from T2 to T9 levels and there was oedema of the cord from C2 to T8 (Figure 4).

(a) T2-weighted axial image of the cervical spine demonstrating heterogeneous signal abnormality in keeping with a subdural haematoma (white arrow). (b) T2-weighted sagittal image of the thoracic spine demonstrating ventral subdural haematoma from T4–T9 levels (white arrow).
No obvious cause for the intra-thecal haemorrhage was identified and there were neither focal-enhancing lesions nor areas of restricted diffusion to suggest infarction. There was no any evidence of a vascular malformation. The heparin was reversed with intravenous Protamine Sulphate and the patient commenced on intravenous Dexamethasone 8 mg TDS. An urgent neurosurgical consult was obtained; however, the neurosurgeon declined to operate, citing extensive blood in the spinal canal with widespread cord swelling and mass effect on imaging which would require overly extensive laminectomy and instrumentation with high chance of cord herniation and inability to achieve closure, as well as high risk of further bleeding and a poor neurological prognosis from the long duration of cord compression overnight (of some 8–9 h). The patient was instead started on medical management with intravenous steroids, in consultation between the neurosurgeon and family.
A repeat angiogram of the right lower limb three hours after discontinuation of thrombolytic and heparin infusion showed re-occlusion of the SFA. The patient subsequently underwent an above knee amputation for his nonviable right lower limb. Intraoperatively a 3 × 3 cm area of necrotic adductor muscle was present at the incision line requiring proximal debridement. Furthermore, a 4 cm distal SFA aneurysm was encountered, containing extremely firm established thrombus. The thrombus was removed piecemeal with considerable effort using an artery forceps to crush and avulse the thrombus and the proximal SFA trawled with a Fogarty embolectomy catheter restoring forward flow. The wound subsequently healed well.
The patient has since developed a lower limb below-knee deep vein thrombus with pulmonary artery embolism necessitating placement of a retrievable inferior vena cava filter and anticoagulation with enoxaparin, which was initially complicated by a large gluteus medius hematoma. The enoxaparin was subsequently resumed with close follow-up by a haematologist. CT aortogram demonstrated a fusiform 3.8 cm infrarenal aortic aneurysm with a small rind of thrombus and bilateral 2.2–2.8 cm common iliac aneurysms (Figure 5) which he has declined intervention for. Transthoracic echocardiogram returned normal without evidence of thrombus. He remains paraplegic and wheelchair bound a year later.
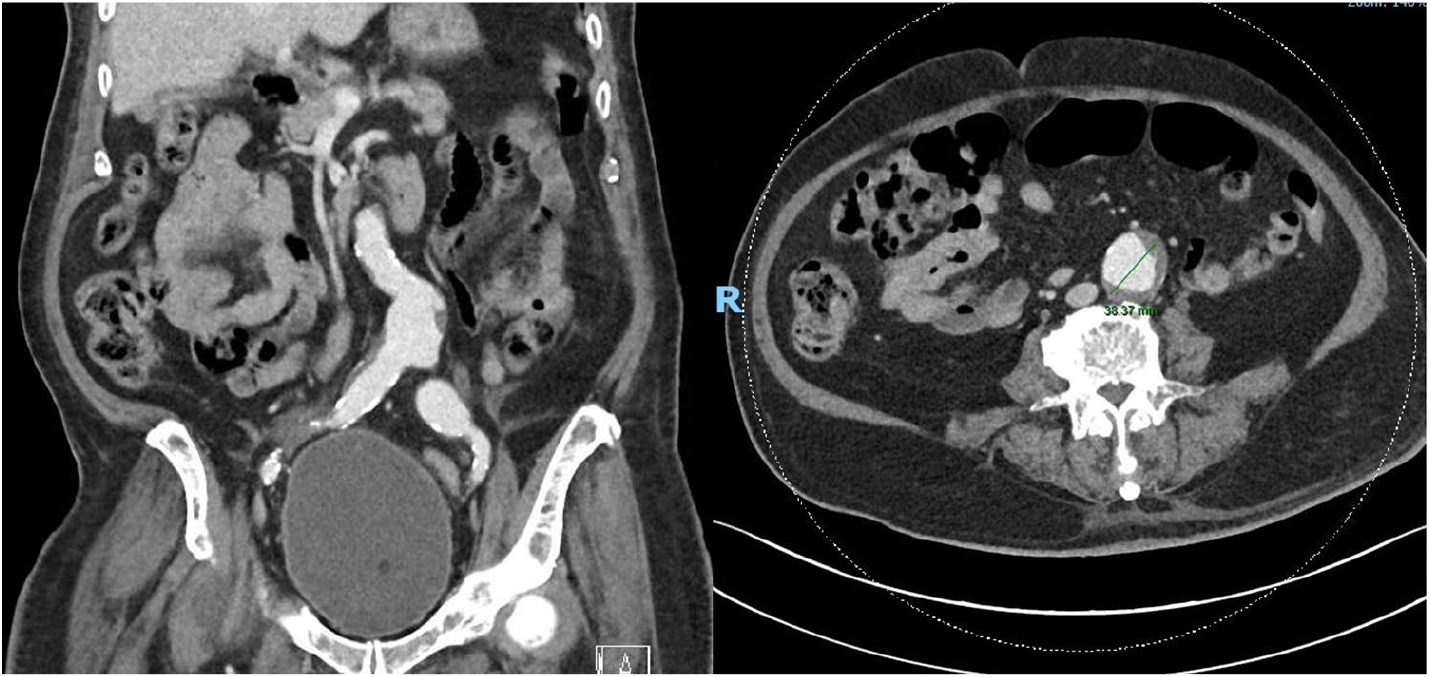
CT aortogram demonstrating the aortoiliac aneurysm with small amount of thrombus within.
Discussion
Acute limb ischaemia carries significant rates of morbidity and mortality with some reports quoting in-hospital mortality rates of 9%–12%. 2 Prompt treatment is necessary to prevent deterioration and options include anticoagulation alone, primary amputation, surgical revascularisation (usually by open embolectomy) and percutaneous catheter–directed thrombolysis (CDT) with or without mechanical thrombectomy. CDT may be chosen only if the following criteria are satisfied: (a) there are no absolute contraindications to thrombolysis, (b) the symptoms of limb ischaemia have been present for less than 14 days and (c) the predicted time taken to re-establish antegrade flow will be short enough to preserve limb viability. Technical success (restoration of antegrade flow and dissolution of at least 95% of the occlusion) rates are good at around 80%, but there is a risk of significant bleeding. A systemic bleeding risk of 1%–2% is often quoted, while the risk of intracerebral haemorrhage (ICH) is quoted at about 5%. Acosta et al had major haemorrhage rates of 13.9% in 104 procedures of which 43 (5.7%) were so severe that thrombolysis had to be discontinued. Three patients had haemorrhagic strokes (0.4%), all of which were fatal. 3 The STILE and TOPAS trials both found risks of ICH of between 1% and 2% with CDT.4,5
SSEH following CDT is exceedingly rare. To our knowledge, this is the first case of SSEH following intra-arterial thrombolysis for acute lower limb ischaemia. The term spontaneous spinal epidural haematoma (SSEH) is in fact a misnomer and refers to an atraumatic origin regardless of aetiology rather than an idiopathic onset. In the majority of cases, there is no cause identified. It is believed that the source of bleeding is usually from weakened epidural veins (the ‘locus minoris resistentiae’). The incidence of SSEH is estimated at 0.1 per 100,000. 6 Risk factors for SSEH include anticoagulation, aspirin, vascular malformations, venous epidural plexus defects, hypertension, pregnancy, physical exertion, haematological disorders and epidural analgesia.7–9 SSEH has also previously been reported in a patient on Clopidogrel 10 and on patients on intravenous heparin, although the latter is most frequently on the background of recent lumbar puncture or spinal anaesthesia. 11 The most common presenting symptoms of SSEH are neck or back pain with or without radiating radicular pain. Neurological dysfunction either begins concurrently or follows soon thereafter.
In our patient, a provisional diagnosis of acute-on-chronic limb ischaemia led to the decision for CDT in favour of surgical embolectomy. Radiologically, the abdominal aortic aneurysm appeared small and stable with smooth walled thrombus making it unlikely to be a source of embolus, and there were features of chronicity including mature collaterals both above and below the knee and chronic occlusion of the AT and PT arteries. The clinical picture was of an acute deterioration on a background of existing peripheral vascular disease, likely representing in situ thrombosis of a severely narrowed lumen within the SFA aneurysm. The patient subsequently suffered SSEH as a result of thrombolysis.
Although not observed in our case, spinal cord haematoma (haematomyelia) is a similarly rare entity which can be associated with systemic anticoagulation. First described by Tellegen in 1850, the usual presentation is with sudden-onset back or neck pain together with acute or evolving neurological deficit. Aetiology can be divided into traumatic or non-traumatic causes, with non-traumatic causes including vascular malformations, clotting disorders, inflammatory myelitis, spinal cord tumours, abscess, syringomyelia, or idiopathic origins. Spontaneous haematomyelia has been reported in association with warfarin as well as in patients with intrinsic coagulopathy. 12
The prevailing thinking is that rapid surgical evacuation of the haematoma and neural decompression within 48 h is an important predictor for positive outcomes, 13 and although there are a few reports of successful management with conservative care, the described patients were often showing signs of improving neurological deficits at presentation.14,15
In a retrospective cohort study of 14 patients with a mean interval from presentation of neurological deficit to surgery of 21.29 ± 10.2 h, all had favourable responses to surgical intervention, except for one patient who had a 10-day delay till surgery. Multilevel decompressive laminectomy and hematoma evacuation was performed in 13 of the 14 patients, with one patient requiring extensive decompression of eight levels. 16
In another case series of three patients who suffered SSEH, one of the three patients was operated on late at 72 h, yet still achieved complete neurological recovery, suggesting a role for surgery even when delayed past 48 h. 17
A case of fatal SSEH 50 h post systemic thrombolysis with rTPA for an extensive acute myocardial infarction has been described, where the extradural hematoma was so extensive as to affect the C1–T1 levels, resulting in respiratory failure. 18
Conclusion
The importance of prompt diagnosis of this rare but devastating complication of CDT cannot be overemphasised since continuing anticoagulation may prove fatal. A low index of suspicion is essential for timely detection, and early surgical decompression is mandatory for optimal neurological outcomes. Despite prompt reversal of anticoagulation and corticosteroid administration, our patient was unfortunately deemed unsuitable for spinal cord decompression and hematoma evacuation, and his outcome and prognosis have been dreadful. It is hoped that this report will give the reader a greater appreciation that CDT, while generally successful, carries the potential for great harm in the form of SSEH.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.