
Abstract
Introduction:
The major challenge in the HIV epidemic in Georgia is a high proportion of undiagnosed people living with HIV (estimated 48%) as well as a very high proportion of late presentations for care, with 66% presenting for HIV care with CD4 count <350 and 40% with <200 cells/mm3, in 2013. The objectives of this study was to evaluate patient engagement in the continuum of HIV care for HIV patients diagnosed in 2013 and, within this cohort, to evaluate factors associated with late diagnosis and attrition from care.
Methods:
Factors associated with late diagnosis were analyzed through binary logistic regression. Exposure variables were the mode of HIV transmission (injecting drug use, male-to-male contact, and heterosexual contact), gender (male vs female), and age (categorized by median value ≤36 vs >36). In addition, CD4 count at diagnosis (cells/mm3) (≤350 or >350) together with all above factors were tested for the association with attrition through Poisson regression.
Results:
Overall, 317 patients retained in care, representing 65% of those diagnosed (n = 488). Out of eligible 295 patients, 89.5% were on treatment and 84% of those viral load count was measured after 6 months of antiretroviral treatment initiation had HIV-1 viral load <1000 copies/mL. Patients reporting injecting drug use as a route-of HIV transmission had two times the odds (95% confidence interval = 1.34–3.49) to be diagnosed late and patients reporting male-to-male contact as a way of HIV transmission had half the odds (odds ratio = 0.46 (95% confidence interval = 0.26–0.81)) of late diagnosis compared to patients acquiring HIV through heterosexual contact. Patients older than 36 years were more likely to being diagnosed late.
Conclusion:
More attention should be given to injecting drug users as they represent the most at-risk population for late diagnosis together with older age and attrition.
Introduction
The HIV care continuum is a model that outlines the sequential steps of HIV medical care that people living with HIV (PLWHIV) go through from initial diagnosis to achieving viral suppression and shows the proportion/percentage of individuals living with HIV who are engaged at each stage. 1
In order to fully benefit from antiretroviral treatment (ART), patients need to be engaged in regular HIV care and receive the adequate ART. Various barriers contribute to poor engagement in HIV care, limiting the effectiveness of efforts to improve health outcomes for those with HIV and to reduce new HIV transmissions. 2
The major challenge in the HIV epidemic in Georgia is the high proportion of undiagnosed PLWHIV (out of estimated 6400 HIV-infected people, in 2014, 51% were undiagnosed) as well as a very high proportion of late presentations for care, with 66% presenting to care with CD4 count <350 cells/mm3 and 40% with advanced disease (CD4 count <200 cell/mm3) in 2013. 3 A late case detection and consequently treatment initiation at late stages of disease pose significant challenges to the National HIV response in Georgia. This has detrimental effect on survival, resulting in almost 90% increased risk of mortality. 4
Overall, the country has a low HIV prevalence of 12.7 per 100,000 in 2014, in the general population. Population estimates of HIV prevalence, among people who inject drugs (PWIDs), in cities range from lowest 0.4% in Telavi to highest 9.1% in Zugdidi. The percentage of drug use, as a transmission mode among newly registered HIV cases, decreased from 43.2% in 2012 to 35% in 2013 while heterosexual transmission increased from 44.8% in 2012 to 49% in 2013.5–7
Population size estimation studies, conducted in 2014, showed that in Georgia, there are 49,700 injecting drug users, 17,000 men who have sex with men (MSM), and 6500 female sex workers.8–10 Similar to other countries in the region, the epidemic in Georgia has been driven largely by injecting drug use (IDU). 11 However, by 2011, heterosexual contact had become the dominant mode. Many of these infectious are likely linked to IDU.12,13 Dvali et al. 13 demonstrated that there is a genetic linkage between viruses from injecting drug users and heterosexually infected women.
Georgia’s response to the HIV epidemic is supported by the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM). Diagnosed PLWHIV are referred to the Infectious Disease, AIDS and Clinical Immunology Research Center (IDACIRC) in the capital city Tbilisi or one of its three affiliated regional centers in Batumi, Zugdidi, and Kutaisi, where they receive free of charge HIV-related medical services. HIV treatment and care can be received only in these centers. The objective of this study was to evaluate patient engagement in the continuum of HIV care for HIV patients diagnosed in 2013 and, within this cohort, to evaluate factors associated with late diagnosis and attrition from care.
Methods
The study included all individuals diagnosed with HIV in Georgia in 2013. The cohort was followed until 30 June 2015. Data were extracted from the national AIDS health information system (AIDS-HIS). AIDS-HIS collects information on all HIV-positive cases diagnosed in Georgia, including demographic, epidemiological, and clinical and laboratory data. Patients are registered in the database with unique national ID. Currently, the database is a secure web-based system networking all centers that provide HIV care countrywide.
Definitions
The following definitions were used in the data analysis:
HIV diagnosis was defined as positive HIV test result by any method and confirmed by Western blot or nucleic acid–based test;
Linked to HIV care was defined as at least one documented clinical visit (CD4 cell count or HIV-1 viral load (VL) measurement) after HIV diagnosis;
Enrolled in ART was defined as at least one pick-up of combination of at least three antiretroviral (ARV) drugs prescribed for the treatment of HIV infection;
Lost-to-follow-up (LFTU) of those on ART was defined as the last visit earlier than 90 days prior to the end of follow-up period, for any reason;
LFTU of those on HIV care was defined as the last visit earlier than 180 days prior to the end of follow-up period, for any reason;
Viral suppression was defined as plasma HIV RNA level <1000 copies/mL at the most recent measurement up to the end of follow-up period. As a rule, some lapse of time is expected between ART initiation and VL suppression. We used a default time point, and for VL suppression calculation, VL data was measured after 6 months of ART initiation; 6
The term “attrition” refers to all cases of disengagement from HIV care (pre-ART care or ART care) including death and LFTU;
The term “late diagnosis” is defined as having CD4 count ≤350 cell/mm3 at the time of diagnosis;
According to the guidelines used in 2013, eligibility for ART was defined as CD4 count ≤350 cells/mm3.
Statistical analysis
Late diagnosis
Factors associated with late diagnosis were analyzed through binary and multivariable logistic regression. Exposure variables were age (categorized by median value ≤36 vs >36), gender (male vs female), and mode of HIV transmission (IDU male-to-male contact, and heterosexual contact).
First, univariable analyses were performed to assess the strength of the association between each exposure variable and outcome, if they showed statistically significant association (p < 0.005). Other variables were then included in an initial multivariable model if they were associated with the outcome at p < 0.05. Likelihood rate ratio tests (LRT) were used to assess a variable’s contribution to the model’s fit. Results were presented as estimated odds ratios (OR) with corresponding 95% confidence intervals (CI) and p values.
Attrition from care
Factors associated with attrition from care were evaluated using Poisson regression analysis. Time spent in the study was calculated from the point of patients’ linkage to HIV care till the last documented contact. CD4 count at diagnosis (cells/mm3) (≤350 or >350) was tested for the association with attrition in addition to all those variables tested for late diagnosis.
Results are presented as estimated incidence rate rations (IRR) with corresponding 95% CI and p values. All p values are two sided and reported to three decimal place with those less than reported as p < 0.001. Analyses were performed using STATA version 11.
Results
HIV care cascade
In 2013, 490 patients were diagnosed with HIV. Due to missing data, we excluded two patients from the data analysis. The final data set included 488 patients, out of which 90.8% (443/488) were linked to HIV care, and in total, 73.8% (360/488) started ART (Table 1).
Characteristics of the cohort.

ART: antiretroviral treatment.
For one patient, CD4 count at the time of diagnosis was not available.
The median age at diagnosis was 36 years (interquartile range (IQR): 28–44). Quarter of the cohort was female (122 patients). Heterosexual contact, IDU, and male-to-male contact as a route-of transmission was indicated by 49.2% (240/488), 35.2% (172/488) and 13.5% (66/488) of patients, respectively. HIV infection was acquired through mother-to-child transmission in four cases and through blood transfusion in two cases. The mode of transmission of HIV was unknown in only four patients.
Half of the patients were linked to care within 3 days from diagnosis (IQR: 1–9). The median CD4 count at the entry into the care was 241 cells/mm3 (IQR: 104–400). Among patients linked to care, 317 (71%) remained in care and were followed through to the end of the study period (30 June 2015). Out of the eligible (CD4 count≤350 cell/mm3) 295 patients, 264 (89.5%) were on treatment. Out of 264 patients who started treatment, 224 had VL assessed after 6 months of ART and 189 (84%) of those had HIV-1 VL <1000 copies/mL. A total of 95 patients with a CD4 count above 350 cell/mm3 started ART, out of which 82 (86%) measured VL after 6 months of ART initiation and 71 of those measured (86.5%) reached viral suppression (Figure 1).
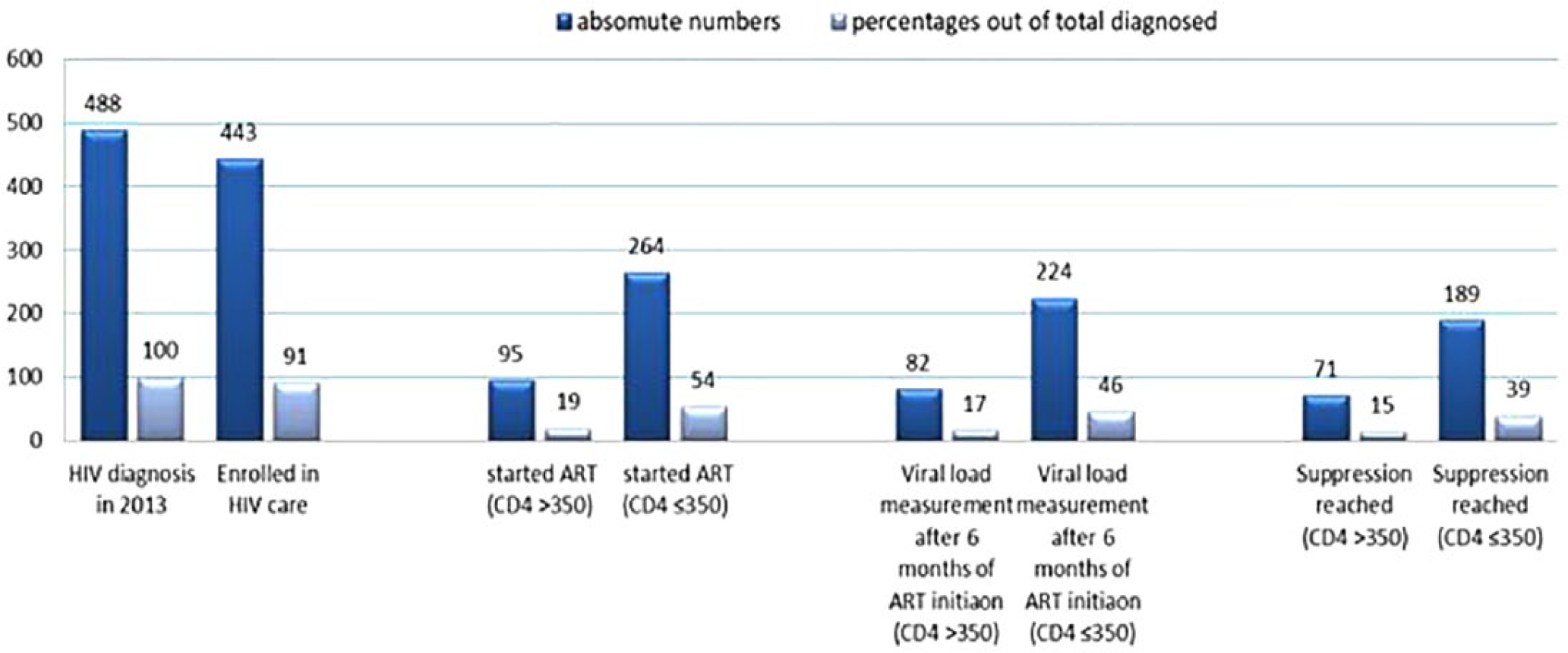
The 2013 HIV cohort cascade (n = 488).
Among patients eligible for ART the following modes of HIV transmission were indicated: injecting drug use in 42% (124/295) of cases, heterosexual contact in 46.8% (138/295) of cases , male-to-male contact in 9.5% (28/295) of cases, mother-to-child transmission in 0.7% (2/295) of cases, blood transfusion in 0.7% (2/295) of cases and unknown reasons in 0.3% (1/295) of cases. In all, 59.3% (175/295) of eligible patients were older than 36 years and 26.1% (77/295) were female.
Among those eligible (CD4 count ≤350) and enrolled in ART, the highest level of VL suppression was found in patients acquiring HIV through male-to-male contact with 77% (20/26), followed by heterosexual contacts with 76% (97/127) and injecting drug users with 65% (69/106) (Figure 2).

Cascade of care: IDU, heterosexual, and male-to-male contacts.
Late diagnosis
Patients reporting the IDU as a route-of HIV transmission had two times the odds (95% CI: 1.34–3.49) to be diagnosed late and patients reporting the male-to-male contact as a way of HIV transmission had half the odds (OR: 0.46 (95% CI: 0.26–0.81)) of late diagnosis compared with patients who acquired HIV through heterosexual contact (Table 2).
Variables associated with late diagnosis—univariable analysis of total cohort.

OR: odds ratio; CI: confidence interval.
IDU remained to be the independent predictor for late diagnosis, as well as age (Table 3).
Variables associated with late diagnosis—multivariable analysis of total cohort.

OR: odds ratio; CI: confidence interval.
Age older than 36 years was significantly associated with late diagnosis with OR = 3.73 (95% CI: 2.43–5.74). Proportion of older persons (>36 years) was significantly higher among those infected through IDU and heterosexual contact compared with male-to-male contact 66%, 48%, and 15%, respectively (p < 0.001).
Attrition from HIV care
Attrition from HIV care was documented in 130 (26.6%) persons. In total, 45 HIV diagnosed patients (9.2%) were not linked to HIV care at all. Attrition from care was reported in 64 (77.1% of those being linked but not started ART) patients after being linked to HIV care and in 66 (18.4% of those started ART) patients after ART initiation. Overall, 31% (40/130) of attrition was due to death and 69% (90/130) due to LTFU.
In total, 54 deaths were reported among the patients diagnosed with HIV in 2013. Out of these 54 patients, 3 were diagnosed with HIV after death, 11 died before linked to care, 15 died after linked to HIV care but before initiated ART and 25 died after initiating ART.
The majority of deaths (83%) occurred within a year from diagnosis, with the median time of 59 days (IQR: 21–209 days). Median time between diagnosis and death for those not linked to HIV care was 4 days (IQR: 0–24 days); for those linked to HIV care, median time from the date of linkage to death was 15 days (IQR: 7–27 days); and for those started ART, the 50% of patients died within 151 days (IQR: 19–385 days) from ART initiation. In total, 88.9% of those died were older than 36 years (p < 0.001) and 92.9% had CD4 (CD4 count was not available for one patient) count ≤350 cell/mm3 at the time of diagnosis (p < 0.001).
In total, 70% of LTFU occurred within the year of diagnosis. Half of these losses occurred within 224 days from diagnoses (IQR: 75–399 days). For those linked to HIV care but did not initiate ART, the median time from the date of linkage until the last visit was 89 days (IQR: 0–265 days). The median time for LTFU from the date of ART initiation until the last visit was 298 days (IQR: 173–398 days). In total, 55.1% of those LTFU had CD4 count ≤350 cell/mm3 at the time of diagnosis. IDU, as a way of HIV transmission, showed statistically significant association with attrition from HIV care (IRR: 1.71, 95% CI: 1.17–2.49) (Table 4).
Univariable analysis of variables associated with attrition from care—total cohort.

IRR: incidence rate rations; CI: confidence interval.
Discussion
Key findings
Among the cohort of individual linked to HIV care, 71% of patients were followed through to the end of the study period, 30 June 2015. Death accounted for 31% of attrition. Patients older than 36 years were more likely to be diagnosed late. Patients who reported getting infected through male-to-male sex had lower odds for late diagnosis compared with heterosexual contacts, while patients who reported acquiring HIV through IDU were more likely to be diagnosed late.
Comparability with other studies
At the stage of diagnosis, the CD4 count <350 cell/mm3 were observed in 67% of cases. This is similar as that found in Mayben et al. 14 study: among 119 patients recently diagnosed with HIV infection in Houston, Texas, 65% had CD4 count <350 cell/mm3.
We found that the delayed diagnosis (<350 cell/mm3) was associated with IDU and >36 years of age. Similar to our findings, Rotily et al. 15 demonstrated that in southern France, the delayed diagnosis were more frequent among injecting drug users than other transmission categories; it was also positively associated with older age. Spanish researchers revealed that in Barcelona, CD4 count ≤350 cell/mm3 upon diagnosis or diagnosis of AIDS within 3 months of HIV diagnosis was positively associated (among other factors) with IDU and older age. 16 Similar findings were observed in Italian study, conducted in 2016, where IDU and older age were positively associated with late presentation. 17 In contrast to our findings, comparison of two groups of late and early testers in the United States found that late testers were significantly more likely to be having been exposed to HIV through heterosexual contacts, although the researches defined the late testers as persons who had their first positive HIV test <1 year before the diagnosis of AIDS. 18 Girardi et al. showed that in Italy, IDU significantly increased the probability of delayed presentation to medical care after being tested HIV-positive but reduced the chance of late testing (CD4 count <200 cell/mm3). 19 Similar to our findings, the Collaboration of Observational HIV Epidemiological Research Europe (COHERE) study, analyzing 2010-2013 data, also found that among MSM, patients with CD4 count ≤350 cell/mm3 were lowest compared with those acquiring HIV through heterosexual contacts and IDU. However, in contrast to our study, in COHERE study, heterosexual contacts were the group among those late presentation was the most prevalent, and in our study, such group was PWID. 20
The risk of having CD4 count <350 cell/mm3 at diagnosis is three times higher (95% CI: 2.1–5.1) among >36-year-old group compared with younger persons. Generally, the previous studies have estimated that the risk of “late testing” in older age groups ranges from 2 to 6.5.21–26 However, it should be mentioned that these studies used different cut-off points for age and for CD4 count that we used. In this analysis, it was estimated that the prevalence of attrition from HIV care was 26.6% and attrition from ART was 18.8%. Similar percentage of attrition from care was observed in pervious Georgian study. Chkhartishvili et al. 27 found that among HIV-infected patients diagnosed in Georgia from January 1989 until June 2012, 27% of the study cohort was not retained in care. Our finding are also in accordance with several other studies conducted in African countries.28–31
We also found that 31% of attrition is due to death, which by itself is largely related to late diagnosis (92.9%). Three hospitalized patients were confirmed to have HIV after death. Out of these three, two were infected by IDU and one reported heterosexual transmission, this again underlines the late diagnosis problems among injecting drug users. In total, 53.7% of deaths occurred among patients not linked to HIV care (14 cases) or linked but not started ART (15 cases). The problem of death before accessing or linked to HIV care was reported by Krentz et al. 32 Out of 543 confirmed cases (Calgary Zone, Canada), one patient was diagnosed after his or her death. In total, 20 of 35 deaths occurred for individuals linked but not retained in care and 15 of 35 among those were in care. 32
Strengths and limitation of the study
Due to the different settings and different definitions that is used in different studies, it is difficult to perform direct comparison with our study findings. The strength of the study is the electronic system which captures demographic, epidemiological, and clinical and laboratory data.
Conclusion
Detection of HIV-infected patients remains the challenge against the fight of HIV epidemic in Georgia. The late diagnosis is the serious problem as patients die shortly after being diagnosed or even begin diagnosed after the death. Our study highlights that particular attention should be given to injecting drug users as they represent the most at risk population for late diagnosis and disengagement from HIV care, as well as patients older than 36 years. The reasons injecting drug users fail to be diagnosed and engaged in care probably are multifactorial and different from patients older than 36 years. More efforts should be put to seek individuals who may be infected as well as to link them to HIV care and ART. For these two groups (injecting drug users and >36 years), additional strategies for finding and maintaining HIV care should be thought to ensure favorable outcomes and reduce HIV transmission.
Footnotes
Acknowledgements
The authors are thankful to Dr Ivana Božičević, the Director of WHO Collaborating Centre for HIV Strategic Information, School of Medicine, University of Zagreb, Croatia, for her support and guidance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the IRB # 00006106 of Georgia AIDS and Clinical Immunology Research Centre.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Infectious Disease, AIDS and Clinical Immunology Research Center (IDACIRC) and The National Center for Disease Control and Public Health’s GFATM’s projects implementation unit.