
Abstract
Background and Aims:
Radical surgical intervention is necessary to save patients’ lives in cases of necrotizing fasciitis. This leads to persistent disabilities and most likely to a deteriorated quality of life. The purpose of this study was to evaluate the midterm outcomes after survival of necrotizing fasciitis.
Materials and Methods:
A retrospective analysis of 69 patients, treated for necrotizing fasciitis between 2003 and 2012. The patients were identified using the International Classification of Diseases (10th Revision) code M 72.6. Of the 50 survivors, 22 patients completed the Short Form 36 and Short Musculoskeletal Function Assessment questionnaires as a postal survey. The follow-up averaged 59 months (range: 6–128 months).
Results:
The average age at the time of necrotizing fasciitis was 60.0 years. The body mass index average was 29.7. The patients had a significantly decreased physical component summary score of 33.3 compared to a normative group (p < 0.001) (Short Form 36). They further showed a significantly decreased dysfunction and bother indices (Short Musculoskeletal Function Assessment) (p < 0.001). An increased age (⩾70 years) was associated with an inferior role emotional (p = 0.048) and physical functioning (p = 0.011) as well as social functioning (p = 0.038) (Short Form 36). The majority of patients (16, 72.7%) complained of pain at the final follow-up and 50% of patients required an assistive device on a regular basis.
Conclusion:
Patients who survived necrotizing fasciitis suffer from functional impairment and changed body appearance. Assistive devices or pain medication are often required, and the patients present with significantly decreased physical, social, and emotional functioning at the midterm follow-up. The patient’s age is a critical factor regarding functional or mental outcome parameters. Further research on the post-hospital course and long-term multidisciplinary care is required to improve the outcomes of these patients.
Keywords
Introduction
Necrotizing fasciitis (NF) remains a dreaded infectious disease because of its high mortality rate, which ranges from 6% 1 to 76%, 2 and its risk for delayed diagnosis, because of the similarity to other soft tissue infections or noninfectious cutaneous diseases such as pyoderma gangrenosum, abscess, erysipelas, skin ulcers, or cellulitis, especially at the early state of NF.3,4
The causes, risk factors, and microbes have been identified and the classification systems5,6 as well as scores to identify patients with a high risk for NF, such as the LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score, 7 have been established in the past; however, it still remains a challenging disease for surgeons. Prompt and radical surgical intervention is necessary to save the patient’s life. After surviving NF, the appearance of patient’s body is likely to have changed by several operative procedures, amputation, skin mesh graft, free tissue transfers, or other procedures for wound closures after radical debridement. Patients may be disabled for the rest of their life and less is known about the mid- or long-term outcomes after the survival of NF.
Only a few studies have been performed focusing on the outcomes after NF in the past.8–11 Most follow-up investigations are on burn patients, which also suffer from an altered physical appearance.12–15 The purpose of our study is to report about the midterm outcomes of patients who survived NF using two standardized outcome scores.
Material and methods
The study was approved by the institutional ethics committee (approval number: 3962). Between January 2003 and December 2012, we retrospectively reviewed all patients, who were treated for NF at our Department of General and Trauma Surgery in a level one trauma center. Patients were identified using the ICD-10 (International Classification of Diseases, 10th Revision) code M 72.6. Patients aged ⩾18 years with clinically and histologically confirmed NF and operative intervention at our department were included in the study.
The SMFA-D (Short Musculoskeletal Function Assessment) 16 and SF-36 (Short Form 36) 17 questionnaires were sent to all survivors by mail as a postal survey. Nonresponders were contacted by phone one time. Four patients reported being very much distressed after the disease, and they denied the participation in the study because they did not want to have “anything to do with a hospital at all.”
The results of both questionnaires were analyzed using the results of Hopman et al. 18 and Hunsaker et al. 19 providing the reference values. Patient’s demographics, pre-existing diseases, body mass index (BMI), ASA score (ASA Physical Status System), location (upper extremity, lower extremity, torso), cause (traumatic/atraumatic), and classification (type I-IV) of NF were documented. All patients received initial antibiotic treatment according to department guidelines. Surgical treatment was based on the perioperative findings and remained at the discretion of the individual surgeon. Full thickness biopsies (cutis, subcutis, fascia) were taken for histopathological and microbiological probes.
The number of transfusion of packed red blood cells (pRBC) and the necessity for amputation were recorded. The rates of patients developing an acute respiratory distress syndrome (ARDS), acute respiratory failure (ARF), multiorgan failure (MOF) or renal failure, disseminated intravascular coagulopathies (DIC), and the necessity of admission to the intensive care unit (ICU) were analyzed.
Statistical analysis
The sample size was calculated using G*Power®. Primary outcomes were differences in the SMFA and SF-36, which were used as variables for calculation of the sample size. For the SMFA, a minimal sample size of 15 patients in each group (NF vs normative control group) will have a 95% power to show differences of 15.0 in the mean of the functional outcome scores of the SMFA DYSFUNCTION and BOTHER indices. A standard deviation of 15.0 using a t-test of two independent groups has a double-tailed significance level of 0.05. For the SF-36, a minimal sample size of 20 patients in each group (NF vs normative control group) will have a 95% power to show differences of 15.0 in the mean of the functional outcome scores of the SF-36 physical component summary (PCS) and mental component summary (MCS). A standard deviation of 15.0 using a t-test of two independent groups has a double-tailed significance level of 0.05. For analysis of variables such as age, BMI, and ASA regarding functional outcomes, a multivariate regression was performed. Descriptive statistics were completed, including percent, mean, range, and standard deviation, using Microsoft Excel, 2010. Nominal variables were evaluated using the chi-square test, unless the sample size was too small, in which case the two-tailed Fisher’s exact test was used. Significance was determined at p < 0.05. The data were analyzed using SPSS version 22.0 (IBM, Armonk, NY).
Results
We were able to identify 69 patients. Nineteen (27.5%) patients died during the hospital stay because of the NF. Twenty-six patients (54.2%) did not respond, and 2 patients were deceased, independent of the NF (Figure 1). In total, 22 survivors completed the questionnaires for evaluation. Patients’ follow-up averaged 59 months (SD (standard deviation) 34; range: 6–128 months). On average, patients were 60.0 years old at the time of the NF (Table 1). Eighteen (81.8%) patients had pre-existing diseases such as diabetes mellitus type 1 or 2 (4, 18.2% patients), chronic heart failure/arrhythmia (4, 18.2% patients), hypertension (7, 31.8% patients), chronic respiratory disease (1, 4.5% patients), obesity (BMI ⩾ 35) (3, 13.6% patients), and illicit drug abuse (1, 4.5% patients). Surgery was performed on an emergency basis as soon as NF was diagnosed, which was on average 8 h (range: 1–178 h) after admission. A revision surgery was performed in 21 (95.5%) patients after 24–48 h. The patients required 3.8 (SD: 2.3; range: 0–10) operative revisions on average. In 13 (59.1%) patients, definitive wound closure was performed using a skin mesh graft.

Flow chart for patient selection.
Demographics, BMI, ASA, location, and cause of NF.
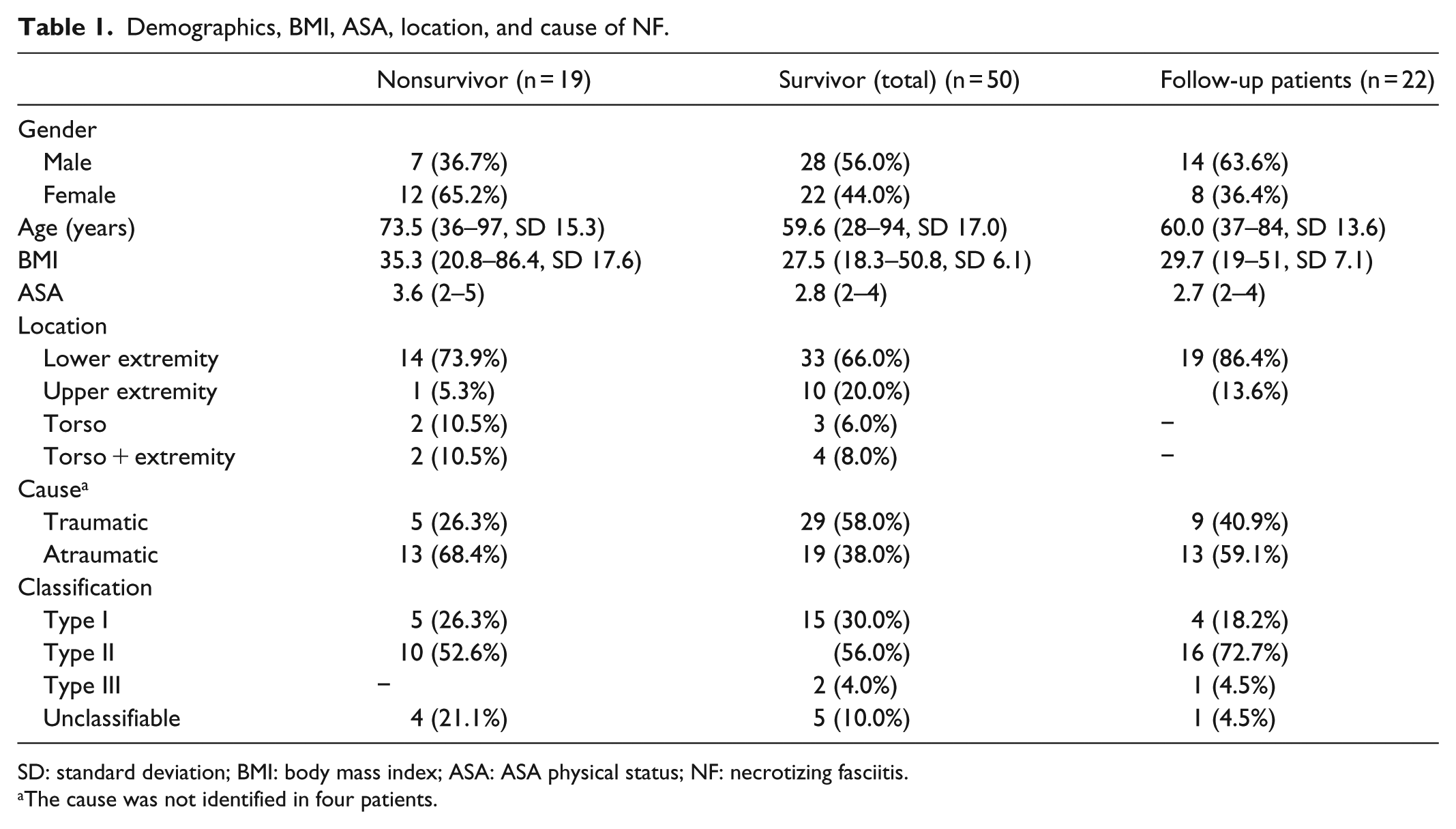
SD: standard deviation; BMI: body mass index; ASA: ASA physical status; NF: necrotizing fasciitis.
The cause was not identified in four patients.
Four (18.2%) patients required amputation (below-knee amputation (2), shoulder-exarticulation (1), and hip-exarticulation (1)). Two (9.1%) patients required an artificial anus (anus praeter). Patients required an average of 14.2 (SD: 22.2; range: 0–68) pRBC. Sixteen (72.2%) patients developed an ARDS (1), ARF (1), MOV (1), DIC (2), septic shock (2), and/or were admitted to the intensive care unit (8) during their hospital stay (Figure 2).

Distribution of complicating factors during the hospital stay.
On follow-up, 8 (36.4%) patients were pensioners, 1 (4.5%) patient was unemployed, 3 (13.6%) worked in medium physically demanding jobs, and 10 (45.5%) patients did not provide their working status. The results of the SMFA-D and SF-36 questionnaires are shown in Table 2. The patients had a significantly decreased PCS score of 33.3 (p < 0.001) in the SF-36 questionnaire and a significantly decreased dysfunction and bother indices in the SFMA questionnaire (p < 0.001) compared to a normative group (Table 2).
SF-36 and SMFA.

SD: standard deviation; CI: confidence interval; SF-36: Short Form 36; SMFA: Short Musculoskeletal Function Assessment; PCS: physical component summary; MCS: mental component summary.
Hopman et al. 18
Hunsaker et al. 19
An increased age (⩾70 years) was associated with an inferior role emotional (RE) (p = 0.048) and physical functioning (PF) (p = 0.011) as well as social functioning (SF) (p = 0.038) scores (SF-36). An increased BMI (⩾25) showed a decreased MCS (p = 0.025). The BMI and ASA showed no significant associations with regard to the outcome parameters in the SMFA; however, older patients’ age (⩾70 years) was related to an inferior outcome in daily and mobility indices (SFMA), which was not statistically significant.
Sixteen (72.7%) patients complained of pain at the final follow-up. Sixteen (72.2%) patients took pain medication (always (8), intermittently (4), or seldom (4)), and 11 (50%) patients required an assistive device (walking cane (1), rollator (4), or wheelchair (6)) on a regular basis. Ten (45.5%) patients required individual footwear (heel lift (2), customized (4), or prosthesis (4)).
Discussion
NF remains a challenging infectious disease and past research has mainly focused on pathogens,20,21 diagnosis,22,23 risk factors, 24 treatments,25–27 or determinants of mortality25,28,29 to help understand the complexity of the disease and to develop treatment guidelines. It is indisputable that immediate radical surgical intervention followed by antibiotic treatment and intensive care is necessary to save the patients’ lives. However, the scars, amputations, anus sphincter, and the large areas with mesh graft transplantation or free tissue flaps to restore the integument after extremity salvation may lead to permanent disability due to joint contractures or hypo- or hyperesthesia. Assistive devices and permanent need for care might be necessary. Pham et al. reported extremity involvement as an independent factor of a higher functional limitation in patients after survival of NF, but they also showed that a performed amputation had no further impact on the functional limitation. In their study population, 30% of patients presented mild-to-severe functional limitations. 10
To further understand the outcomes of survivors, we asked the patients to complete the SMFA-D and SF-36 questionnaires. Czymek et al. 8 reported significantly decreased SF-36 Role Physical functioning, Physical Functioning, General Health and Physical Health Summary, as well as a deterioration of sexual function in patients after survival of Fournier’s gangrene compared to a normal population. Even though we did not treat patients with a Fournier’s gangrene, we observed similar results in our study population with significantly decreased physical functioning, role-physical, general health and PCS scores (SF-36) and a significantly decreased dysfunction and bother indices (SFMA). Gawaziuk et al. 11 reported a decreased MCS (44.5) and PCS (36.5) in 56 patients (mean age 51.5 years) with NF and a mean follow-up of 257 weeks (range: 8.4–495.4; SD: 130), which are similar to our results (MCS: 47.1; PCS: 33.3). The observed association between an increased age (⩾70 years) and an inferior role emotional, physical functioning, and social functioning (SF-36) scores and inferior outcome in daily and mobility indices (SMFA) is likely not only the result of surviving NF alone but also the result of an increased disability with age in general, which we did not further differentiate. However, especially for the elderly, the outcome after NF might be worse than the outcome for younger patients. Pikturnaite et al. reported the capability of psychosocial adjustment after NF to be improved with longer follow-up and older age. However, they also observed that pain, physical limitation, and energy levels were more relevant in older individuals and improved slower with time compared to psychological issues. They reported an average SF-36 score of 65.8 in 10 survivors of NF. They further included the Derriford-Appearance-Scale-24 (DAS) in their investigation to assess the degree of distress with regard to one’s appearance. The average score was 38, presenting a moderate level of distress. 30 Gawaziuk et al. reported a significantly worse MCS for younger patients (39.2) compared to patients older than 51.5 years (49.8). Furthermore, they observed a worse PCS in unmarried individuals (32.4) compared to married individuals (38.9). 11 Hakkarainen et al. found in an interview with 18 survivors at a median follow-up of 4.2 years that patients reported their quality of life to be significantly affected by their physical functioning and ongoing pain. Depression and post-traumatic stress were additionally reported. 9 A prevalence rate of 46% for mild-to-moderate symptoms of depression in burn reconstruction patients was reported by Thombs et al. 12
In our study population, only 22 patients completed both questionnaires. We were able to contact four patients, who did not complete the questionnaires, by phone and spoke with them about the reasons they refused to participate in the study. They reported to be in enormous distress after the disease and thus did not want to be in further contact with a hospital at all. This implies that the results might be even worse if those patients had participated in the study. Similar observations were reported by Pikturnaite and Soldin, 30 in which two of three patients reported being too distressed to talk about their experiences.
There are some limitations to this study. The retrospective nature should be considered. Furthermore, over 50% of the survivors were excluded from the study, as most of them did not return the questionnaires, which may have created a selection bias. The reference values, which were used for the normative population, are not based on the German population, which may have influenced the analysis results of the SMFA and SF-36. The number of patients returning the questionnaires is still small and larger series are further required to underline the statistical significance. The strength of the study is the focus on the post-hospital outcomes of patient’s who survived NF, which has been less of a focus in previous literature.
Conclusion
Following these results, after surviving NF, patients present with decreased physical, social, and emotional functioning outcome scores at the midterm follow-up. The patient’s age is a critical factor regarding functional or mental outcome parameters. Long-term multidisciplinary care, including physiotherapy and psychotherapy, should be provided after the survival of an NF to help patients adjust to their functional impairments and changed body appearances. This further substantiates the importance of continued research on the post-hospital course with the goal of improving the outcome of the survivors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Ethic Committee of the Ruhr-University Bochum (Bergmannsheil GmbH) (Approval Number: 3962).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge support by the DFG Open Access Publication Funds of the Ruhr-Universität Bochum.
Informed consent
In addition to the questionnaires, the patients received a letter with information about the study, protection of data privacy, and their right to withdraw from the study at any time. Informed consent was obtained by sending back the questionnaires. This was in agreement with the ethical committee and proofed prior to the start of the study.