
Abstract
Bier anemic spots, cyanosis, and urticaria-like eruption comprise the recently defined BASCULE syndrome. This rare and benign condition has been reported in approximately 15 individuals in the literature. We present three new cases of BASCULE syndrome occurring in adolescents with interesting associations.
Introduction
The current understanding of the pathogenesis of BASCULE syndrome includes a vasomotor dermatosis that can occur from venous stasis. 1 Features differentiating BASCULE syndrome from acrocyanosis include Bier anemic spots, red-orange macules representing the urticaria-like eruption, and the background cyanosis. 2 BASCULE syndrome has also been noted to produce paresthesias and edema. 3 The urticaria-like eruption in BASCULE syndrome has been proposed to be a response to hypoxia of tissues. 1
Cases
Case 1
A 15-year-old female experienced her first eruption of pruritus, warmth, and skin changes at the age of 12. These dermatologic changes would begin at the distal legs and would stay localized to the legs and thighs (Figure 1). The legs would be pruritic and warm, and the entire episode would last 10–15 min. The patient noticed the eruptions usually occurred during summer months while standing and occurred approximately once a week. There were no new medications started prior to the initial eruption, and there were no associated pre-syncopal or syncopal episodes. Past medical history included premature delivery and fifth disease at less than 2 years old. Medications included drospirenone-ethinyl estradiol. Family history included the mother having a history of BASCULE syndrome that first presented at the age of 11 and resolved at the age of 25. On examination, the patient did not have an eruption at the time. However, the patient had an image of a previous eruption that displayed cyanotic changes with discrete oval pale patches and urticoid plaques on the lower extremities (Figure 1). Investigations including complete blood count, liver enzymes, and liver function tests were within reference ranges. A trial of oral cetirizine 20 mg once daily was started which helped to reduce the number of eruptions.

Bier anemic spots, cyanosis, and urticaria-like eruption on the bilateral lower extremities.
Case 2
An 18-year-old male presented with a history of red welts, mottled skin, and abrupt color changes of red and a cyanotic hue on the lower extremities. Before the cutaneous eruption, the individual would feel paresthesias and cold in the lower extremities. The first of these episodes was at the age of 15. These eruptions would start on the lower extremities and sometimes would also involve the trunk and face. The episodes could happen 20–30 times per day and resolve within 10–45 min. The episodes would typically occur after standing for a long time or while experiencing a period of stress. There were no pre-syncopal or syncopal episodes associated with these eruptions. Past medical history included autism spectrum disorder, attention deficit hyperactivity disorder (ADHD), dyslexia, anxiety, migraines without aura, and uveitis, and also included pre-syncopal episodes that were not temporally associated with the BASCULE syndrome eruptions. Family history included Crohn’s disease, rheumatoid arthritis, and systemic lupus erythematosus. Medications included methylphenidate (Concerta), sertraline, Nexium, topiramate, amitriptyline, Cambia, Epuris, and vitamins B2 and D3. During physical examination, there was no mottling or urticaria on the skin. The patient had photos of their previous eruptions (Figure 2(a)–(c)). Complete blood count, liver enzymes, liver function tests, inflammatory, and autoimmune workup were non-contributory. A workup for postural orthostatic tachycardia syndrome (POTS) was negative. A trial of oral cetirizine 10 mg taken once a day began. This was switched to cetirizine 20 mg taken once in the morning and diphenhydramine (Benadryl) in the evening which produced a decrease in flares. Management was later switched to bilastine 20 mg taken orally twice daily which improved the eruptions more than cetirizine or diphenhydramine.
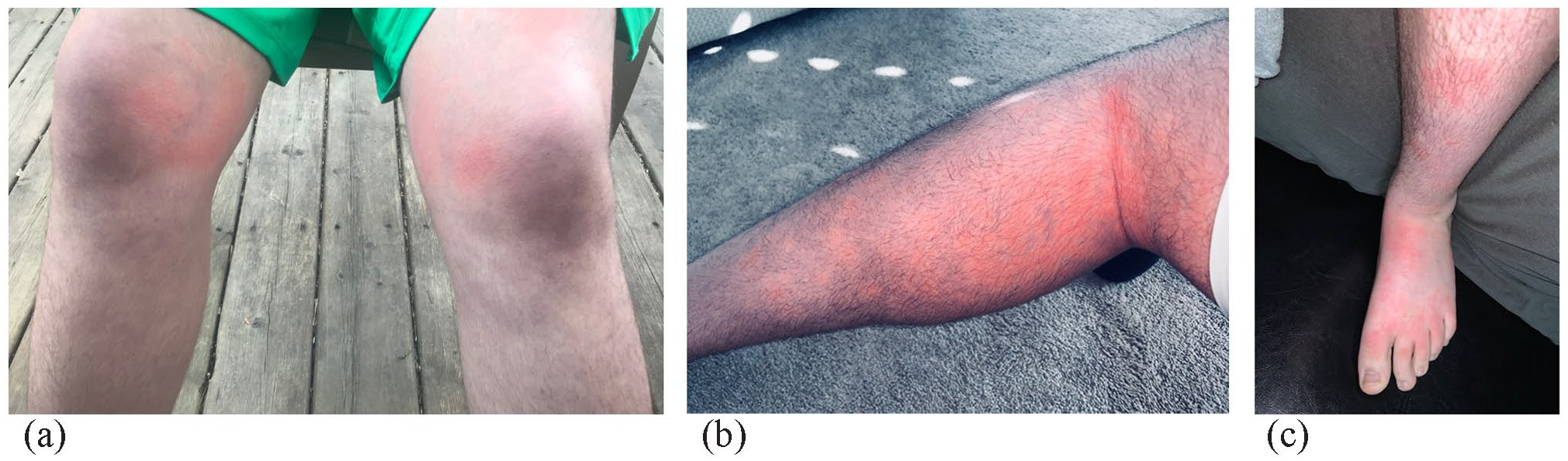
(a) Erythematous urticaria-like eruption with a pale halo with cyanotic changes on the knees and lower extremities, (b) Erythematous, urticaria-like macules and patches, pale macules, and cyanotic changes, and (c) Erythematous urticaria-like macules with a pale hue and interspersed cyanotic changes.
Case 3
A 15-year-old male first had a presentation of BASCULE syndrome when standing up after lying down. The eruptions would begin on the legs and stay localized to the legs and thighs (Figure 3(a) and (b)) and dorsum of the feet. The episodes would last approximately 15 min and appear more often in the late evening, with exercise, moving from sitting to standing, and occasionally with showering. Interestingly, while running, the individual would also experience similar skin changes on the arms. The individual reported that occasionally the lower extremity veins appeared more prominent during the cutaneous manifestations. During the episodes, the individual felt the dorsum of the feet become warm and felt lower extremity pruritus and paresthesias. The legs would appear cyanosed. There was no pre-syncope or syncope associated with the episodes. The individual had a past medical history of ADHD, asthma, and eczema. Family history was unremarkable. Medications included methylphenidate (Concerta). At the time of physical examination, there was no active BASCULE syndrome eruption. The individual had pictures that clinically displayed features of BASCULE syndrome on the lower extremities (Figure 3(a) and (b)). Complete blood count, liver enzymes, liver function tests, and inflammatory and autoimmune investigations were unremarkable. Oral cetirizine 20 mg once daily was recommended, which helped to decrease the frequency of episodes.
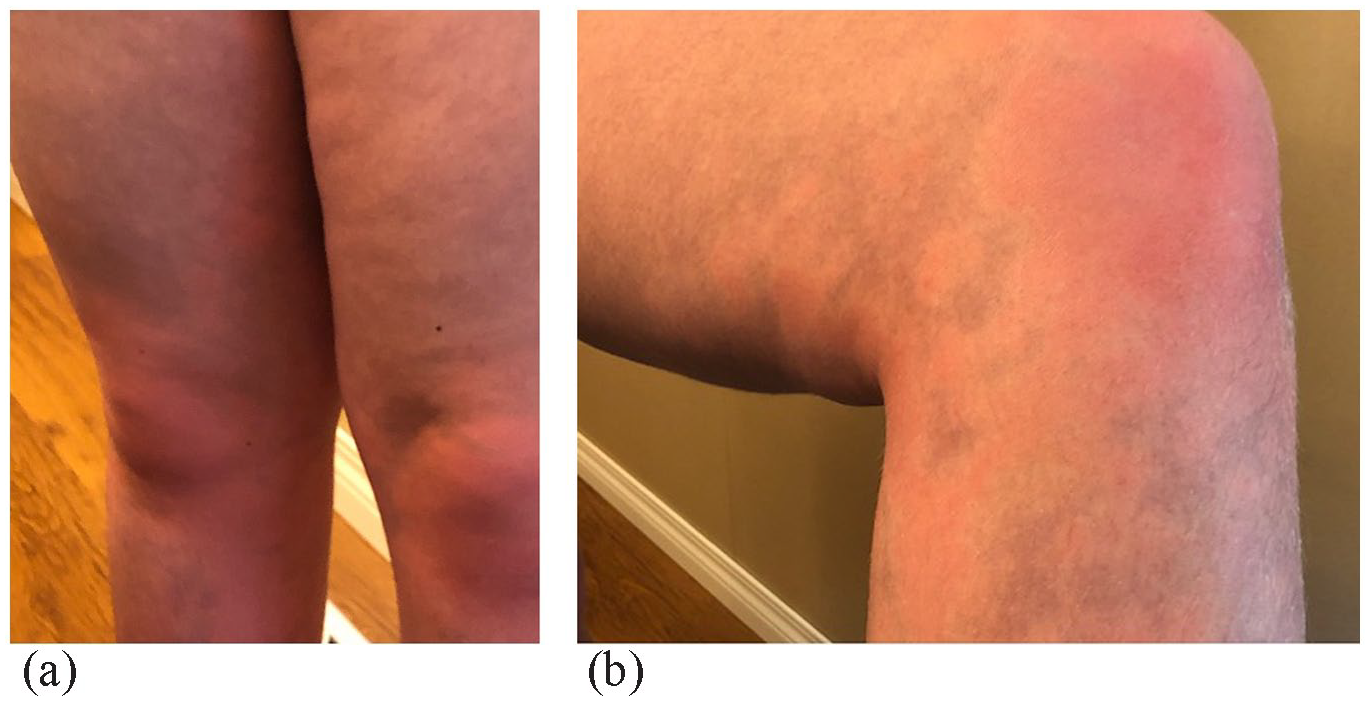
(a) Cyanosis of the lower extremities with erythematous and pale macules. (b) Erythematous patches with relatively pale macules with a background cyanosis.
Discussion
August Bier was a German surgeon who first described anemic spots in 1898. 4 BASCULE syndrome is a recently described condition that has a small number of reported cases. The limited number of cases in the literature necessitates the importance of exploring associations with the condition. Some of the previously reported associations include COVID-19, POTS, orthostasis, and syncope.5–7
The three new cases we present add additional associations to the current literature. A commonality among many of the cases in the literature is the occurrence of BASCULE syndrome in youth.3,6 In our series, all three individuals are adolescents.
One of the new findings we add to the literature is an association of family history in BASCULE syndrome. In case 1, the mother of the patient also experienced BASCULE syndrome in their adolescent and early adult years. To our knowledge, at present there are no cases in the literature that have reported an association with a first-degree relative. This presents the potential for a heritable or genetic component to BASCULE syndrome. Another association that was demonstrated in the present case series is a potential association with ADHD. Both individuals in case 2 and case 3 had a past medical history of ADHD and were taking methylphenidate (Concerta). This association is also demonstrated in a previous case reported by Berrebi et al. 5
Guillen-Climent et al. 7 have reported a case associated with first-degree atrioventricular block and orthostasis. The literature has supported the association of orthostatic changes with or without POTS with BASCULE syndrome.2,3 In our case series, all three individuals found that standing was an associated precipitant for their BASCULE syndrome eruption, consistent with the BASCULE syndrome definition and previous literature. 1 None of the individuals in our series had pre-syncopal or syncopal episodes associated with the eruptions. The individual in case 2 had pre-syncope not temporally associated with BASCULE syndrome eruptions, and their workup for POTS was negative.
We present three cases of the rare condition BASCULE syndrome in adolescents, with a first-reported association of family history. We have also presented a potential association with ADHD or its treatment. Furthermore, reports of BASCULE syndrome will aid in the understanding of risk factors, mechanisms of pathogenesis, and associations with the condition.
Footnotes
Acknowledgements
The authors thank the patients and their families.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Patient consent
All patients and a parent of patients provided consent to be involved in the case series and have photos published.