
Abstract
Objectives:
The utilization of long-acting reversible contraceptive methods is one of the key factors in protecting women and couples against unwanted pregnancies. The study aimed to assess the determinants of long-acting reversible contraceptive use among women in Northwest Ethiopia.
Methods:
A community-based unmatched case-control study was conducted from 1 February to 8 March 2017 in Northwest Ethiopia. The cases were women who used long-acting reversible contraceptive methods, and the controls were women who used short-acting contraceptives. Both of them were selected using a systematic sampling method. An interviewer-administered questionnaire was used to collect the data. Epi info and SPSS version 23 were used for data entry and analysis, respectively. Descriptive statistics and association measures were done and presented in texts, tables, and figures.
Results:
A total of 882 women were interviewed, with a response rate of 99.3%. Women who were between 15 and 24 years old were two times more likely to use long-acting reversible contraceptive methods than those whose age was ⩾35 (adjusted odds ratio = 2, 95% confidence interval: (1.20, 3.50)). A good level of knowledge about long-acting reversible contraceptive methods (adjusted odds ratio = 11.6, 95% confidence interval: (5.42, 24.80)), a negative attitude toward long-acting reversible contraceptive methods (adjusted odds ratio = 0.31, 95% confidence interval: (0.21, 0.46)), membership in the health development army (adjusted odds ratio = 2.8, 95% confidence interval: (2.12, 3.78)), no discussion with a partner about long-acting reversible contraceptive methods (adjusted odds ratio = 2.3, 95% confidence interval: (1.54, 3.49)), and more than 2 years of desire to wait before another pregnancy (adjusted odds ratio = 23.7, 95% confidence interval: (11.63, 48.55)) were determinants of long-acting reversible contraceptive methods use.
Conclusion:
This study revealed that attitude toward long-acting reversible contraceptive method use, being a member of the women’s health development army, and the desire to space children were determinants of long-acting reversible contraceptive method use. More actions should be taken to increase the utilization of long-acting reversible contraceptive methods by promoting discussion between partners about modern contraceptives and increasing women’s participation in being a member of the health development army.
Introduction
The World Health Organization (WHO) and the United Nations Population Fund (UNFPA) launched five key targets to help nations get back on track in decreasing unnecessary maternal deaths and tracking progress toward the Sustainable Development Goals. From 2000 to 2017, maternal mortality fell by more than a third globally. Despite this, an estimated 810 women die every day as a result of pregnancy and childbirth complications. Developing countries account for 99.0% of all maternity-related deaths, with Sub-Saharan Africa being the most risky region in the world.1,2
Modern family planning methods, particularly long-acting reversible contraceptive methods (LARCMs), are highly effective in reducing maternal mortality by preventing unintended and closely spaced pregnancies. 3 These methods are safe, effective, inexpensive, and reversible and have much better compliance rates than other hormonal methods. 4 These LARCMs include intra-uterine devices (IUDs) and implants.3,5
The demand for long-acting reversible contraceptive methods (LARCMs) is one of the key factors in protecting women and couples against unwanted pregnancies. However, the proportion of women using these methods was lower than the proportion who desired to use them.3–6 In many countries, less than 5% of women use LARCMs. The reasons are that many services and supplies are not yet available everywhere, choices are limited, fear of social disapproval, partner’s opposition poses formidable barriers, worries about side effects, and health concerns hold some people back, while others lack knowledge about contraceptive options, and their use. 5 Closely spaced pregnancies increase the risk of infants with adverse outcomes such as preterm birth, low birth weight, and small for gestational age. 7
In Ethiopia, the prevalence of reproductive-age women who were using LARCMs was 18.4%. 8 The prevalence of married women who used long-acting reversible contraceptives was 11.0%. Even though the total fertility rate in Ethiopia is 6.7, the modern contraceptive prevalence rate (CPR) among married Ethiopian women is 41%. 9 Short-acting contraceptives, such as pills and injectables, were the most commonly used contraceptive methods in Ethiopia. The unmet need for family planning shows the discrepancy between women’s reproductive intentions and their contraceptive behavior. Twenty-six percent of currently married women had unmet family planning needs. 10 However, studies addressing the determinants of long-acting reversible contraceptive use with a more robust design and a larger sample size are limited. Therefore, this study aimed to identify the determinants of LARCMs among modern contraceptive users in the Jawi woreda, Awi Administrative Zone, Northwest Ethiopia.
Methods
Study design and study setting
A community-based unmatched case-control study was conducted from 1 February 2017 to 8 March 2017, in Jawi district, Awi zone, Amhara region. Jawi district is located 148 kilometers from Bahir Dar (the capital city of the Amhara region) and 548 kilometers from Addis Ababa (the capital city of Ethiopia). There are five health centers, 27 health posts, and 39 private clinics in the woreda. Jawi district is administratively structured into 25 rural and two urban kebeles. The total population is 139,041 (68,825 males and 70,216 females) as projected by the Ethiopian Central Statistical Agency Population Census. 11 There are a total of 32,786 females in the reproductive age group in the district. According to the 2018 health office report, family planning coverage was 67.0%. 12
Population
The source populations of the study were all women who were using modern contraceptive methods, which included both short-acting and long-acting reversible contraceptives, and who lived in the Jawi district. The study populations were those women who were using long-acting reversible and short-acting modern contraceptives in the study area during the study period.
Case and control definition
Cases were women who had been using LARCMs and lived in the study area for at least 6 months before the data collection period. Controls were those women who were using short-acting reversible contraceptive methods and resided in the study area for at least 6 months before the data collection period. Women who used emergency contraceptives at the time of data collection and those women who used female and male sterilizations were excluded from the study.
Sample size determination
The sample size was determined using Epi Info version 7.14 software with the following assumptions: an adjusted odds ratio (AOR) of 0.5 (0.25–0.98), a 95% confidence interval, 80% power, two design effects, and a case-to-control ratio of 1:2, 80.8% of controls were exposed. 13 By adding a 5% nonresponse rate, the total sample size became 882 (294 cases and 588 controls).
Sampling procedure
A stratified sampling technique was used to classify urban and rural kebeles in the Jawi district. We selected five kebeles from the 25 rural kebeles and one kebele from the two urban kebeles using a simple random sampling method. Then, the samples were allocated proportionally to each kebele. Finally, the study participants were selected using a systematic random sampling method (Figure 1).

Sampling procedure to select the study participants in Jawi district, Ethiopia.
Operational definitions of terms
Long-acting reversible contraceptives: these include implants and IUDs, but do not include female and male sterilizations.
Short-acting contraceptives: these include pills, condoms, and injectables.
Good knowledge of LARCMs: those who scored 80.0% or higher on the distinct features of LARCMs on eight knowledge questions.
Moderate knowledge of LARCMs: those who scored 50.0% to 79.0% on eight knowledge questions on distinct features of LARCMs.
Poor knowledge of LARCMs: those who scored less than 50.0% on eight knowledge questions for any of the LARCMs.
Positive attitude: those who scored 50.0% or above positive answers out of six attitude questions.
Negative attitude: those who scored <50.0% positive answers out of six attitude questions.
Data collection and Quality control
A pretested structured questionnaire was adapted from different kinds of literature.3,7,9,12,13 The questionnaire was prepared in the English language and then translated into the local language. Then, it was translated back to the English language by people who are proficient in both languages to maintain the consistency of the questionnaire, which was also validated. The data were collected at the household level.
Six female diploma nurses were recruited for data collection, and two BSc nurse supervisors were assigned. Data quality was maintained through training, the questionnaire being pretested on 5% of the contraceptive users chosen at random, close monitoring, and supervision.
Statistical analysis
The data were entered, edited, coded, and cleaned using Epi info version 7.1.4 and then exported to SPSS version 23 software for analysis. Descriptive statistics and both bivariate and multivariate logistic regressions were made to control confounding factors and identify the determinants of LARCMs. Variables with a p ⩽ 0.20 in the bivariate logistic analysis were entered into the multivariate logistic regression model. Variables having a p ⩽ 0.05 were considered statistically significant in the multivariate logistic analysis. The Hosmer and Lemeshow goodness-of-fit test was used to assess the model’s fitness and a p > 0.05 was considered a good fit. Proportions, crude, and AORs with their 95% confidence intervals were presented using text, tables, and figures.
Results
Sociodemographic characteristics of the respondents
A total of 882 (294 cases and 588 controls) modern contraceptive users with a response rate of 99.3% (876) were interviewed. The mean age of the study participants was 27.33 ± 6.95 and 28.14
Sociodemographic characteristic of contraceptive users in Jawi district, Ethiopia.

Knowledge and attitude of contraceptive users about LARCMs
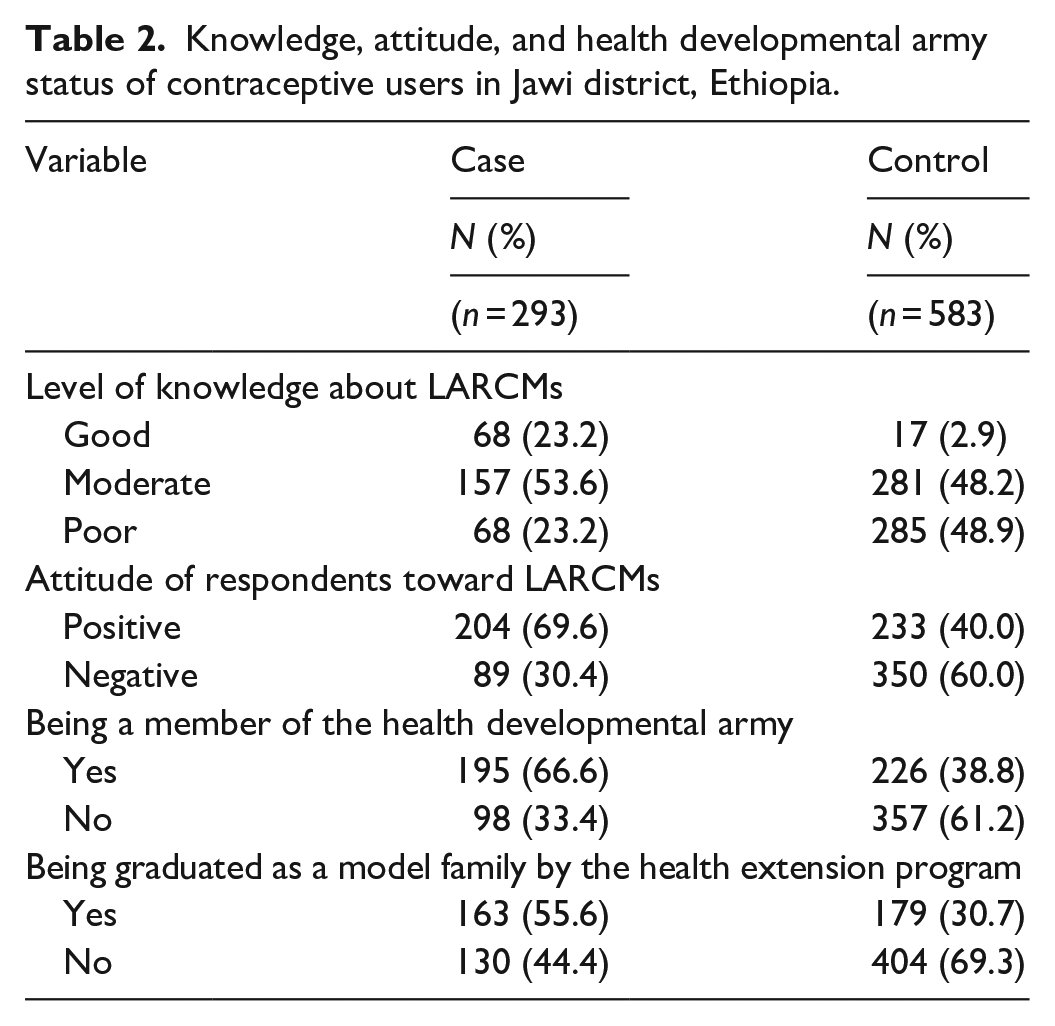
The level of knowledge of the study participants was assessed by asking eight questions. Sixty-eight (23.2%) cases and 17 (2.9%) controls had good knowledge of LARCMs. Similarly, the attitude of study participants was assessed by asking six questions. About 89 (30.4%) of cases and 350 (60.0%) of controls had a negative attitude toward LARCMs. One hundred ninety-five (66.6%) cases and 226 (38.8%) controls were members of the health development army. One hundred sixty-three (55.6%) cases and 179 (30.7%) controls were graduated as model families by the health extension programs (Table 2).
Knowledge, attitude, and health developmental army status of contraceptive users in Jawi district, Ethiopia.
Reproductive characteristics of long-acting reversible and short-acting contraceptive users
About 56 (19.1%) cases and 121 (20.8%) controls had five and more children, respectively. Two hundred three (69.3%) cases and 509 (87.3%) controls wanted to give birth in the future. One hundred-sixty (54.6%) of the cases and 227 (38.9%) of the controls made a joint decision to limit the number of children they had with their husbands. About 201 (68.6%) cases and 237 (40.7%) controls had a discussion with their husbands about contraceptives. Health providers were the first source of information about LARCMs for 243 (82.9%) of cases and 190 (32.6%) of controls (Table 3).
Reproductive and service-related characteristics of contraceptive user women in Jawi district, Ethiopia.

Determinants of LARCM use
Women’s age, being a member of the health developmental army, knowledge about LARCMs, attitude toward LARCMs, women’s provider sex preference to receive family planning service, child spacing desire, and discussion with husbands were statistically significant factors for LARCM use (Table 4).
Bivariable and multivariable analysis of determinants of LARCM use among women in Jawi district, Ethiopia.
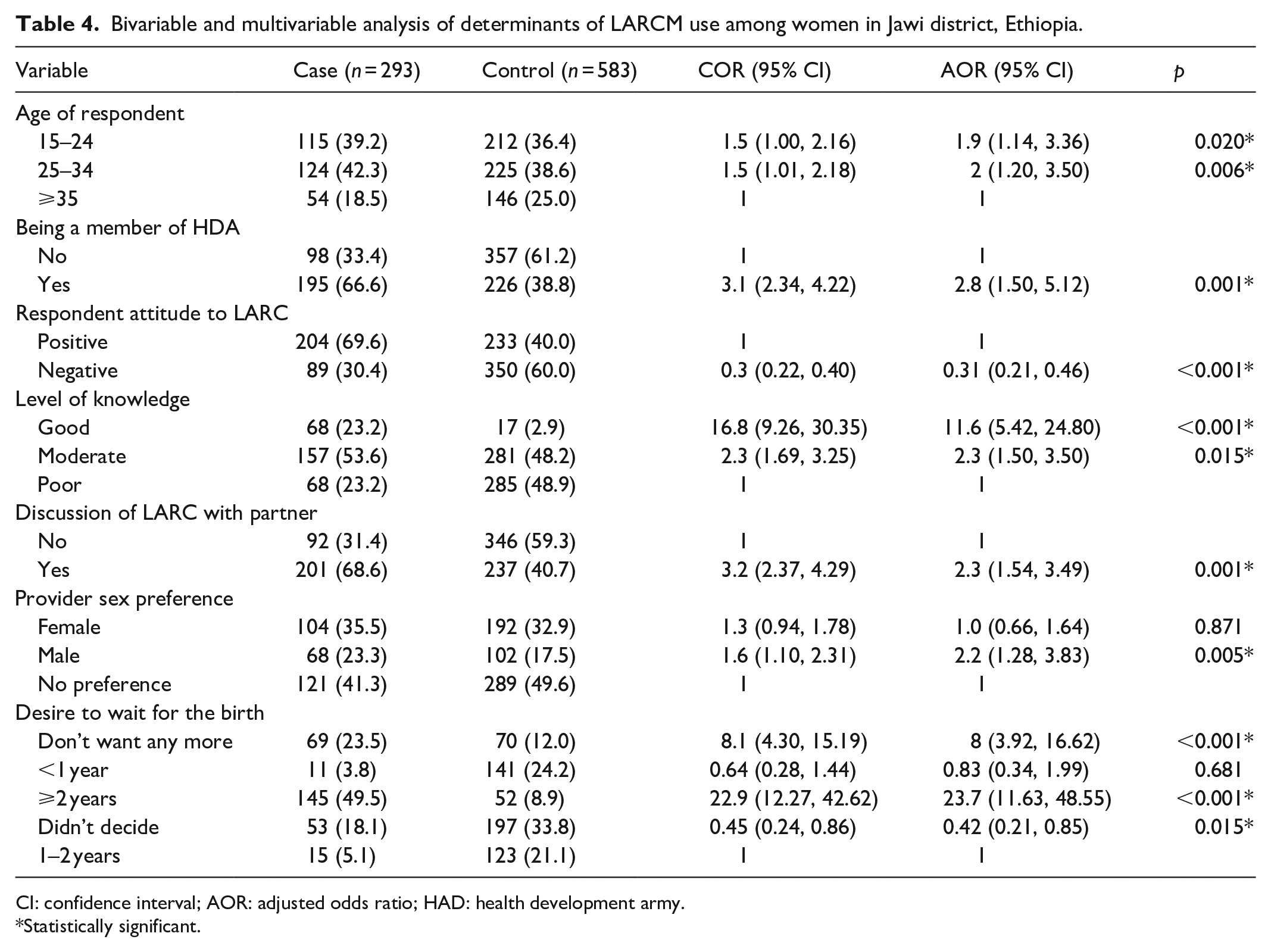
CI: confidence interval; AOR: adjusted odds ratio; HAD: health development army.
Statistically significant.
Women aged 15 to 24 years old were positively associated with the use of LARCMs. Women aged 15–24 years were 1.9 times more likely to use LARCMs than women aged 35 and older (AOR = 1.9, 95% CI: (1.14, 3.36)). Similarly, women at age 25–34 years were positively associated with the use of LARCMs (AOR = 2, 95% CI: (1.20, 3.50)).
Women who were members of the HDA were associated with the use of LARCMs (AOR = 2.8, 95% CI: (1.70, 6.25)). This means those women who were members of the HDA were 2.8 times more likely to use LARCMs than women who were not members of the HDA.
The husband–wife discussion was found to be a statistically significant association with LARCMs use (AOR = 2.3, 95% CI: (1.54, 3.49)). Women who had the experience of discussion with their husbands were 2.3 times more likely to use LARCMs as compared to those who did not have a discussion (Figure 2).

Decision-maker to use contraception among women in Jawi district, Ethiopia
The level of knowledge was the main determinant factor of LARCM use. Women with a good level of knowledge on LARCMs were 11.6 times more likely to use LARCMs compared to those who used short-acting contraceptives (AOR = 11.6, 95% CI: (5.42, 24.80)). Women with a moderate level of knowledge about LARCMs were 2.3 more likely to use LARCMs compared to those who used short-acting contraceptives (AOR = 2.3, 95% CI: (1.50, 3.50)). However, women who had a negative attitude toward LARCMs were 69% less likely (AOR = 0.31, 95% CI: (0.21, 0.46)) to use LARCMs than controls.
Child spacing desire was a strong determinant for LARCMs use. Women who wanted to wait more than 2 years before another pregnancy were 23.7 times (AOR = 23.7, 95% CI: (11.63, 48.55)) more likely to use LARCMs than those who wanted to wait for 1 to 2 years. Women who did not want any more pregnancies were eight times (AOR = 8.0, 95% CI: (3.92, 16.62)) more likely to use LARCM than those who want to wait for 1–2 years before another pregnancy. Women who had not decided on waiting time were 58.0% less likely to use LARCMs (AOR = 0.42, 95% CI: (0.25, 0.86)) than those mothers who wanted to wait 1–2 years before another pregnancy.
Service provider sex preference was another determinant factor for LARCM use. Women who preferred male service providers for family planning were two times more likely (AOR = 2.2, 95% CI: (1.28, 3.83)) to use LARCMs than those women who did not have a sex preference.
Discussion
This community-based case-control study identified determinants of LARCMs among modern contraceptive users in Jawi, Ethiopia. After handling other confounding factors, age, level of knowledge, attitude to LARCMs, being a member of the health, developmental army, and wife–husband discussion about contraceptive methods, child spacing desire, and sex preference to get family planning services were found to be the determinant factors of LARCM utilization.
The use of LARCMs is higher among women aged 15–24 years and women aged 25–34 years. This result is in line with the study done in Malawi and Debre Markos.6,14 The possible reasons for this could be young women aged between 15 and 24 years might have a fear of being at higher risk of unintended pregnancy and get much more information on the benefits of LARCMs through various media. However, this finding counters a report from Areka town. Women in the Age group ⩾ 35 years were 3.99 times more likely to use LARCMs compared to women in the age group 15–24 years. 11 The possible explanation for the disparity might be because of small variations in age groups and the need for child spacing might be high in women whose age is ⩾ 35 years old.
However, women who had good knowledge about LARCMs were more likely to use LARCMs compared to those who had poor knowledge. This finding was consistent with the study done in Hossana, Arbaminch, and Bisheftu towns.3,10,15
The odds of LARCM utilization increased for women who had a positive attitude toward LARCMs. Women who had a negative attitude were 69% less likely to use LARCMs than mothers who had a positive attitude. This is consistent with a study done in Arba Minich town and the Wolaita zone.3,4 The reason behind this might be that women may get adequate information about the benefits of LARCMs and decide to use them. Governmental organizations and NGOs were working better on the importance of long-acting family planning methods.
In contrast, women having discussions with their husbands on LARCMs were 2.3 times more likely to use LARCMs than women who did not have discussions. It is scientifically sound that if there is no discussion between husband and wife, it has a negative influence on the use of LARCMs. This result is supported by studies conducted in Debre Markos, Dendi district, Rwanda, Western Ethiopia, and Hossana town.5,12,15,16 The probable reason might be that, in developing countries like Ethiopia, men have great dominance over women and play a great role in decision-making in family planning use and method choice. It may also be because of cultural barriers in Ethiopia. The magnitude of family planning services chosen by the health providers was higher in cases compared with controls. This may be due to the fact that the women might be forced to receive the providers’ preferences rather than their own preferences.
Being a member of the HDA had a positive impact on the use of LARCMs. This may be due to the women’s being members of the HDA; their level of knowledge and attitude toward LARCMs increased. This is the fact that if there were a discussion, the participants would learn something new and important about the discussion.
Women who wanted to wait more than 2 years before the next pregnancy were 23.7 times more likely to use LARCMs than those women whose desire was 1–2 years. This result is supported by a study done in Malawi. In contrast, women who did not decide their waiting time before the next pregnancy were 58% less likely to use LARCMs than women whose desire was 1–2 years. Women who did not want any more pregnancies were 8 times more likely to use LARCMs than those whose desire was 1–2 years. This result was supported by EDHS 2019. 11
The strength of this study was the use of primary data collected through face-to-face interviewing, which might minimize errors. The second strength might be the use of a strong study design that shows the cause-effect relationship. In addition to this, the sample size was large enough to provide strong evidence of case-control group comparability. The main limitation of this study was that there might be a recall bias among women who were interviewed regarding their previous use of LARCMs. The study lacked qualitative findings that might have provided further insight into some of the concerns regarding current contraceptive methods.
Conclusion
In this study, age, husband-wife discussion, being a member of the health developmental army, level of knowledge, and attitude toward LARCM use, child spacing desire, and provider sex preference to taking contraceptives were determinants of LARCM use. More action should be taken to increase the utilization of LARCMs by promoting discussion between partners about modern contraceptives, increasing women’s knowledge and attitudes toward LARCMs, and increasing women’s participation in being a member of the health developmental army in the kebele.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221094658 – Supplemental material for Determinants of long-acting reversible contraceptive use among women in Jawi woreda, North West Ethiopia: A case-control study
Supplemental material, sj-docx-1-smo-10.1177_20503121221094658 for Determinants of long-acting reversible contraceptive use among women in Jawi woreda, North West Ethiopia: A case-control study by Abiyot Wolie Asres, Ayele Almaw Tiruneh, Addisu Gasheneit Ferede and Woldeamilak Adamu Hunegnaw in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the data collectors, supervisors, and women who participated in this study.
Author contributions
W.A. and A.A. conceived and designed the study, performed the analysis, and interpreted the data. A.G. and A.W. participated in the design, analysis, and interpretation of data. W.A., A.G., A.W., and A.A. participated in drafting the manuscript. All authors read and approved the final submitted version of the manuscript. All authors have agreed to both be personally accountable for the author’s contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Bahir Dar University, College of Medicine and Health Science, Institutional Review Board with the ethics approval number CMHS/278/2017.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study. The exceptions for consent to medical treatment for minors fall into two categories. The first is for situations where the minor is married or is the parent of a child. The second is for situations where a minor seeks particular types of treatment. These minor subjects did not require parental or guardian consent because they were married and lived independently. Furthermore, the study did not need medical treatment or did not have an injury for individuals under the age of 18 years. They gave their own written informed consent. These concerns were taken into account by the IRB when approving the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.