
Abstract
Objectives:
Data suggest that adolescents in the United States receive inadequate contraceptive counseling. This study sought to determine factors affecting pediatricians’ discussion of contraception with adolescent patients, with a specific focus on long-acting reversible contraception—implantable contraception and intrauterine devices.
Methods:
A cross-sectional survey was sent via email to a convenience sample of pediatric residents and pediatric primary care providers in Western Pennsylvania. Self-reported contraceptive counseling and prescribing practices in response to clinical vignettes were assessed.
Results:
Of potential participants (287), 88 (31%) responded. Younger providers and providers who had received contraceptive training were significantly more likely to discuss long-acting reversible contraception methods. Discussion of contraceptive methods also varied by both the age and the sexual history of the patient.
Conclusion:
Variation in contraceptive counseling potentially results in missed opportunities to counsel about and provide the most effective contraceptive methods. More uniform, universal provider training might alleviate some of these inconsistencies.
Keywords
Introduction
Despite recent decreases, the United States has one of the highest teen pregnancy rates in the industrialized world. In a comparison of sexual activity among adolescents from Sweden, Great Britain, France, Canada, and the United States, the proportion of individuals who had sex before age 20 was similar; however, adolescents in the United States were less likely to use medical methods of contraception (combined oral contraceptive pills (OCPs), injectable contraception, implantable contraception, and the intrauterine device (IUD)) as compared to adolescents in the other countries. 1 In this study, 52% of 15- to 19-year-old US women used medical methods of contraception at last intercourse, compared to 56%–73% of similarly aged women in the other countries studied. 1 These data suggest that low rates of contraceptive use may contribute to the disproportionately high teen pregnancy rates in the United States.
Available data suggest that adolescents in the United States are not routinely offered contraception or counseled appropriately about their contraceptive options. A study of family physicians’ and obstetrician-gynecologists’ contraceptive knowledge revealed that multiple providers in both specialties were unfamiliar with common birth control side effects and contraindications. 2 In another study focusing on family physicians and obstetrician-gynecologists, the authors “considered their patients to be receptive to learning about intrauterine contraception,” but found that only 36% of these physicians discussed intrauterine contraception at visits. 3 Specifically, the authors found that only 39% of the providers felt teenagers were appropriate candidates for intrauterine contraception. 3 Similarly, a study asking eight knowledge-based contraceptive questions to graduating residents from obstetrics and gynecology, internal medicine, family medicine, and pediatrics programs demonstrated that most residents trained in internal medicine, pediatrics, and family medicine were only able to answer half of the questions correctly. 4 This study also found that residents who reported formal training in contraception had statistically significant higher test scores than those who did not report receiving formal training. Improving contraceptive knowledge and training among health care providers could improve contraceptive access for adolescents.
Current American Academy of Pediatrics (AAP) guidelines 5 recommend that adolescent contraceptive needs be addressed in the primary care setting. However, limited data are available regarding the contraceptive prescribing patterns of primary care pediatricians. A study conducted in Chicago interviewed pediatric residents and hospital-affiliated physicians regarding their referrals for contraception and their concerns about various contraceptive methods. 6 This study found a wide variety of perceptions and misconceptions about multiple types of contraception and revealed non-statistically significant trends suggesting that female physicians, recent graduates, and current residents accurately recognized that a wider array of contraceptive methods were appropriate for the patients described in the clinical vignettes provided by investigators. However, this study did not evaluate whether contraceptive counseling patterns were affected by the age of the provider, the patient’s age or sexual history, or provider training in contraception. A survey-based study among Massachusetts pediatricians found that female providers and younger providers were more likely to provide counseling about intrauterine contraceptive devices but did not address the role of contraceptive training in subsequent contraceptive counseling behaviors, nor did it address patient characteristics that might affect counseling, other than patient history of abortion or history of vaginal delivery. 7
In summary, little is known about pediatricians’ contraceptive counseling patterns. As demonstrated by prior studies, multiple factors including provider specialty, contraceptive knowledge base, and gender are associated with whether or not appropriate contraceptive counseling is provided. This study sought to determine factors affecting discussion of contraception with adolescent patients with a specific focus on long-acting reversible contraception (LARCs)—birth control implants and IUDs—because LARCs are the most effective contraceptive methods, are known to be safe to use in the adolescent population, and are recommended as first-line contraceptive options for adolescents; 5 decreasing barriers to LARC use in adolescents is considered a key strategy for reducing teen pregnancy. 8 We hypothesized that provider gender, age, and prior contraceptive training would be associated with the likelihood of discussing LARCs and that younger patients would receive less comprehensive contraceptive counseling than older patients.
Materials and methods
We developed a 24-question survey to distribute to pediatric providers in Western Pennsylvania. The survey was developed by combining and modifying questions from surveys developed by Rubin et al., 9 Swanson et al., 6 and Upadhya et al. 10 A 4-point Likert scale was used for most questions. For example, participants were asked “During an office visit conversation with a female adolescent about contraceptive options, how frequently do you discuss abstinence” and answer choices were “1 = very infrequently,” “2 = somewhat infrequently,” “3 = somewhat frequently,” or “4 = very frequently.” Other questions included multiple response options. For example, participants were asked “For each of the following clinical scenarios, given the patient history, please indicate which types of contraception you would discuss/prescribe at a routine clinic visit.” Each scenario provided a patient age and that patient’s sexual history (e.g. a 14-year-old nulliparous female who is not sexually active). Participants could then select multiple contraceptive options that they would discuss or prescribe. These options included condoms, combined hormonal contraception (patch/pill/ring), injectable birth control (depo medroxyprogesterone acetate (DMPA)), birth control implant, IUD, or none. All questions were geared at assessing self-reported health care provider counseling for various methods of contraception as well as self-reported provider counseling for contraceptive counseling based on patient age and sexual activity. The survey was piloted by three pediatric primary care attending physicians but was not otherwise validated.
We had access to a sample of 287 physicians to participate in the survey. We assumed, based on the literature, that approximately 29% would answer the survey 11 and that approximately 36% would report discussing IUDs with adolescents. 3 Assuming an alpha of 0.05, the width of the confidence interval (CI) of the estimate would not exceed 0.20. 12
The survey was sent to two groups. The first group, pediatric primary care providers, was recruited through the University of Pittsburgh Clinical and Translational Science Institute pediatric practice-based research network, Pediatric PittNet (n = 174 primary care providers at the time of the study). The second group, pediatric residents, was recruited from the Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center (n = 113). Providers were sent the link to the anonymous Qualtrics© survey by email. The survey was open for response from July to September of 2014. Reminder emails to complete the survey were sent periodically during the study period. This study was deemed exempt by the University of Pittsburgh Institutional Review Board.
We excluded attendings, fellows, and nurse practitioners in the division of adolescent medicine from the study, as it was assumed that their level of comfort and education surrounding contraception was higher than that of a general pediatrician.
Data analysis was performed using STATA 13.1. McNemar’s test and chi-square test were used to compare responses to determine whether a statistically significant difference in prescribing was present between physicians of different ages, genders, or for those who did or did not have contraceptive training. These variables were chosen because existing literature suggests that they may impact contraceptive counseling and prescribing habits. Additionally, differences in prescribing patterns between patients of different ages and patients with different sexual histories were assessed. While some respondents did not answer all questions asked, the amount of missing data was low (9%). Those with missing data were not included in analyses involving that variable. For those answers with fewer than five respondents, Fisher’s exact test was used. For multivariate analysis, a logistic regression was performed. All variables that were significant in the univariate analysis were included in the multivariate analysis.
For the question about training on prescribing contraception, responses were grouped to include any type of training (lecture, clinical experience, published literature, adolescent medicine rotation) as “yes” and no training as “no.” The word “discuss” is used in the results section to convey that a prescriber reported he or she would “discuss, prescribe or refer a patient” for that contraceptive type. For data analysis, participants that responded that they “1 = very infrequently” or “2 = somewhat infrequently” discuss a method were grouped as “infrequently,” and participants that responded “3 = somewhat frequently” or “4 = very frequently” were grouped as “frequently.”
A prior study with a median respondent age of 48.6 years found that younger physicians were more likely to provide comprehensive contraceptive counseling than older physicians. 3 For our analysis, respondents were grouped into “over age 50” and “under age 50.”
Results
Of potential participants (287), 114 opened the survey, but those who answered no questions or only filled in demographic information were eliminated from data analysis. In total, 88 respondents (31%) provided usable data, of whom 31 (35%) were attending physicians, 6 (7%) were nurse practitioners, and 51 (58%) were pediatric residents. In all, 65 participants (74%) were female, and 69 (78%) were under age 50. Full demographic information is shown in Table 1.
Characteristics of survey respondents (n = 88).
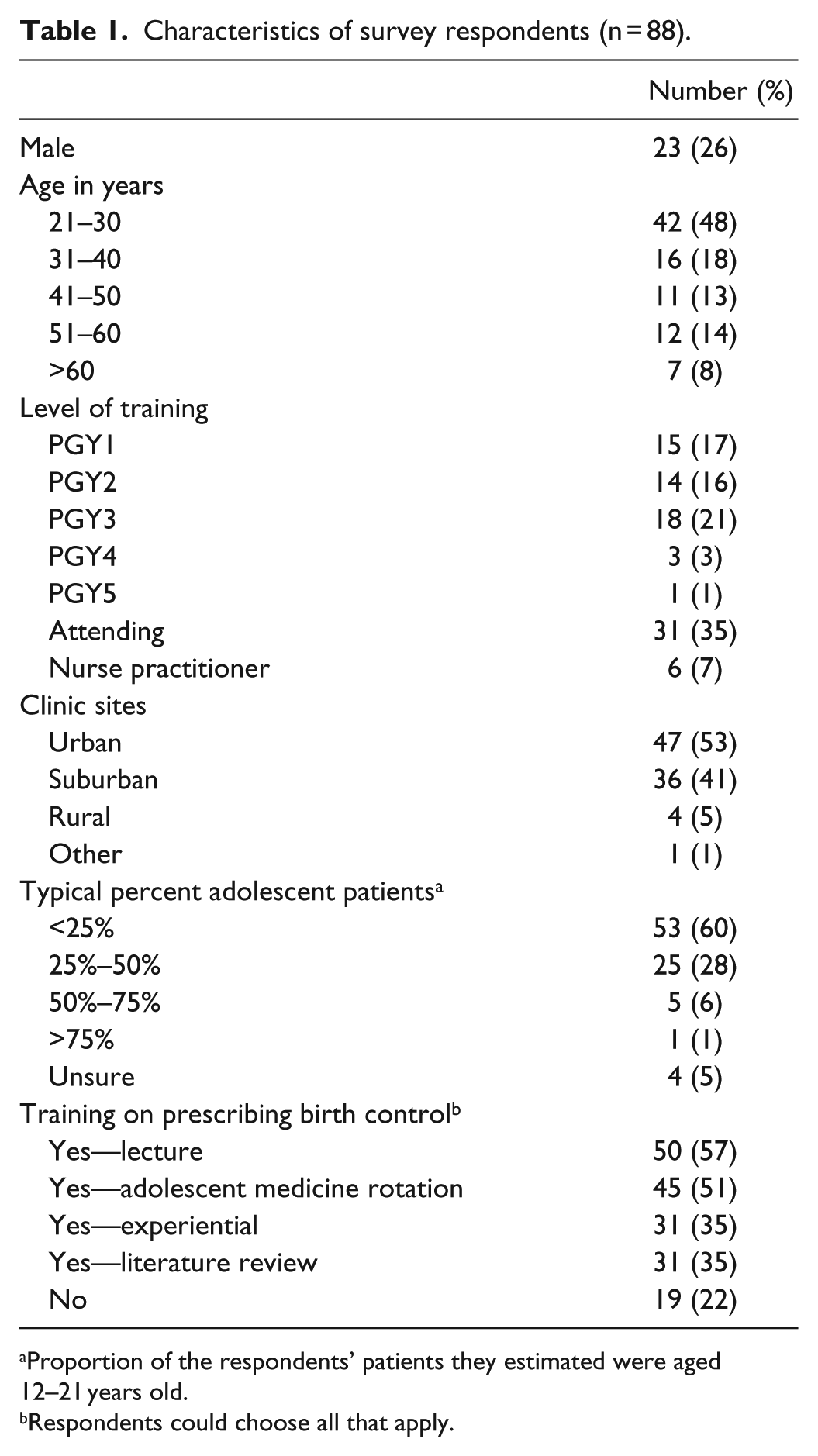
Proportion of the respondents’ patients they estimated were aged 12–21 years old.
Respondents could choose all that apply.
Across all providers, combined OCPs were most likely to be discussed, with 74 (94%) respondents reporting having prescribed or referred an adolescent for this contraceptive type. Only 29 (37%) respondents discussed an IUD and only 20 (25%) a birth control implant (Implanon® or Nexplanon®; Merck, Kenilworth, NJ).
Contraceptive discussion varied by both the age and the sexual history of the patient with trends toward increased discussion of all contraceptive options with increasing patient age. For the vignette describing a routine clinic visit for a nulliparous female patient who was not sexually active, only 48 (60%) providers stated they would discuss any contraceptive method beginning at age 14, whereas 71 (90%) providers would discuss at least one contraceptive option with a 16-year-old patient and 74 (94%) with an 18-year-old patient. Regarding sexual history, all providers would discuss at least one contraceptive option with adolescents who are sexually active or have a history of pregnancy, regardless of age.
In specifically examining referrals for LARCs, patient age impacted these referrals as shown in Figure 1. For nulliparous sexually active females, implants and IUDs were more likely to be discussed as patients increased in age, with a statistically significant difference noted between 14-year-old patients and 18-year-old patients (implant 52.4% vs 64.6%, p = 0.013; IUD 42.7% vs 58.5%, p = 0.001). Similarly, for patients with a history of pregnancy, LARC methods were discussed more frequently with increasing patient age, with a statistically significant difference between 14-year-old patients and 18-year-old patients (implant 65.9% vs 74.4%, p = 0.02; IUD 62.2% vs 72.0%, p = 0.005).

Percentage of pediatricians discussing LARCs in sexually active nulliparous females stratified by patient age.
Additionally, within a specific age group, the sexual history of a patient informed referrals for LARCs as shown for 16 year olds in Figure 2 (similar patterns were seen for 14 and 18 year olds, data not shown). For example, while few prescribers reported they would discuss LARC methods in the vignette describing a 16-year-old nulliparous female who was not sexually active (25.3% implant, 24.0% IUD), the proportion who said they would discuss these methods increased when a patient was sexually active or had a history of pregnancy; differences between all groups were statistically significant.

Percentage of pediatricians discussing LARCs in 16-year-old patients stratified by patient’s sexual activity.
As shown in Table 2, providers who reported they had received contraceptive training (“trained”) were more likely to discuss abstinence (odds ratio (OR) = 5, CI = 1.3–13.2), OCPs (OR = 5, CI = 1.3–16.1), DMPA (OR = 25, CI = 3–200), implantable contraception (OR = 16.7, CI = 1.9–125), and IUDs (OR = 25, CI = 3.1–200). Female providers and providers under the age of 50 were also more likely to discuss IUDs than other providers (female OR = 5, CI = 1.4–16.1; age less than 50 OR = 5.8, CI = 1.5–22.6). Female providers were also more likely to discuss OCPs (OR = 5, CI = 1.4–16.1) and DMPA (OR = 5, CI = 1.3–12.5) than male providers. Providers under age 50 were less likely to discuss abstinence (OR = 0.3, CI = 0.1–0.9) than providers over age 50. In multivariate analysis, as shown in Table 3, we examined whether variables that were statistically significant in the univariate analysis were independently associated with discussion of various contraceptive methods. In terms of discussing abstinence, adjusted OR for providers less than 50 years old is 0.2 (CI = 0.1–0.8) and adjusted OR for providers who received training is 5.6 (CI = 1.5–20.4). Similarly for OCPs and DMPA, adjusted OR for providers who reported training in contraception and for female providers remained statistically significant in multivariate analysis (OCPs trained adjusted OR = 4.8, CI = 1.3–18.9; OCP female adjusted OR = 5, CI = 1.3–18.2; DMPA trained adjusted OR = 25, CI = 3.3–250; DMPA female adjusted OR = 4.6, CI = 1.3–15.4). For the IUD, the variables providers under age 50, providers with contraceptive training, and female providers all remained statistically significant after adjustment (age less than 50 adjusted OR = 10.3, CI = 2.2–48.6; trained adjusted OR = 37, CI = 4.1–333, female adjusted OR = 8.8, CI = 2.1–37).
Percentage of providers who frequently discuss various contraceptive methods. a

DMPA: depo medroxyprogesterone acetate; IUD: intrauterine device; CI: confidence interval.
Data depicted as number of positive responses/total number of responses. Total number of responses varies because survey participants with missing data for these questions were excluded from analysis.
p < 0.05.
p < 0.001.
Multivariate analyses for contraceptive discussion.

IUD: intrauterine device; OR: odds ratio; CI: confidence interval.
Discussion
All reversible contraceptive methods, including LARCs, are known to be safe and efficacious in nulliparous female adolescent patients. 5 However, only 52% of pediatric primary care providers in Pittsburgh would discuss the contraceptive implant, and only 42% of providers would discuss an IUD at a routine office visit with a 14-year-old sexually active female. Specific to LARC methods, participants reported they would be more likely to counsel about a LARC method with increasing patient age and in scenarios in which patients are sexually active or have a history of pregnancy.
Prior research has shown that contraceptive counseling provided by primary care providers, including pediatricians, is variable in terms of when it occurs, what types of contraceptive options are offered, and providers’ contraceptive knowledge base.2–4,6,7,13 Specific to LARC methods, much of the prior research has focused on intrauterine contraception options and has found that pediatricians lack training in these methods and do not routinely counsel about these methods.6,7 However, as demonstrated by the CHOICE study in St. Louis, when education is provided to patients about LARC methods and when barriers to accessing these methods are removed, adolescents prefer LARCs. 13
We found that providers under 50 years old and those with contraceptive training were more likely to counsel about LARCs, IUDs, and implants when compared with providers over age 50 and those without contraceptive training, respectively. Female providers were also more likely to counsel about LARCs, although this trend was statistically significant only with IUDs not implants. Our study also demonstrated that receiving contraceptive training increased self-reported contraceptive counseling. Unfortunately, our sample size was too small to compare different types of training or to explore interactions between age and training.
A prior study noted that pediatricians in Boston were more likely to discuss intrauterine contraception with patients with a history of a vaginal delivery or abortion. 7 Similarly, our study found that adolescents who are sexually active or have a history of prior pregnancy were more likely to receive contraceptive counseling that included discussion of LARC methods. We also investigated patient age as a variable in contraceptive counseling and found that younger patients were less likely to receive comprehensive contraceptive counseling than older adolescents with the same sexual history. Our study did not address pediatricians’ contraceptive knowledge base, although other studies asking knowledge-based questions of pediatricians show that they are frequently unable to answer them correctly.6,7 This study also did not address the practicality of contraceptive counseling within the time constraints of a routine office visit. It is possible that many of the responders would provide contraceptive counseling given more time to do so in an office visit.
An important limitation of our study is that only 31% of eligible participants completed the survey. Physician response rates to surveys vary significantly depending on delivery mode.14–18 Our survey was sent via email, and our response rate is within the range typically found with email-based surveys of physicians, which are known to be as low as 9%. 11 Previous studies of various physician groups have found response rates from 26% to 45%.15–18 One study found that pediatrician response rates average around 29%. 11 Accordingly, the low response rate, particularly among individuals over the age of 50, limits the generalizability of our findings.
At the time of this survey, the Children’s Hospital of Pittsburgh of UPMC residents were 27% male (31 men and 82 women) similar to the breakdown of male and female respondents to the survey but slightly lower than proportion of male AAP resident members (33% in 2011). 19 The gender breakdown of members of PittNet is unknown. Additionally, the age breakdown of both the pediatric residents and the members of PittNet is unknown. Therefore, it is a limitation to our study that we cannot determine whether our respondents are demographically representative of the 287 pediatricians to whom we sent our survey. Nor can we make precise comparisons to the population of primary care pediatricians in the United States, about whom limited data exist; recent data, however, suggest that they are more likely to be male and more likely to be older than our respondents. In 2011, 43% of general pediatricians were male (according to the American Medical Association Masterfile). 19 Data from the American Board of Pediatrics (ABP) show that in 2015, among those currently or previously certified by the ABP (including subspecialty pediatricians and excluding residents), 48% were male and 48% were under 50 years of age. 20 In 2014, 58% of members of the AAP (which also includes some subspecialty pediatricians, does not include all general pediatricians, and excludes residents) were under age 50. 21 Thus, it is possible that women and younger physicians, those found in the literature to be most likely to discuss IUDs,3,4,6,7 are overrepresented in our sample and therefore our survey may overestimate the frequency with which pediatricians in our region were discussing LARC methods with their adolescent patients.
Prevention of unintended pregnancy is an important aspect of preventive care for adolescents, and contraception should be offered to teens choosing not to be abstinent. A recent study in Minnesota focused on missed opportunities to provide contraceptive counseling, which were defined as preventive, acute, or follow-up visits with a physician, nurse practitioner, or physician’s assistant in pediatrics, family practice, or obstetrics and gynecology in the 12 months prior to pregnancy. 22 The study focused on adolescents aged 15–19.9 years with continuous health insurance coverage in the study period and found a mean of 2.7 missed opportunities per teenage pregnancy. Of these visits, sexual activity was not documented in 57%, and reproductive health counseling was not documented in 47%. This suggests that health care providers are not maximizing opportunities to provide contraceptive counseling to adolescent patients who may be at risk for pregnancy.
All contraceptive methods can be used for menstrual problems such as dysmenorrhea and heavy menstrual bleeding. While not addressed in our survey, we note that the most recent AAP guidelines recommend pediatricians be familiar with the use of contraception to treat medical concerns. 5 Thus, even for patients choosing abstinence, there is a role for discussion of contraceptive methods at office visits.
Our sample size limited our ability to explore how training might affect contraceptive counseling differently based on the respondent’s age. Our survey also did not assess the content of the training received, and it is likely that providers of different ages received different types of contraceptive training. In order to better inform future training efforts, we recommend that future studies ask about the specific content of previous training. This study focused primarily on patient demographics and provider demographics; further research is needed to investigate ways to facilitate comprehensive contraceptive counseling even during office visits that have multiple priorities to be addressed during a brief health care encounter.
In summary, contraceptive counseling varies widely among pediatric health care providers and is affected by provider demographics and patient characteristics, potentially resulting in missed opportunities to counsel about and provide the methods most effective in preventing unintended pregnancies and their consequences. LARCs are known to be safe for adolescents so it is critical that LARCs be included, and described as the most effective method, for adolescents of all ages in need of contraception. More uniform, universal provider training might alleviate some of these inconsistencies. For those adolescents deciding not to be abstinent, it is critical that pediatricians include comprehensive pregnancy prevention and contraceptive counseling as part of preventive care.
Footnotes
Acknowledgements
The authors thank Drs Alicia Haupt, Kristin Ray, and Timothy Shope for piloting the study and Dr Evelyn Reis, the Medical Director of Pediatric PittNet, for her help with distributing the survey.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.S.S. has been a site PI in multi-site trials and received reimbursement for research-related activities from Teva, a pharmaceutical company that produces contraceptives. There are no other conflicts of interest to disclose.
Ethical approval
Ethical approval for this study was waived by The University of Pittsburgh Institutional Review Board because this project meets all the necessary criteria for an exemption and is hereby designated as “exempt” under section 45 CFR 46.101(b)(2) Tests, surveys, interviews, observations of public behavior.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIH/CTSA Grant UL1TR000005 (Pediatric PittNet).
Informed consent
Neither written nor verbal informed consent were obtained from subjects before the study. The emails with the link to the survey included a standard text discussing the purpose of the study and outlining risks and benefits to participants as well as the voluntary nature of participation. Participants indicated their willingness to participate by clicking the survey link.