
Abstract
Objective:
Endometrial polyps are localised growths of endometrial tissue containing glands, stroma and blood vessels, covered with epithelium. The reported prevalence of endometrial polyps is dependent upon the population being studied and the uterine imaging technique utilised. The light microscopy literature provides very little information regarding their microvasculature and lymphatic systems; however, a plethora of ultrasound data demonstrating single central arteries in most medium- or large-sized endometrial polyps are well documented.
Methods:
Archived formalin-fixed paraffin-embedded blocks of endometrial curettings were retrieved from files for women with confirmed endometrial polyps (n = 20) and women with normal endometrium (control endometrium; n = 32). Immunohistochemistry was performed with the antibodies CD31 (blood vessels) and D2-40 (lymphatics). Blood vessels and lymphatics were quantified in endometrial polyps and adjacent, distant and control endometrium.
Results:
CD31 and D2-40 staining was present in all specimens, although there were no significant differences in blood vessel (F(3,70) = 2.36, p = 0.079) and lymphatic (F(3,70) = 0.16, p = 0.920) densities between endometrial polyps as well as adjacent, distant and control endometrium. There were also no significant differences in women with endometrial polyp-associated bleeding and those with no bleeding. In relation to infertility, there were no significant differences found in blood and lymphatic densities between women with endometrial polyps who were infertile and those with endometrial polyps who were fertile.
Conclusion:
Small blood vessel wall and perivascular structures rather than the distribution of vessels may be associated with abnormal bleeding.
Introduction
Endometrial polyps are outgrowths of the surface epithelium and stroma of the endometrium. 1 Endometrial polyps are common, mostly benign lesions that are pedunculated or sessile. They are typically solitary, although 20% of endometrial polyps occur in multiples. 2 They can be found at any age in the reproductive or postmenopausal phase of life. 1 It is difficult to determine the true prevalence of endometrial polyps, as most of them are asymptomatic lesions. When polyps are symptomatic, heavy bleeding and/or spotting usually accompany them. However, many endometrial polyps are believed to be the source of bleeding only when the tip is necrotic, gangrenous or hemorrhagic. 3 Originally, inflammation was believed to be the main etiologic factor, yet most endometrial polyps are free of evidence of infection. 3
Utilising two-dimensional sonograms, sonohysterography or hysteroscopy, endometrial polyps have been reported in 50% of women with a history of postmenopausal bleeding, 4 in 13% of perimenopausal women with abnormal uterine bleeding 5 and in 16.5%–26.5% of women with unexplained infertility. 6 Furthermore, women suffering from infertility with associated endometriosis have a higher rate (46.7%) of endometrial polyps. In contrast, women with a recurrent pregnancy loss have a lower rate (0.6%–5%) of endometrial polyps. 7 Post polypectomy, pregnancy rates improved twofold in intrauterine inseminated patients. 8 Hysteroscopic polypectomy increased pregnancy rates and ultimately improved fertility in women who were previously infertile with no known causes. 9
No differences in endometrial blood vessel density have been reported when cases of women with unexplained infertility were compared to those with normal endometrium. 10 However, the eutopic endometrium of women with endometriosis accompanied by infertility was found to have an increased density of blood vessels when compared to normal endometrium. 11 This may mean that the density of blood vessels in endometrial pathologies may be linked with infertility.
The malignant potential of most endometrial polyps is generally low; however, there may be risk factors leading to endometrial cancer. The detection of malignancy in endometrial polyps has varied between 0.5% and 4.8%. 12 In combination, obesity associated with hypertension seems to be a significant factor and may be involved in the pathogenesis of endometrial polyps, similarly to late menopause, found in 30% of postmenopausal women. 1 Furthermore, there is a positive association of increased body mass index, hormone replacement therapy (HRT) and endometrial polyps. 12
Hysteroscopic polypectomy is recommended as the optimal treatment for the removal of endometrial polyps. Removal of the endometrial basalis at the endometrial polyp origin appears to prevent further recurrences. 1 Polypectomy by surgical treatment results in high satisfaction rates and a decrease in bleeding symptoms. Satisfactory outcomes following polypectomy appear to be independent of menopausal status and size and number of polyps. 13 However, the diagnosis of endometrial polyps is often missed as there may be fragmentation of the specimen during curettage, or focal gland dilatation may be over-interpreted as simple endometrial hyperplasia. 3
The aims of the study were as follows:
To quantify the blood vessel density of endometrial polyps and adjacent and distant endometrium using immunohistochemistry and monoclonal mouse anti-human CD31 endothelial cell clone;
To quantify the lymphatic density of endometrial polyps, adjacent and distant endometrium using immunohistochemistry and monoclonal mouse anti-human D2-40 which react with the lymphatic endothelium;
To demonstrate that the blood vessel and lymphatic densities are not affected by the menstrual cycle;
To demonstrate that both the blood vessel and lymphatic densities of endometrial polyps are influenced by abnormal bleeding and infertility.
Materials and methods
Collection of tissue
This study was approved by the committees of the Sydney Local Health District – Royal Prince Alfred Hospital (SLHS RPA), Research Ethics and Governance Office, and Human Ethics – The University of Sydney (Protocol No. X13-0342 & HREC/13/PRAH/470 – ‘Blood and lymphatic vessel densities in human endometrial polyps’). Archived formalin-fixed paraffin-embedded (FFPE) endometrial blocks were retrieved from histological filing within the Department of Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Camperdown, Australia. Hysterectomy blocks retrieved from women with a histologically confirmed diagnosis of endometrial polyps included adjacent and distant endometrium from the same women (Table 1). For control tissue, FFPE blocks of hysterectomy control samples with no evidence of endometrial polyps in either the adjacent or distant endometrial samples or histopathology reports were also retrieved with ethical approval (Table 2).
Hysterectomy blocks retrieved from women with a histologically confirmed diagnosis of endometrial polyps, including adjacent and distant endometrium from the same women.

FFPE: formalin-fixed paraffin-embedded.
Hysterectomy control samples with no evidence of endometrial polyps in either the endometrial samples or histopathology reports.
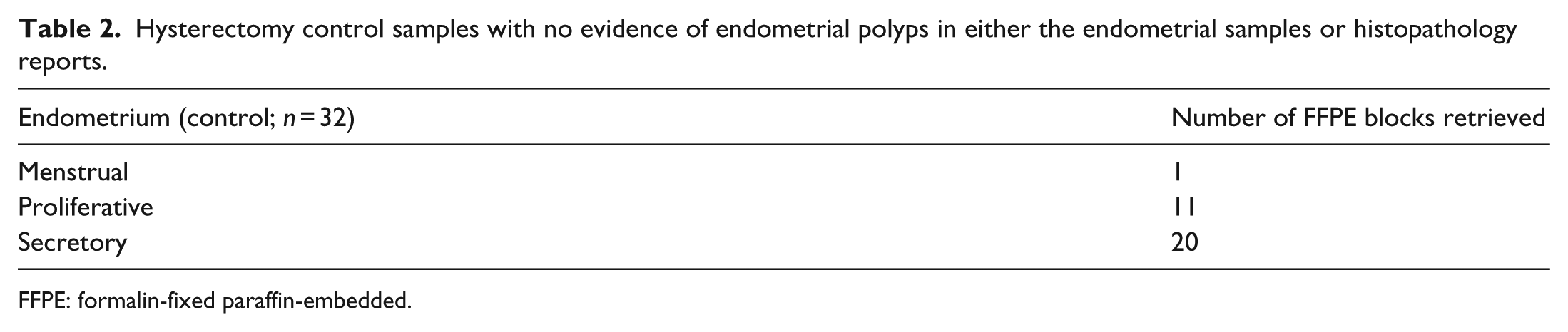
FFPE: formalin-fixed paraffin-embedded.
All endometrial and control samples had their menstrual cycle staging determined by histopathologists within the Department of Tissue Pathology and Diagnostic Oncology Department, Royal Prince Alfred Hospital using Noyes criteria. 14
A priori sample size calculation was not performed since the associations explored were novel. Consequently, we were unable to estimate effect sizes based on other data.
Exclusion criteria
None of the women had received hormonal treatment for the last 3 months prior to endometrial hysterectomy sampling.
Histopathology
Serial sections were cut at 4 μm, dried at 60°C for 1 h and routinely stained with haematoxylin and eosin (H&E).
Immunohistochemistry
Deparaffinised slides for immunohistochemical staining underwent heat antigen retrieval for 20 min in pre-heated 100°C Dako EnVision™ Flex Target Retrieval Solution pH 9.0 (K8023, DakoCytomation, Carpinteria, CA, USA). Slides were cooled for 45 min and then placed in a Tris-buffered saline (TBS) bath for 10 min.
Immunohistochemical staining was performed using the Dako Autostainer Model S3400 (DakoCytomation). A 3% hydrogen peroxide solution (DakoCytomation) was applied for 10 min followed by 30-min incubations with the primary antibodies monoclonal mouse anti-human CD31, endothelial cell clone, JC70A and M0823 (1:400) and monoclonal mouse anti-human D2-40, clone D2-40 and M3619 (1:50), and then incubated for 30 min with the detection system EnVision + Dual Link System-HRP K4061 (DakoCytomation). The reaction was visualised with a 10-min incubation of liquid DAB + Substrate Chromogen System K3468 (DakoCytomation). Slides were counterstained with Mayer’s haematoxylin and cover-slipped.
Quantification
Each slide was examined at ×200 magnification and images captured with the use of an Olympus BX51 microscope and a DP70 digital camera with DP controller and DP manager (Olympus Optical Co., LTD, Tokyo, Japan; Figure 1(a)–(h)). Assessments of blood and lymphatic densities were performed on 15 non-overlapping images where possible.

(a)–(h) Immunohistochemical staining of CD31-positive blood vessel structures: (a) endometrial polyp, (b) adjacent endometrium, (c) distant endometrium and (d) control endometrium; D2-40-positive lymphatic structures: (e) endometrial polyp, (f) adjacent endometrium, (g) distant endometrium and (h) control endometrium.
Blood and lymphatic vessels were counted manually for each image taken by two independent observers (N.P.N., F.M.) without knowledge of the phase of the menstrual cycle or other clinical parameters. Concordance between the two observers was calculated for the average of all fields of view.
The interclass correlation coefficients (ICCs) for inter-rater reliability were good. For polyp blood vessel density, the ICC was 0.994 (95% confidence interval (CI) 0.985–0.998; n = 20, p < 0.001), for adjacent endometrium 0.989 (95% CI 0.972–0.996; n = 8, p < 0.001), for distant endometrium 0.993 (95% CI 0.978–0.992; n = 14, p < 0.001) and for control endometrium 0.990 (95% CI 0.991–0.996, n = 32, p < 0.001).
The ICC for polyp lymphatic density was 0.991 (95% CI 0.993–0.998; n = 17, p < 0.001), for adjacent endometrium 0.986 (95% CI 0.981–0.993; n = 7, p < 0.001), for distant endometrium 0.996 (95% CI 0.987–0.995; n = 13, p < 0.001) and for control endometrium 0.993 (95% CI 0.991–0.997; n = 31, p < 0.001).
Statistical analysis
Results were expressed as mean (M) ± standard deviation (SD) numbers per mm2. Statistical analyses were performed with the use of SPSS version 17 (SPSS Inc., Chicago, IL, USA). The distribution of blood vessel and lymphatic densities was examined with the use of the one-sample Kolmogorov-Smirnov test. Since the density data did not deviate significantly from normality, one-way analysis of variance (ANOVA) tests were used to compare the mean vessel densities between all the ‘groups’ (polyp, adjacent, distant and control tissues). Post hoc Bonferroni contrast tests were used for pairwise comparison of the groups. Paired-samples t tests were used to compare matched tissues (e.g. polyp vs adjacent tissues from the same women). Independent-samples t tests were used to compare the various groups across the menstrual cycle (proliferation and secretory phases) and to compare the relationship between mean blood vessel densities (MBVDs) and mean lymphatic densities (MLDs) and the presence or absence of abnormal bleeding or infertility. Alpha was set at 0.05 for all analyses.
Results
Both CD31- and D2-40-stained structures were found to be normally distributed because their p values were significantly higher than 0.05 (p = 0.351 for CD31; p = 0.139 for D2-40) indicating that the data did not deviate significantly from a normal distribution. Therefore, the M and SD values were used as the parameters to compare between the different groups. The SDs of both blood vessel and lymphatic densities were very large, indicating that the measurements of data were highly variable from sample to sample.
Comparison of MBVD and MLD between the polyp and adjacent, distant and control endometrium groups
There were no significant overall differences between the groups in terms of average endometrial polyp or endometrial functional layer blood vessel density count (F(3,70) = 2.36, p = 0.079; Table 3). There were no significant differences with pairwise comparisons of blood vessel density (polyp vs adjacent, polyp vs distant, adjacent vs distant and adjacent vs control each p = 1.00; polyp vs control p = 0.27; distant vs control p = 0.17). For tissues from women with polyps, secretory MBVDs were consistently lower than proliferative MBVD; however, there were no statistically significant differences (polyp p = 0.15; adjacent p = 0.27; distant p = 0.53). The MBVD was higher during the secretory phase among the control samples; however, this difference was not statistically significant (p = 0.51). There were no statistically significant differences between the MLD in the polyp and adjacent and control endometrium (F(3,70) = 0.16, p = 0.920; Table 4).
One way ANOVA test used to compare the mean blood vessel density per mm2 presented for polyp, adjacent, distant and control endometrium.

SD: standard deviation.
One way ANOVA test used to compare the mean lymphatic density per mm2 between all the groups (polyp, adjacent, distant and control endometrium).
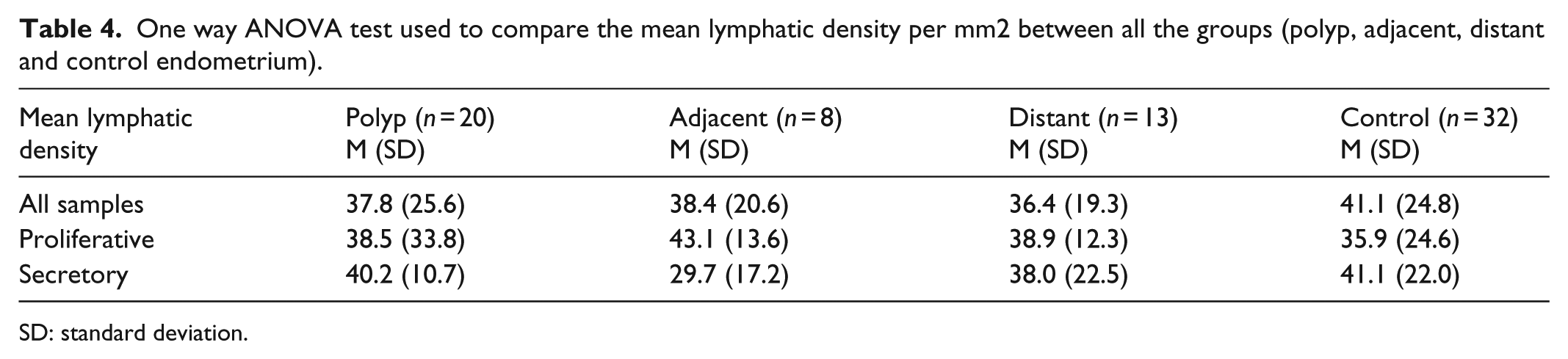
SD: standard deviation.
Comparing the MBVD and MLD between the paired groups polyp–adjacent endometrium, polyp–distant endometrium, polyp–control endometrium, adjacent–distant endometrium, adjacent–control endometrium and distant–control endometrium
Post hoc Bonferroni contrast test was used to compare paired groups (polyp–adjacent endometrium, polyp–distant endometrium, polyp–control endometrium, adjacent–distant, adjacent–control, distant–control). When the paired groups were compared, further analysis did not reveal any significant differences in the MBVD (Table 5). Likewise, there were no statistically significant differences in MLD between any of the paired groups (Table 6).
Comparison of the mean blood vessel densities per mm2 between paired groups.
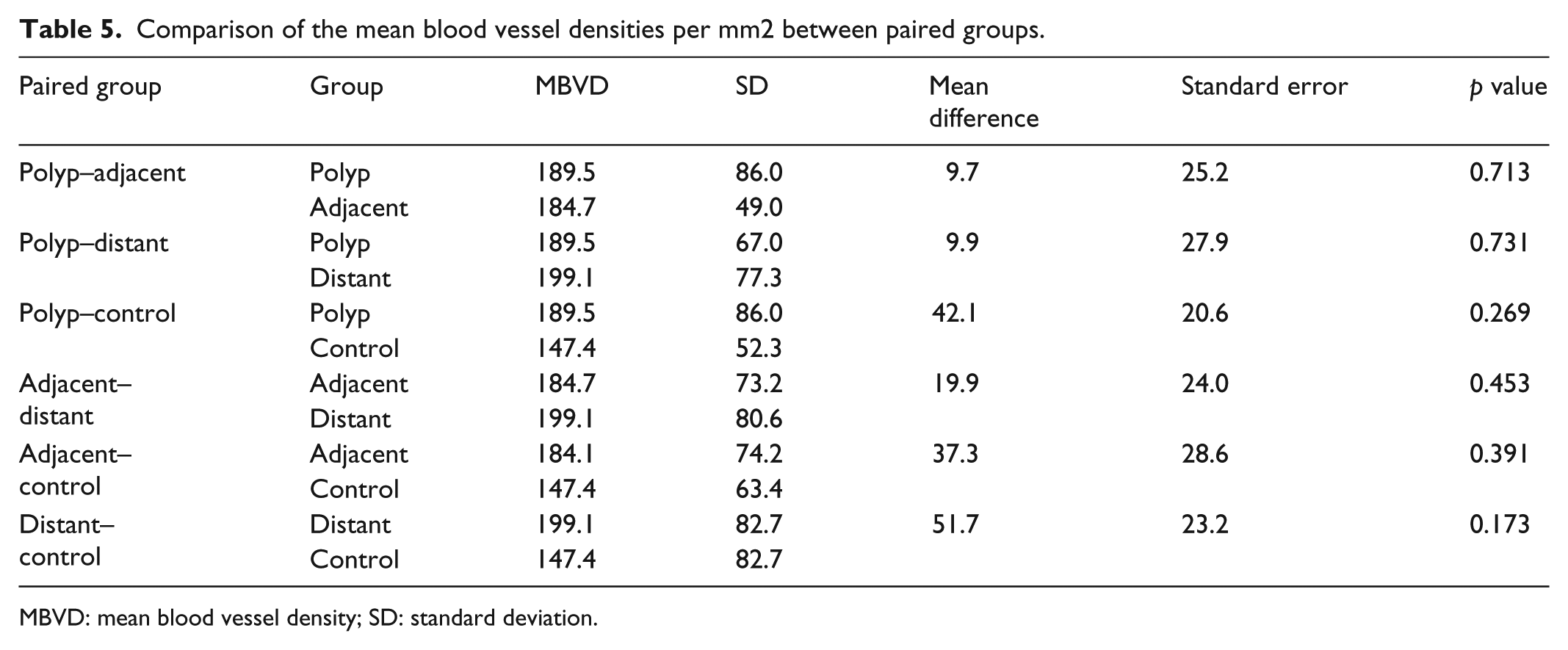
MBVD: mean blood vessel density; SD: standard deviation.
Comparison of the mean lymphatic densities per mm2 between paired groups.

MLD: mean lymphatic density; SD: standard deviation.
Comparing the matched data of MBVD and MLD between polyp and adjacent and distant endometrium
Paired t test was used to compare the matched data of the different groups. There were no statistically significant differences between the MBVD of any of the paired groups with matched data. Likewise, there were no statistically significant differences between the MLD of any of the paired groups with matched data.
Comparison of the MBVD and MLD across the menstrual cycle (proliferative and secretory phases) in the polyp and adjacent, distant and control endometrium groups
Two-sample independent t test was used to compare the MBVD and MLD across the proliferative and secretory phases in the polyp and adjacent, distant and control endometrium groups. There was no statistically significant difference in MBVD between the proliferative and secretory phases of the menstrual cycle in the polyp. The difference of MBVD between the proliferative and secretory phases of the menstrual cycle in the adjacent endometrium was not significant. In the distant endometrium, there were no significant differences in MBVD between the proliferative and secretory phases of the menstrual cycle. No significant difference was found in MBVD between the proliferative and secretory phases of the menstrual cycle in the control endometrium.
There were no statistically significant differences in MLD in the polyp across the menstrual cycle. There were also no significant differences in MLD across the menstrual cycle in adjacent, distant and control endometrium.
Comparison of MBVD and MLD of endometrial polyps and the presence or absence of abnormal bleeding
Two-sample independent t test was used to compare the relationship between MBVD, MLD and the presence or absence of abnormal bleeding. There were no statistically significant differences in MBVD between the polyp samples of women with and without abnormal bleeding. There were no statistically significant differences in MLD between the polyp samples of women with and without abnormal bleeding.
Comparison of MBVD and MLD of endometrial polyps with and without infertility
Two-sample independent t test was used to compare the relationship between MBVD, MLD and the presence or absence of infertility.
There were no statistically significant differences in MBVD between the polyp samples of women with and without infertility. There were also no statistically significant differences in MLD between the polyp samples of women with and without infertility.
Discussion
Endometrial polyps in reproductive-age women are small and sometimes regress completely, while in postmenopausal women, with no physiologic angiogenic influence, they often remain stable with a much higher tendency of becoming malignant with uncontrolled angiogenesis. 15 Endometrial polyps, although mostly benign lesions, have been associated with a high frequency of abnormal uterine bleeding and infertility, yet very little is known about the distribution of their blood and lymphatic microvasculature.
Our observations found that both the blood vessel and lymphatic densities did not change across the menstrual cycle (proliferative and secretory phases). However, there were numerical increases of blood vessel density in polyps, relative to control endometrium. The small polyp sample size compared to control endometrium accompanied by the large SD may have resulted in the non-significant differences of blood vessel densities. There were no significant associations found between endometrial polyp blood vessel and lymphatic densities in either abnormal bleeding or infertility.
Ovarian hormonal influence
Endometrial polyps are made of endometrial glands and stromal cells with some response to ovarian hormones. 16 Ovarian hormones are known to initiate and regulate endometrial angiogenesis. 17 They achieve this through a dynamic balance of both angiogenic and antiangiogenic factors maintaining a constant endometrial blood vessel density during a woman’s reproductive life through vessel growth and regression in a cyclical manner called the menstrual cycle. 18 However, Carvalho et al. 19 reported that most endometrial polyps are non-functional and are unaffected by ovarian hormones that regulate and control endometrial angiogenesis; thus, the blood vessel and lymphatic densities remained relatively unchanged across the menstrual cycle.
Angiogenesis and lymphangiogenesis
Endometrial angiogenesis appeared to have increased in the proliferative phase of the menstrual cycle, where the blood vessels only elongate with no net increase in blood vessel density across the menstrual cycle, 20 Gambino et al. 21 and Manconi et al. 22 , indicating that endometrial polyps that manifest secretory or proliferative changes may be influenced by endometrial angiogenesis and would also have a constant blood vessel density across the menstrual cycle.
In general, angiogenesis and lymphangiogenesis were found to be constant across the menstrual cycle in the adjacent and distant endometrium, and this appearance would be indicative of the complete control by physiologic angiogenesis in the endometrium which is reported to be relatively constant across the menstrual cycle. 20 Numerous studies have demonstrated similar results of constant blood vessel and lymphatic densities in the normal endometrium (basal and functional layers) across the menstrual cycle.20,23,24 However, these findings are not universal and a number of studies have found lymphatic densities higher in the basal layer of the secretory phase, 25 or blood vessel densities higher in the menstrual phase. 26 This constant observation of microvasculature densities across the menstrual cycle are supported by the fact that the endometrial stromal cell (the main substrate for blood vessel and lymphatic structure) proliferation rate has been found to be constant across the menstrual cycle. 27
Abnormal bleeding
Our findings showed no significant differences between endometrial blood vessel and lymphatic densities in the presence or absence of abnormal bleeding. In spite of this, a similar study investigating dysfunctional uterine bleeding (DUB) found that there were no increases in blood vessel densities and that the blood vessels of these women were very diluted and congested when compared to control endometrium. 10
Infertility
No significant differences were found in endometrial blood vessel and lymphatic densities when cases of women with unexplained infertility were compared to control endometrium. In contrast, the eutopic endometrium of women with endometriosis accompanied by infertility was found to have an increased density of blood vessels when compared to normal endometrium. 11 This may imply that blood vessel density in endometrial pathologies may be linked with infertility. Our results showed no significant differences in endometrial polyp blood vessel density in women with and without infertility. The accompanied thickening of the endometrial blood vessels of polyp patients might be the reason for endometrial polyp-associated infertility. 19 It has long been reported that endometrial polyps are characterised by thick-walled blood vessels. 28 From the relationship between lymphatic distribution in the endometrium and fertility, it was found that lymphatics are reduced in the functional layer of the endometrium when compared to the basal layer of the endometrium and completely disappear in the decidua prior to implantation. 29
Limitations of this study
The human endometrium with its unique environment and intricate changes that take place during the menstrual cycle makes it very difficult to study. Even more challenging was obtaining hysterectomy samples of well-characterised endometrial polyps. Endometrial polyps are categorised based on at least two of three alternating traits and are difficult to differentiate from surrounding tissues. Polyps vary greatly between individuals and are often difficult to obtain.
Standardisation
All immunohistochemical staining was completed using the Dako Autostainer system designed to automate manual staining methods, which aided in the standardisation of the staining methods. As a result, immunostaining most likely did not introduce any bias. However, counting areas were chosen randomly and quantification of blood vessel and lymphatic densities was conducted manually with possible human errors. The number of polyp samples stained was small and the poor sample quality reduced the number of stained slides for counting even further. Although there were no statistically significant differences observed in blood vessel and lymphatic densities between endometrial polyps and normal endometrium, there was an obvious trend which would most likely yield a significant result if there was a larger sample size.
Conclusion
Numerical increases of blood vessel densities were observed in polyps relative to control endometrium; however, there were no noticeable differences in lymphatic densities in polyps relative to control endometrium.
Endometrial polyps associated with bleeding may be more related to the structure than the number of blood vessels. Endometrial polyp blood vessel densities did not change across the menstrual cycle because of the unique endometrial angiogenic environment which is able to influence it and prevent any variation. There were no associations found between endometrial polyp blood and lymphatic densities in either abnormal bleeding or infertility. A better understanding of endometrial polyps and their inner mechanisms may provide a greater insight into the development and function of these lesions and open the way for more effective treatments.
Footnotes
Acknowledgements
The authors wish to acknowledge technical support from Mr Lawrence Young (DAKO, Sydney, Australia) and statistical advice from Dr Georgina Luscombe.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Human Ethics Review Committee, Sydney Local Health District, Royal Prince Alfred Hospital (RPAH), and the University of Sydney Human Ethics committee (Protocol No. X13-0342 & HREC/13/RPAH/470 – ‘Blood and lymphatic vessel densities in human endometrial polyps’).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was not sought for this study because of the difficulty of contacting individuals directly when there is no existing or continual relationship between the organisation and the individuals. Formalin-fixed paraffin-embedded archival blocks were used for the study and no identifying information was required.