
Abstract
Objective:
Tobacco education is among the initiatives encouraged for health professionals to help them appreciate the significance of addressing tobacco use among their patients. In this pilot study, a nicotine biomarker (cotinine) study was introduced to an applied microbiology course required of all allied health students. Participants assessed their own smoking status in the previous 24 h using a two-dimensional experimental design of a questionnaire and rapid urinary cotinine immunoassay. The study goals were >90% participation of the home-administered assay and high correlation of the results to cotinine standards. Allied health students (medical assistants, respiratory therapists, surgical technicians) were selected as the initial test group.
Methods:
The study was initiated 10 months after the college became 100% tobacco free. Participants were initially trained on the use and interpretation of the rapid cotinine test using three cotinine standards (0, 400, and 2000 ng/mL urine). Participants subsequently tested their own first-morning urine sample at home and then answered a questionnaire about their tobacco smoke (and/or nicotine) exposure in the previous 24-h period.
Results:
The cotinine laboratory was offered to a total of 161 students (88% female) over 24 months. Participants who reported no exposure to a nicotine product in any venue made up 55% of the group. Daily smokers made up 17% of the study participants as confirmed by their elevated cotinine levels (greater than 100 ng/mL urine). The remaining participants (28%) either resided with smokers and/or rode in an automobile with an individual smoking in the previous 24 h. Their cotinine levels were moderately elevated in some cases, particularly if they had ridden in a car with a smoker.
Conclusion:
The pilot study met our objectives of >90% participation and high correlation of urinary cotinine levels with questionnaire self-reports.
Introduction
Community colleges enroll 46% of US students, yet little is known about the smoking behavior of the students. The smoking status of students enrolled in the health professions at these colleges is of particular interest. Tobacco exposure among nurses and respiratory therapists, for example, has been found to exceed 13%.1,2 Since tobacco education is among the initiatives encouraged for health professionals, the purpose of this study was to develop an experimental laboratory, combined with a questionnaire, to help students appreciate the significance of various types of tobacco exposure.3,4 The laboratory protocol addresses limitations in the current literature as to the actual tobacco exposure among a group currently termed “second-hand smokers.” 5 Our goal was to introduce students to the “gold standard” of a two-dimensional study in which self-reports of tobacco exposure are compared to their own urinary biological cotinine assay (Figure 1).
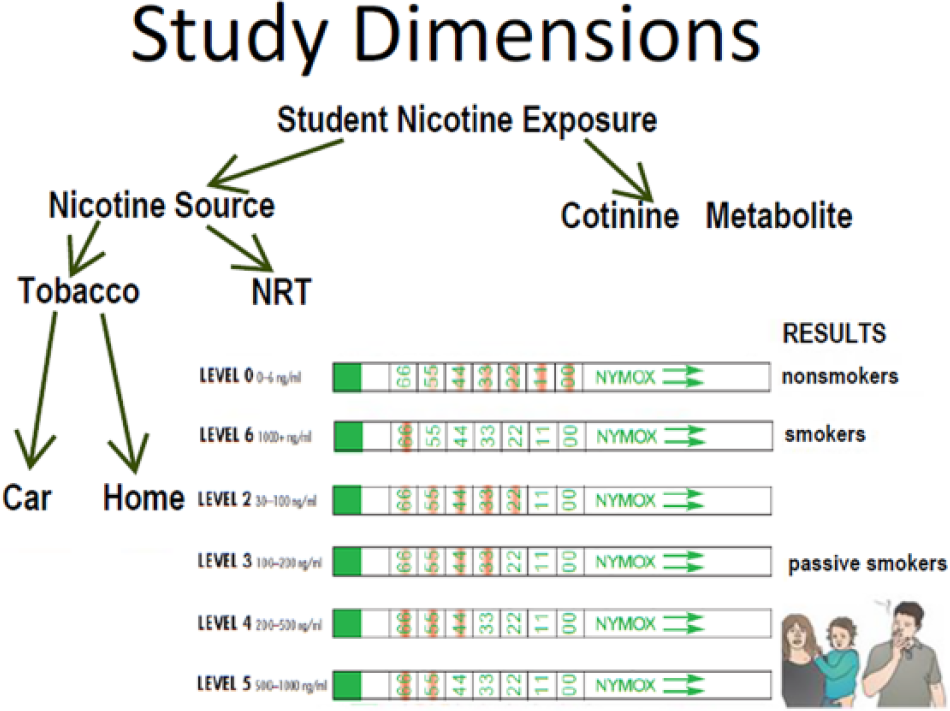
Two-dimensional confirmation of student tobacco exposure.
Allied health students (medical assistants, respiratory therapists, surgical technicians) were selected as the initial test group for a pilot study of an educational laboratory suitable for healthcare curriculums. The quantitative goal of the pilot study was >90% student participation since the urinary cotinine immunoassay would be conducted at home by the students. This novel departure from the usual procedure described in the literature was hoped to provide participants with an opportunity to share the results with family members. Most smokers are actually quite surprised that there is a test capable of confirming tobacco smoke exposure in both the smoker and in the family members in the immediate environment. Key features of the laboratory design were to include a questionnaire on recent tobacco/nicotine use combined with a rapid analysis of urinary cotinine. It was expected, as a study goal, that smokers would exhibit high levels of cotinine and that nonsmokers would exhibit no measurable cotinine when compared to cotinine control standards. Cotinine, the primary proximate metabolite of nicotine, is a useful biomarker to monitor active and passive exposure to environmental tobacco smoke. Cotinine is not a natural substance that would be found in the human body unless an individual had been exposed to a nicotine source. Cotinine immunochromatographic test strips have been used for over a decade to preclassify the smoking status of patients prior to surgery.6,7 In those studies, diagnostic accuracy was found to improve by the combined use of self-reported smoking status and cotinine rapid testing (15 more true positive tests per 1000 patients). The test strips contain cotinine-specific monoclonal antibodies attached to 40-nm colloidal gold particles. Test strips, initially dipped into a urine sample, absorb a uniform amount of urine. Any cotinine present in the urine sample binds with the anti-cotinine antibodies subsequently migrating up the laminated region of the strip by capillary action over 5–10 min. The antibody-coated colloidal gold particles function as both a carrier and a visual detection system.
Methods
The pilot study was initiated 10 months after all eight of the college campuses became 100% tobacco free so that nonsmokers could claim no tobacco exposure in any venue. A guided-inquiry laboratory was designed for a 5-week applied microbiology course required of all allied health students. The laboratory was relevant to the course competency in which students were expected to perform diagnostic procedures of body fluid specimens. The laboratory course, repeated six times a year, typically enrolled 15 students.
After a brief in-class training session using cotinine control standards, participants were instructed to conduct the cotinine immunoassay themselves at home using their own first-morning urine sample. Participants were instructed that cotinine immunoassay is considered an “acute” test effective in detecting nicotine exposure in the previous 24 h. Also, their urine sample should be collected before consuming any fluid, food, or medications in order to minimize any diet interference with the results. Participants were taught how to interpret the strips using control solutions of cotinine (0, 400, or 2000 ng cotinine/mL; TobacAlert strips and cotinine standards supplied by Nymox Pharmaceutical Corp, St.-Laurent, Quebec, Canada).
In conducting the immunoassay, participants practiced dipping a strip into a urine control sample to a depth of no more than 0.5 inch (1 cm) for 20 s. They were cautioned that unlike conventional urinalysis, only the tip of the strip was to be exposed to the urine solution. The strip was then removed and placed flat on a nonabsorbent surface in order to develop for 10–15 min until a blue indicator band substantially faded or disappeared as described in the procedure provided by the manufacturer. 8 The presence of many pink lines starting at the base of the strip indicated that there was no cotinine present in the sample, typical of a nonsmoker. Only one pink line at the top of the strip indicated that cotinine levels exceeded 1000 ng/mL, typical of a daily smoker.
Informed consent, approved by the school’s Institutional Review Board, was provided. Participants were informed that they could withdraw from the study at any time without penalty. A questionnaire was provided that consisted of six questions about tobacco exposure in the previous 24 h (Figure 2). The questionnaire was to be returned to the instructor along with the participant’s developed urine strip. Questionnaire responses were subsequently scored by the instructor. Questions ranged from personal use of a nicotine product (Questions 1–2), to riding in an automobile where a person was smoking or recently smoked (Questions 3 and 4, respectively), and/or to visiting or residing in a home with a person smoking or where a person had recently smoked (Questions 5 and 6, respectively). Individuals who answered “NO” to all six questions were scored as “NONSMOKERS” (at least within the context of the previous 24 h). Individuals who answered “YES” to Questions 1 and/or 2 where scored as “SMOKERS.” Individuals who answered “NO” to Questions 1 and/or 2 but answered “YES” to any of Questions 3–6 were scored as “AT RISK NONSMOKERS.”

TobacAlert urine immunoassay questionnaire.
Results
Quantitative summation for the 24-month study period is shown in Table 1. The 161 participants (88% of whom were female) were classified into three categories: (1) Nonsmokers (55%), (2) Smokers (17%), and (3) At-risk nonsmokers (28%). Cotinine assay results for all 89 nonsmoker respondents reflected their questionnaire responses in that cotinine levels were essentially below the level of detection (Levels 0 or 1) similar to the negative cotinine control solution (Figure 3).
Summary of cotinine results (24 months).

Based on Figure 2 questionnaire: Nonsmoker NO to all six questions; Smoker YES to Question 1 or 2; At-Risk NO only to Question 1 or 2.
TobacAlert Levels of 3–6 (100–2000 ng cotinine/mL urine).
TobacAlert Levels of 0 and 1 (below limit of detection).
The chi-square statistic is 116 for Nonsmoker/Smoker; p value is <.00001; result is significant at p < .01; http://www.socscistatistics.com/tests/chisquare2/Default2.aspx.
Respondents enrolled in 12 Allied Health Medical (AHM) 220 Applied Microbiology Courses from April 2014 to March 2016.

Typical response and TobacAlert assay for a “Nonsmoker.”
The 27 smoker respondents exhibited cotinine levels exceeding 100 ng cotinine/mL urine (Levels 3–6), typically exhibiting Level 6 (equivalent to >1000 ng cotinine/mL urine as in the high cotinine control solution). A representative comment from this group was, “Unfortunately, I am a smoker. This is what I expected to see on the test strip.” Only one respondent circled both Questions 1 and 2, indicating dual use of an e-cigarette. One respondent circled only Question 2 with the following comment: “I had a feeling it would be that high because I chew tobacco. Thankfully, I’m in the process of quitting.” Occasionally, participants would discuss the idea of smoking cessation: “That was the result I was expecting. Sadly, I do smoke and after seeing this and also hearing in class that some healthcare providers won’t hire you if you smoke makes me want to quit smoking.” Participants also commented about their experiences of socializing with other smokers: “I expected to be a little high but not at the highest. I am around people who smoke daily and I myself smoke occasionally to calm my anxiety but I didn’t expect it to be that high.”
The third category consisted of 45 respondents who answered “NO” only to the first two questions and “YES” to one or more of Questions 3–6, admitting to being either in the presence of a smoker or in the home or automobile where a person had previously smoked. Since the cotinine results for 77% of this group were nearly below the limit of detection of the rapid immunoassay (Level 1), participants were classified as “At Risk” Nonsmokers. Members of this group expressed concern about second-hand smoke exposure: “I don’t smoke but my boyfriend does so every day I am exposed to smoke.” The highest cotinine result for this group (equivalent to 400 ng/mL urine) was observed for a participant who commented, “My boyfriend smokes a lot and does it in the bedroom when I’m asleep.” Most participants described their efforts to avoid second-hand smoke as follows: “I do not smoke and I do my best to avoid areas that people smoke in. My mother smokes, but only outside, therefore I’m not really exposed to the actual smoke.”
Since the course was 5 weeks long, students had 4 weeks after the initial training to complete the assignment. The 4 weeks provided an opportunity for some students to stop smoking before administering the TobacAlert cotinine test. Similarly, members of the at-risk group could refuse to ride in an automobile with a smoker before administering their TobacAlert cotinine test.
Discussion
The pilot study met the quantitative objective of >90% participation of the home-administered urinary cotinine assay. In addition, questionnaire responses and cotinine levels for nonsmokers and smokers were highly correlated. Participants who reported no environmental tobacco exposure (car or residence) in the previous 24 h exhibited cotinine immunoassay results similar to the zero cotinine standard. It should be noted that although this correlation would be expected, such a result is not typical in the literature since smokers (as identified by their high urinary cotinine levels) often report as nonsmokers on questionnaires. 9 Study participants who reported smoking or consuming any nicotine product in the previous 24 h exhibited positive (>100 ng cotinine/mL urine) on their self-administered urinary immunoassay. Results for this smoking group were similar to either the high-level cotinine standard (>1000 ng cotinine/mL urine) or to the mid-level cotinine standard (>100 ng cotinine/mL urine).
Participants were surprisingly forthcoming about their smoking status considering recent reports that the stigma of smoking often decreases the likelihood of such self-reporting. The promise of confidentiality provided by the Informed Consent may be a factor. Also, the students were curious about participating in a scientific study as both the investigator and as the subject. Smokers reported that it was an “eye-opening experience” to observe the lingering presence of nicotine metabolites in their body fluids. In addition, the immediate visual feedback of their exposure to nicotine sources reinforced the literature provided to them on the hazards of tobacco smoke exposure. 10 The study protocol of directly observing elevated urinary cotinine appeared to provide a rare transformative experience in which participants began to question routine behaviors. Examples include “at risk nonsmokers” who rode in a car with an individual smoking or who slept in a room while a person smoked. Participants visually confirmed that there is no safe exposure to environmental tobacco exposure. Furthermore, the cotinine dipstick provided “at-risk nonsmokers” with physical evidence that they could share with the smoker.
In summary, the success of this pilot study adds to the medical literature as an effective protocol to improve accuracy in tobacco studies. Participation >90% was highly desirable since the literature indicates that smokers are typically reluctant (due to social stigma) to participate or to accurately report their tobacco exposure. The success of this study further suggests a novel approach that could be used to assess smoking status in physician offices. Typically, urine samples are collected from patients and then assayed by the medical assistant. The patient independently completes a questionnaire about tobacco smoke exposure where false denial of smoke exposure is common. Perhaps patients should be permitted to participate (or at least to watch) the urinary cotinine assay in order to observe the lingering presence of a nicotine metabolite in the case of a smoker. Furthermore, “at risk nonsmokers,” who had recently ridden in the car with a smoker (such as pediatric patients or pregnant women), could be alerted to elevated cotinine levels and environmental tobacco exposure.
Limitations of the pilot study were that the protocol was evaluated at only one college site and that the study size was limited to class enrollment over 24 months. For these reasons, the authors do not claim to have quantified smoking among US allied health students. Hopefully, this novel protocol will aid tobacco scientists in such studies. The Nursing Division of the college, though, concluded that the study provided sufficient confirmation that allied health students benefit from in-depth training on the hazards of tobacco smoke. Due to the high student participation and acceptance, the pilot-study protocol was successful and the laboratory was subsequently incorporated into the course curriculum.
Footnotes
Acknowledgements
The authors would like to thank the student participants for their forthrightness and dedication to the project. This article was presented at the 22nd Annual Meeting of the Society for Research on Nicotine and Tobacco, Chicago, IL, 4 March 2016.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Institutional Review Board of Delaware County Community College (IRB# 2015-0013). Approval was Exempt (Category 4). Contact: Christopher Tokpah, PhD, Chair IRB.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supplies for the pilot study were purchased by mini-grant awards by the college during 2014 and 2015.
Informed consent
Written informed consent was obtained from all subjects before the study.