
Abstract
Background:
The population-based information on the prevalence of stroke from rural areas of Middle East countries including Turkey is unknown. Our aim is to evaluate the prevalence of stroke in those ⩾18 years in the Turkish population in a rural area of Istanbul.
Methods:
A cross-sectional door-to-door study was conducted in a rural area of Istanbul between 1 March and 30 March 2013. A research protocol recommended by World Health Organization for developing countries was used. Each screening teams consisted of one neurologist, one local nurse, and five surveyors. Teams were trained about the survey and questionnaire. The patients, who claimed to have suffered a stroke, were examined, and the diagnosis was confirmed by a neurologist on site. The findings and medical records were documented.
Results:
In total, 2906 people ⩾18 years were screened. 50 stroke cases were detected. 80% of those were found to have had an ischemic stroke, 14% of those were hemorrhagic cases, and 6% of those had an unclassified stroke type. The overall prevalence rate in those ⩾ 18 years was 1.7%. The male/female ratio was 0.92. Young (<45) stroke prevalence was found to be 0.6%.
Conclusion:
This study was the first of its kind to show the stroke prevalence among Turkish population ⩾ 18 years in a rural area of Istanbul. When compared to other studies which investigate people ⩾45 years from Turkey, the result (in the same age group) was moderate high. The male/female ratio was low compared to many other studies.
Introduction
Stroke is the proven second leading cause of death as well as disability among adults globally. 1 The impact of stroke is predicted to increase in the future, and cerebrovascular diseases will remain an important cause of mortality in the future.2,3 5%–10% of stroke incidents occur in those under 50-year olds. 4 In Europe and the United States, stroke incidence in young adults is varies from 5.8 to 11.4/100.000.5–10
Epidemiologic studies about stroke are very rare in Turkey. There are only three published studies until now. They reported the stroke prevalence between 0.9% and 4.1% above 44-year-old Turkish population.11–13 However, the young stroke prevalence is still unknown.
As it is well established, incidence and etiology in young adults differ notably from those seen in older patients. So, we aimed to enlighten the prevalence rate among those ⩾18 years in Şile, Istanbul, a town located by the Black Sea coast.
Material and methods
This study was carried out as a cross-sectional field study. The study was approved by the Dr. Lütfi Kırdar Kartal Training and Research Hospital Ethics Committee. In addition, permission was granted by the Şile Public Health Center. Verbal consent was obtained from individuals during the screening survey.
The characteristics of Şile
Şile is a town connected to the city of Istanbul. It is 60 km from Istanbul. It is located in the most western part of the Black Sea coast at 41°10′ north latitude and 29°36′ east longitude. According to the 2012 census, district of Şile has a population of 13,260. A proportion of this population consists of those visiting from Istanbul for their summer vacation. These people stay in Şile during the summer holiday, which is between May and August. According to the Şile Health Minister and Mayor of Şile, the winter population of Şile is around 7500. Despite the summer residents being registered with the town, they actually live in Istanbul. Homogeneous Turkish people live in Şile. They are the Manav branch of the Oğuz (Turkmen) tribes. The main form of employment is farming and small-scale local tourism. Şile is neither a home to any pollution causing factories nor does it have any noticeable pollution. 14
Sample size calculation
Sample size was calculated to be about 2906 with a confidence level of 99% and ±2% margin of error. We visited one in every three households until we reached 2906 persons ⩾18 years.
Data collection
The research protocol created by World Health Organization (WHO) for developing countries was used. 15 The questionnaire was used in the survey after validation in a pilot study which was conducted on 27 stroke patients in our clinic (sensitivity of 85.7% and specificity of 99%). The questionnaire consisted of 13 questions; participants were asked whether they had ever been diagnosed with cerebrovascular disorders by a doctor, whether or not they needed help with day-to-day activities, and whether or not they had had a stroke in the last 6 months. The following risk factors were also asked in the second section of the questionnaire. The presence of a high blood pressure diagnosed by a doctor, the presence of diabetes diagnosed by a doctor, the presence of coronary artery disease or other heart diseases (atrial fibrillation, congenital heart disease, congestive heart failure, and valvular diseases) diagnosed by a doctor, the presence of a hyperlipidemia diagnosed by a doctor, whether or not they consume alcohol more than once a week, and whether or not they were currently a smoker. The survey was filled in accordance with participants’ answers. Participants’ age, sex, stroke type, and risk factors were recorded on the form.
We organized two teams each consisting of five surveyors, a local nurse, and a neurologist from the Dr. Lutfi Kırdar Kartal Training and Research Hospital. Teams were trained on diseases and questionnaire completion on the first day.
The survey was undertaken door to door and face to face. In the event that the participant was unable to answer the questions, a relative answered in their name. Any doors left unanswered were re-visited the following days. The survey was conducted between 1 March and 30 March 2013 just before the summer holiday season in order to screen only native people.
Case ascertainment
Cases were ascertained by self-report with confirmation by clinical examination by a neurologist. Stroke criteria were derived from WHO and MONICA project.16–18 All participants who claimed to have suffered a stroke which had been diagnosed by a doctor were confirmed by neurologist in the field. Stroke is defined as rapidly developing clinical signs of focal or global disturbance of cerebral function lasting more than 24 h, with no other apparent cause other than a vascular origin. 18 In addition, any laboratory, computerized tomography and magnetic resonance imaging (MRI) findings were examined and used as evidence. Similarly diagnosed risk factors were also recorded.
Statistical analysis
Statistical analysis was performed using PASW Statistics 18.0 software. Frequency distribution, percentage, mean, and standard deviation were calculated. To assess the relationship of risk factors of stroke (hypertension, diabetes mellitus, heart disease, hyperlipidemia, alcohol consumption, and smoking), logistic regression analyses were used. The dependent variable was the presence or absence of stroke. The independent variables were divided as present versus absent. Comparison of prevalence rates were conducted with chi-square tests. Results were considered to be statistically significant at the level of p < 0.05.
Results
A total of 2906 (87.5%) people out of 3320 were screened. 414 people refused to participate. Their ages ranged from 18 to 95 years. Their mean age was 46.7 ± 16.7. 1394 (48%) of participants were male and 1512 (52%) were female. In total, 50 people were found to have suffered a stroke. 24 were male, 26 were female. 4 patients had suffered recurrent stroke. The male/female ratio was found to be 0.92. We determined 9 young (age < 45 years) stroke cases. 3 were male and 6 were female.
Our study showed that the prevalence rate of stroke in ⩾18 years in the Turkish population was 1.7%. Young stroke prevalence in < 45 years was found to be 0.6%. The stroke prevalence rate among those ⩾ 45 years was found to be 2.9%. Age-specific prevalence rate of stroke is shown in Table 1.
Age-specific prevalence rates in 2906 participants.

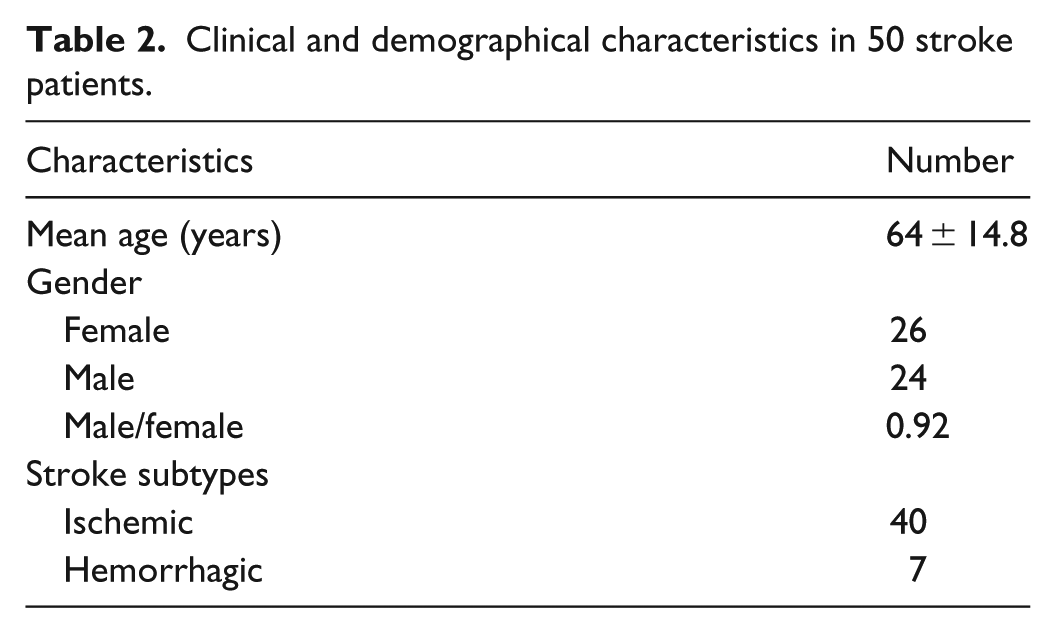
The age range of stroke patients was 35–95 years, and the mean age was 64 ± 14.8 years. Ischemic stroke was found to be 80%, and hemorrhagic stroke was found to be 14%. The stroke type in 6% of patients was unknown. Clinical and demographical characteristics are shown in Table 2.
Clinical and demographical characteristics in 50 stroke patients.
Among young stroke patients, one patient had suffered hemorrhagic stroke (11.1%) due to hypertension and the others were ischemic stroke (88.9%) cases. Cervical artery dissection is seen in two out of eight patients (25%) and small-vessel disease is seen in two patients (25%). One patient (12.5%) had large-artery atherosclerosis. Other three cases (37.5%) had unclassified etiology.
Risk factors
Among all participants of the study, 684 (23.5%) persons had hypertension, 351 (12.1%) were diabetic, 273 (9.4%) persons had heart disease, 323 (11.1%) persons had hyperlipidemia, 926 (31.9%) persons were current smokers, and 196 (6.7%) persons consumed alcohol regularly. Risk factors of participants are shown in Table 3.
Risk factors of participants.

PR: prevalence rate.
Stroke was not seen in anyone under the age of 30. The highest percentage (5.6%) was seen in the 70–79 years age group. Among stroke patients, 39 (78%) had hypertension, 19 (38%) had diabetes mellitus, 19 (38%) had heart disease, 22 (44%) had hyperlipidemia, 16 (32%) were smokers, and 9 (18%) consumed alcohol regularly. Hypertension, diabetes mellitus, heart disease, hyperlipidemia, and alcohol consumption were significantly associated with risk of stroke (p = 0.000, p = 0.000, p = 0.000, p = 0.000, p = 0.001, respectively, chi-square test). Smoking was not found to be significant (p = 0.979).
Among young strokes, proportions of risk factors were smoking (88.9%), hypertension (66.7%), diabetes (44.4%), consuming alcohol (33.3%), and hyperlipidemia (22.2%).
Discussion
This community-based study is the first study showing the young and old stroke prevalence both, conducted in a rural area of Istanbul, Turkey. We recorded a moderate high prevalence of stroke in rural area. The prevalence rate in this study was higher than the prevalence rate of stroke above 44-year olds from Denizli and lower than Karabük city. The prevalence rate of stroke increased with age. The highest prevalence rate was recorded in the seventh decade. Stroke was not noticed in <30 years. Ischemic stroke was more common in general. It is much more common in young patient group. The female/male ratio was almost equal. However, there is a female dominancy in our young stroke patients. Cervical artery dissection and small-vessel disease were only seen in young patients group. There was no recurrent stroke case in young patients group.
Etiologies of young stroke cases are different and could be more complicated than older patients. Putaala et al. 19 reported that, in a 1008 young stroke cohort, cardioembolism (20%) and cervicocerebral artery dissection (15%) were the most frequent etiologic subgroups whereas small-vessel disease (14%) and large-artery atherosclerosis (8%) were seen less. Etiology was undetermined in 33% of patients.
When looking other studies from Turkey, there is a similar study which was carried out by our clinic in Karabük city center in 2014. On a total of 3131 people aged ⩾45 years, the results indicated a slight higher prevalence rate (4.12%) (p = 0.34, chi-square test). 11 This rate is most possibly due to the risk factors (hypertension, diabetes, hyperlipidemia, and heart disease), which are higher in Karabük. Another possible reason for this difference could be that Şile is an unindustrialized rural area without environmental pollution. 14 Karabük city is home to an iron and steel factory built in 1937 which continually emits air pollution. A pollution level exceeding the WHO threshold has been recorded. 20 A study which investigated air pollution in Karabük by Cansaran-Duman and colleagues21,22 showed that the high accumulation of trace elements caused DNA variation in Lichens.
Recent studies show the effect of air pollution on stroke prevalence. One study recorded the association between high PM2.5 levels and an increased stroke risk. Furthermore, Maynard et al. noticed the relationship between the traffic pollution particles and stroke. These results support the previous studies which suggest air pollution may increase ischemic strokes.23–26
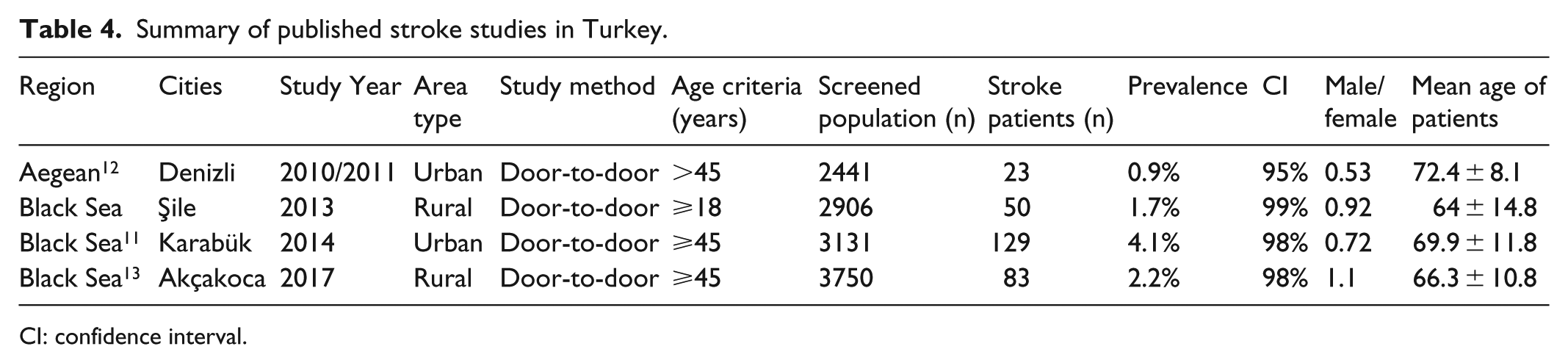
The prevalence rate of stroke in Turkey and the Middle East are not well known. A study from Turkey carried out in 2011, in Denizli located in the Aegean region was the form of a cross-sectional door-to-door survey. Over 44-year-old Turkish population were screened, and the prevalence rate among 44-year olds was found to be 0.9%. 12 Their prevalence rate is much lower than the rates in Karabük and in Şile (p < 0.0001, chi-square test). Another possible reason could be Mediterranean diet and other unknown factors. Recent studies indicate that the Mediterranean diet lowers the risk of stroke. 27 The prevalence rate of the study carried out in Turkey has been summarized in Table 4.
Summary of published stroke studies in Turkey.
CI: confidence interval.
The highest stroke prevalence is seen in ⩾75 years in three cities. Age distribution of stroke in three cities has been shown in Table 5.
Prevalence rate of stroke in three cities according to age.
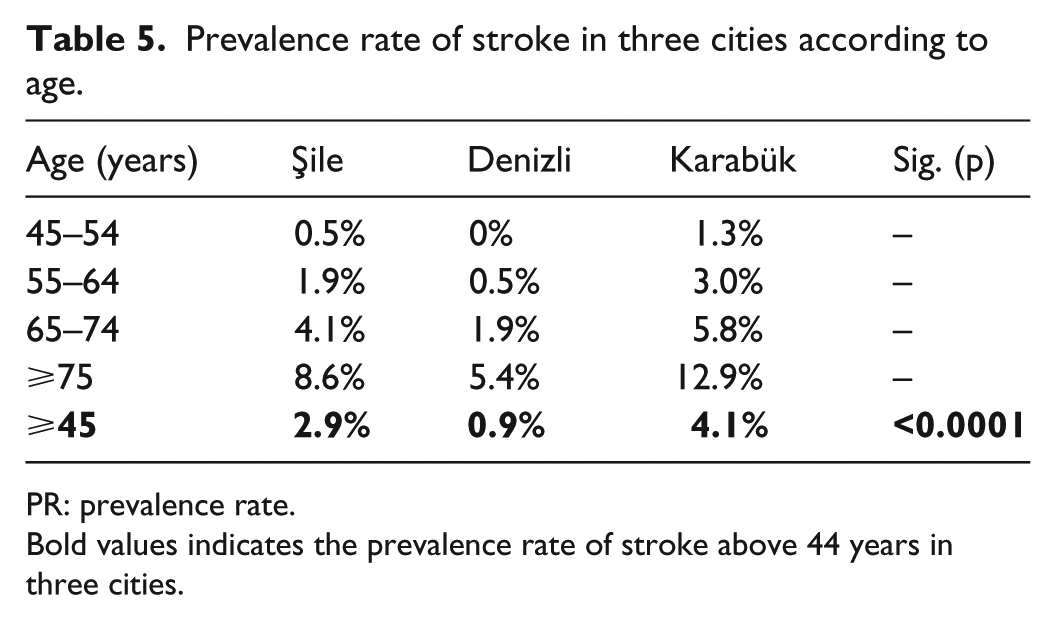
PR: prevalence rate.
Bold values indicates the prevalence rate of stroke above 44 years in three cities.
A comparison of our results with that of the young stroke prevalence rate of Turkish population is not possible because up until now there have been no such studies carried out. Stroke prevalence rates of our neighboring countries are also limited. There are two studies based in Greece, conducted in 1989. One study was a cross-sectional study, carried out in a rural area in the north west of Greece and showed a 0.99% prevalence rate among residences over the age of 20. The other study, carried out in urban area, recorded a prevalence rate of 1.4% over 22-year olds. 28 As these studies are very dated, it is highly possible that new prevalence rates in these areas could be significantly higher.
A study carried out in other Mediterranean country Italy, in over 15-year olds, recorded an overall crude prevalence of 0.14% and 0.47% in over 65-year olds. 29 In a review illustrating studies conducted in Spain, crude stroke prevalence among over 70-year olds was found to be 6.7%. 30
Due to possible factors such as varying methodology, case ascertainment, age distribution, and lack of studies from Turkey and neighboring countries explaining this difference, it is not possible to make a comparison with such studies.
Our male/female rate is almost equal as was the case in the previous Turkish study in Denizli. Male/female ratio in most Western and Asian countries shows a much higher prevalence among males than females.30–33 The reason for this is unclear, but when we evaluated the risk factors of participants in our study; hypertension, diabetes, and hyperlipidemia are more common among females than males. However, smoking and alcohol consumption are more common in males as expected in Turkish tradition. Turkish women rarely smoke and very rarely consume alcohol in general.
Limitation of the study
A limitation of the study is that, fatal stroke events, minor strokes and those which may have been left undiagnosed could result bias. In addition data are limited for young cases. They were not investigated for clotting abnormalities or vasculitis. Another limitation is that silent infarcts and asymptomatic small-vessel disease could not be detected in our methodology. Furthermore, old stroke cases may create a recall bias. Despite participation rate was passable, people who refused to participate is also a limitation.
Strengths of the study
The main strength of the study is that it was a cross-sectional study carried out door to door. There is an important weakness in prevalence studies conducted according to medical records in both Turkey and developing countries, due to a lack of compulsory enrollment at clinics in the patients’ local area. It is possible for patients to seek treatment at multiple centers. In addition to this, bed bound patients may not be able to even visit a hospital and may not have up to date medical records.
The second strength of the study is that self-reported stroke cases were confirmed by clinical examination and laboratory and radiological findings by the assistant neurologist on site.
In conclusion, the study has shed light on the stroke prevalence rate in Turkey. In addition, we have documented the young prevalence rate in Turkey for the first time.
Footnotes
Acknowledgements
The authors thank their colleagues from the Şile Public Health Center who provided insight and expertise that greatly assisted their research. The authors thank Jessica Wells for language assistance and the locals for their high level of participation in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Local Ethics Committee of the Dr. Lütfi Kırdar Kartal Training and Research Hospital.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from all subjects before the study. Ethics committee accepted verbal consent as valid.