
Abstract
Hydatidosis is a zoonosis, caused by a cestode (Echinococcus). Management will depend on the organs affected by the infection and the response to medical treatment. Therapy may be clinical in early stages, but in case of poor response to drug therapy, surgery is the preferred choice. We present two cases in young females, the first case is with Hydatid cysts in both lungs and liver, she received initial medical treatment with lack of response, and surgery was indicated to resect the pulmonary and hepatic lesions. The second case is of a female with Hydatid cysts in the right lung. She was misdiagnosed at the beginning thinking of pneumonia and pulmonary abscess but after further investigation, hydatid cysts were the diagnosis, due to symptoms consistent with thoracic pain and persistent cough and the size of the cyst, surgery was indicated.
Introduction
Hydatidosis is a disease caused by a parasite, that may affect vital organs. It is common in countries with agricultural and livestock areas and temperate climates. 1 The treatment may be medical or surgical; this will depend on the clinical evolution of the patient and radiologic criteria. We present two cases, the first one of a young lady with cysts located in both lungs and liver. She initially received medical treatment with albendazole (ABZ), unfortunately, no response was evident based on radiological control studies which showed progression of the disease. She underwent surgical resection of the pulmonary and hepatic lesions, pathology studies revealed hepato-pulmonary hydatidosis. The second case is of a woman with hydatid cysts (HC) located in the right lung initially she was treated for pneumonia with pulmonary abscess but after looking for a second opinion and exhaustive investigation HC was the diagnosis; due to her symptoms and the size of the lesion she was referred for surgical resection.
Case 1
Patient is a 30-year-old female, with a history of systemic lupus erythematosus treated with corticosteroids, hydroxychloroquine, and rituximab 5 years ago, a journey to Spain previously and no family history of other pathologies. She presented an 8-month history of chronic cough and hemoptysis, so she decided to visit a doctor.
On clinical evaluation, physical findings were negative, but with the history and symptoms, her physician requested radiological studies revealing two lesions on both lungs (Figure 1(a)). A computed tomography (CT) showed the presence of round cystic lesions, with defined contours in the lower pulmonary lobes and a cystic image in the liver; one image in the right lung was compatible with “the water lily sign” (Figure 1(b) and (c)).

(a) Two round lesions, left of 3.38 cm, right of 3.71 cm. (b) Two lesions with liquid and solid content. (c) Left lesion with water lily sign.
The patient was initially treated with the suspected diagnosis of HC. Treatment consisted of ABZ for 3 months with no clinical improvement, so a second CT was obtained and the two known pulmonary cystic lesions increased in size and progressed to solid lesions (Figure 2(a) and (b)), the one in the right lung was 3.5 cm and one in the left lung was 4.2 cm, the lesion in the liver was unchanged (Figure 2(c)).

(a) Two solid lesions. (b) Increase in size of the lesions compared to previous studies. (c) Round lesion located in the anterior wall of the liver.
Due to lack of response to medical management, surgery was recommended.
A bronchoscopy and bilateral thoracotomies were done. The lung lesions were both located in the basal lobes, and no other nodules were found, wedge resection of both lesions with safe margins was made and sent to pathology. Drains were placed and the procedure was completed without complications.
A laparoscopy was continued to resect the liver lesion, and a cystic lesion of 3 × 3 cm (Figure 3(a)) toward segment IV with a thick capsule was found. The lesion was completely resected and sent to pathology (Figure 3(b)).
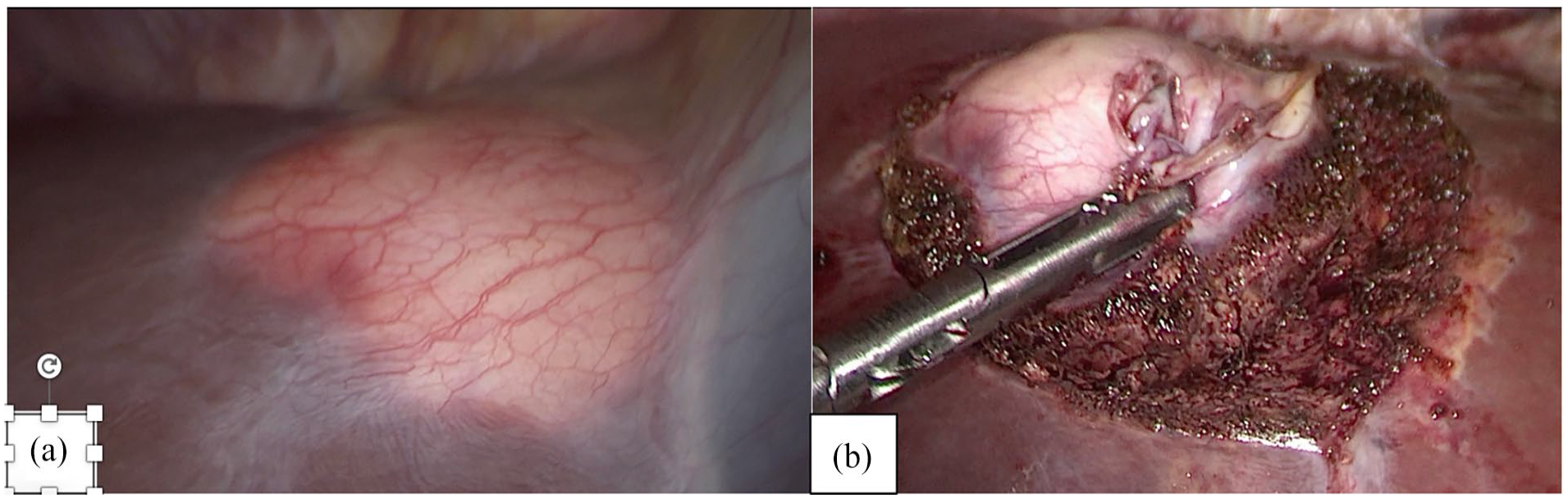
(a) Round lesion located in the IV segment of the liver. (b) Lesion completely resected with free margins.
Pathology studies revealed the presence of cystic echinococcosis in both lungs and liver, with evidence of protoscolices and refractory hooks of echinococcal scolex, highlighted by the Grocott technique; Ziehl-Neelsen and periodic acid-Schiff (PAS) were found (Figure 4(a) and (b)). Pulmonary and liver nodules were completely resected with free margins.

(a) Protoscolices. (b) Hooks of echinococcal scolex. HE 40×.
Her postoperative course was without complications. She was discharged on postoperative day six. She continues with antiparasitic treatment with ABZ to complete 6 months and periodic follow-ups by her primary doctors who sent a control CT showing no recurrence of the cysts (Figure 5(a) and (b)).

(a) No lesions, presence of surgical changes. (b) Surgical changes with no signs of recurrence.
Case 2
Patient is a 34-year-old female, with no previous medical history. She presented back pain and fever for a couple of months. So, she decided to visit a doctor.
On the first evaluation with her physician, the patient had ambiguous clinical findings so it was recommended to do laboratory test, and in a chest X-ray one image in the right lower lobe of the lung was found (Figure 6). She was treated with antifungals thinking the lesion was compatible with aspergillosis, with no response at all. So, the patient decided to get a second opinion.

Round lesion in the lower lobe of the right lung.
The second physician made more in-depth investigations with a CT scan that revealed a round cystic lesion with an air-fluid level in the lower lobe of the right lung compatible with the lesion seen on the chest X-ray (Figure 7). Suspecting echinococcosis immunological test were done and these were positive for echinococcosis. Due to the symptoms of the patient and the characteristics of the lesion surgery was indicated.

Lesion with air-fluid level in the lower lobe of the right lung.
A bronchoscopy followed by a right thoracotomy was done. The cyst was in the basal lobe of the lung, a complete resection of the lesion with safety margins including a partial resection of the parietal pleura was performed. A chest drain was placed, and the procedure was finished without complications.
Pathological studies reported the presence of hooks in the right lung lesion, with the presence of echinococcal scolex (Figure 8). Free margins were reported.

Echinococcal scolex and hooks. HE 40×.
The patient had an adequate post-surgical evolution, she was discharged on the fourth day with appropriate treatment including ABZ. She continues with periodic controls by her physicians.
Discussion
HC is a severe disease that affects different organs in the body and could be potentially lethal, 2 is caused by a zoonotic parasite Echinococcus granulosus.3,4 It is endemic in agricultural and animal-raising communities. 1 The cysts are more commonly present in lungs (10%–40%) and liver (50%–80%). 5
The diagnosis of HC may start with clinical suspicion, like history of contact with animals (dogs, sheep, and cows) or the ingestion of their meat.1,6 But there are two presentations. 1 Asymptomatic which are diagnosed incidentally by routine X-ray. 1 Symptomatic which normally are the ones with cysts bigger than 5 cm. 1 Larger cysts can cause pain, cough with expectoration or hemoptysis, and less common spontaneous anaphylaxis (If the cyst ruptures).7,8 Our second patient had persistent cough and chest wall pain. After clinical suspicion imaging tests, like chest X-ray and CT, showing “the water lily sign”, 3 and laboratory tests normally immunological ones must be taken to have a conclusive diagnosis. 8 The definitive diagnosis is made with histopathological study, using different techniques like the Grocott technique, Ziehl-Neelsen, and PAS. 9
Hydatidosis could be managed medically or surgically 10 as it was done in our patients. Medical treatment is done using benzimidazoles which could be mebendazole or ABZ.4,11 The usual time of treatment could be from 3 months to 2 years. The normal dose of ABZ is 10 to 15 mg/kg/d (taken twice daily).1,11 In cases where surgery is not possible the recommendation is the use of ABZ for 2 years as a palliative treatment. 4
Surgical treatment is the choice in developing countries because it gives a definitive management and it is also used when medical treatment fails. 1 The primary goals of surgery are removing the parasite completely, to approach an R0 (R0, no parasitic residue; R1, microscopic parasitic residue; and R2, macroscopic parasitic residue) 4 and preserve as much parenchyma of the affected organs. 11 After surgery the morbidity ranges are between 6.5% and 39% which is higher in complicated cysts. 1 The mortality is between 0% and 2.3%. 1 Always after surgery drug therapy must be continued with benzimidazole drugs.4,6,12 Both of our patients continue to receive medical therapy.
When facing hydatidosis treatment must be aggressive to have a good prognosis. 12 And these cases must be managed by a multidisciplinary team, to avoid or limit any possible damage from this pathology and its management. The primary goal is to take good care of the patient. 13
Conclusion
HC treatment will always be something complex even with all the tools to perform it. Now, the definitive management described is surgery, accompanied by chronic antiparasitic treatment. More studies and guidelines must be carried out. Management by a team of several specialists should always be carried out to achieve a complement to what the surgeon does.
Footnotes
Acknowledgements
None.
Author contributions
S.A.E.A and D.S.N.C. wrote the manuscript; S.A.E.A and G.A.D.D performed the thoracic surgery; F.I.S.L and M.L.C performed the laparoscopic surgery; C.M.D.V., L.M.R.A., M.M.B.M. and P.M.C.F. participated in the conception of the study; and all authors contributed to the analysis, interpretation, and discussion of the data; all authors reviewed and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series. Within the policies of publication of scientific works of the Hospital Metropolitano, approval by the Ethics Committee is not required for the publication of descriptive works such as this case report.
Informed consent
Written informed consent was obtained from the patient for the anonymized information to be published in this article. Hospital Metropolitano, being a teaching hospital, as part of its policies requires written informed consent from patients about the publication of anonymous information from medical records for purely academic purposes as was in this case report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.