
Abstract
Objectives:
Because most research on long-term acute care hospitals has focused on Medicare, the objective of this research is to describe the Georgia Medicaid population who received care at a long-term acute care hospital, the type and volume of services provided by these long-term acute care hospitals, and the costs and outcomes of these services. For those with select respiratory conditions, we descriptively compare costs and outcomes to those of patients who received care for the same services in acute care hospitals.
Methods:
We describe Georgia Medicaid recipients admitted to a long-term acute care hospital between 2011 and 2012. We compare them to a population of Georgia Medicaid recipients admitted to an acute care hospital for one of five respiratory diagnosis-related groups. Measurements used include patient descriptive information, admissions, diagnosis-related groups, length of stay, place of discharge, 90-day episode costs, readmissions, and patient risk scores.
Results:
We found that long-term acute care hospital admissions for Medicaid patients were fairly low (470 90-day episodes) and restricted to complex cases. We also found that the majority of long-term acute care hospital patients were blind or disabled (71.2%). Compared to patients who stayed at an acute care hospital, long-term acute care hospital patients had higher average risk scores (13.1 versus 9.0), lengths of stay (61 versus 38 days), costs (US$143,898 versus US$115,056), but fewer discharges to the community (28.4% versus 51.8%).
Conclusion:
We found that the Medicaid population seeking care at long-term acute care hospitals is markedly different than the Medicare populations described in other long-term acute care hospital studies. In addition, our study revealed that Medicaid patients receiving select respiratory care at a long-term acute care hospital were distinct from Medicaid patients receiving similar care at an acute care hospital. Our findings suggest that state Medicaid programs should carefully consider reimbursement policies for long-term acute care hospitals, including bundled payments that cover both the original hospitalization and long-term acute care hospital admission.
Long-term acute care hospitals (LTACs) are acute care facilities that provide care for chronically critically ill patients for an extended period of time, typically greater than 25 days. 1 LTACs may best be known for intense respiratory care where patients are mechanically ventilated and, ideally, weaned from such care. The needs of LTAC patients are complex; hence, LTACs are an expensive setting of care. Medicare spent US$39,000 per LTAC visit in 2011, 1 compared to 1997, when the median case cost was US$28,499. 2 Because Medicaid coverage of LTACs is optional for states, coverage and reimbursement of LTAC services differ between Medicaid programs and merits further research. Georgia Medicaid does not distinguish between LTACs and other hospitals. Therefore, participating LTACs are reimbursed through the same diagnosis-related group (DRG) methodology used for all Georgia hospitals; there are no separate rules or requirements for LTAC coverage. 3
The majority of research on LTACs has drawn from samples of Medicare patients, with very few studies that include a Medicaid population. Findings on the costs and outcomes experienced by Medicare patients who received care at an LTAC are mixed. Kahn and Carson 4 found that a transfer to an LTAC was associated with lower post-acute care (PAC) (US$9463 lower) and total (US$13,442 lower) costs, but higher overall Medicare payments (US$15,592 higher). A study commissioned by the Centers for Medicare and Medicaid Services (CMS) found that patients referred to LTACs had higher costs and higher payments compared to similar patients who were not transferred to LTACs, but that the magnitude of the difference varied by the patient’s primary diagnosis. 5 Despite the additional costs, studies have yet to conclusively show that LTAC-level care leads to desirable outcomes, including shortened lengths of stay, lower mortality, or fewer readmissions.1,6–10
New contribution
The nearly exclusive focus of the current LTAC research on the Medicare population and program has resulted in a dearth of studies on LTAC services for the Medicaid population. To our knowledge, only two studies have focused on LTAC care for Medicaid beneficiaries. A report on California Medicaid’s program found that in 2008, 4463 dual-eligible Californians received care at an LTAC at an average cost of US$51,446 per patient (all Medicare spending). 11 In another descriptive analysis, Liu et al. 2 reported that in 1997, 9.4% of all LTAC discharges nationally were for Medicaid beneficiaries. The authors also noted that the median length of stay for Medicaid patients was 40.2 days, compared to 30.4 days for Medicare beneficiaries.
This gap in the literature is important because outcomes, costs, and utilization of Medicare beneficiaries at LTACs may not be representative of the Medicaid population. With very little research on Medicaid beneficiaries and LTACs, state policy makers are left with evidence that is potentially not representative of the population for which they are making coverage decisions. Furthermore, given that patients who receive care at LTACs are some of the most high-cost/high-need beneficiaries, policy makers should place an emphasis on this population if they hope to lower costs for their Medicaid program. Knowing which Medicaid populations receive care from LTACs and their associated outcomes could inform coverage decisions, payment models, prior authorization criteria, and coordination of care initiatives for state Medicaid programs. In addition, if many Medicaid LTAC patients are also eligible for Medicare, this research could inform federal–state joint policies intended to improve care for this vulnerable population.
Research objective
The objective of this research is to describe the Georgia Medicaid population who received care at an LTAC, the type and volume of services provided by these LTACs, and the costs and outcomes associated with these services. For those with select respiratory conditions, we also compare costs and outcomes to those of patients who received care for the same services in acute care hospitals (ACHs).
Our research builds on the premise that patients with select respiratory conditions may experience improved outcomes when receiving specialized care as compared to similar patients who receive non-specialized care. As mentioned previously, LTACs are unique in that they provide intense respiratory care for patients who require prolonged mechanical ventilation. 12 LTACs, as opposed to intensive care units (ICUs), may offer specialized multidisciplinary teams, advanced weaning protocols, and experience with a niche group of patients with similar and complex needs. 4 ICUs, on the other hand, may be more likely to stabilize the patient but serve a far greater variety of patient needs, thereby limiting their ability to specialize their care on one group. 4
Our comparative analysis focuses on a subset of the Medicaid population with select respiratory conditions. We seek to understand both the differences in the demographic and cost characteristics of those who are admitted to an LTAC as compared to those who receive care in alternative settings. Our work adds to that of previous studies, focused on Medicare patients, by assessing the value of LTACs for a different group of complex patients.
Methods
Data sources and study sample
We used Georgia Medicaid claims data from January 2011 through December 2012. Our study sample consisted of fee-for-service Medicaid members who were admitted to an LTAC. As of 1 July 2011, 39% of Georgia Medicaid members were enrolled in fee-for-service Medicaid. 13
Study design and measures
We performed a descriptive analysis to better understand the demographic characteristics, primary diagnoses, and total Medicaid costs for Medicaid patients who were served by LTACs. We constructed 90-day episodes of care based on an ACH visit that immediately led to an LTAC stay. (Start dates for the 90-day episode began at the LTAC visit for patients who were not transferred from an ACH.) This is a common approach in the literature as this patient population has complex needs and is commonly served by multiple facilities.5,14 We then performed an outcomes’ analysis of Medicaid members with one or more LTAC visits, including length of stay, place of discharge, 30-day hospital readmissions, and per-patient costs for patients admitted by each LTAC covered by the Georgia Medicaid program. (We excluded episodes where the patient was discharged to multiple LTACs within the same episode and all episodes that began on 30 September 2012 or later.) We determined the average length of stay at the originating ACH and the patient’s time at the LTAC. The place of discharge variable included five potential settings: (1) ACH; (2) PAC facility, which includes skilled nursing and inpatient rehabilitation facilities; (3) community, where the patient was discharged home or to a home health service; (4) death; and (5) all other. We defined 30-day readmissions as an admission to an ACH within 30 days of being discharged to the community. Readmissions that occurred beyond the 90-day episode window but were within 30 days of discharge were included. We limited our cost measures to patients who survived the 90-day episode and excluded dual-eligibles. Our data included only Medicaid costs; thus, cost estimates for dual-eligibles would have been inaccurate as the amount paid by Medicare was unobserved. Costs captured all Medicaid reimbursed medical payments for services beginning within the 90-day episode.
Finally, we conducted a comparative analysis to measure differences in outcomes and costs for patients with similar conditions who received care at an LTAC, compared with patients who remained at an ACH. We again analyzed the length of stay, place of discharge, 30-day hospital readmissions, and per-patient costs for patients in both these settings and tested for statistical significance between both groups for each variable. We focused on episodes that originated at the ACH and had no previous LTAC or skilled nursing facility admissions during the 2-year time frame. ACHs were selected if the facility was located within or bordering the counties in which any of the LTACs are located. In order to create similar samples between the ACH and the LTAC, we retained only admissions with at least a 14-day length of stay and limited our comparative analysis sample to admissions for one of five respiratory-related DRGs. These five DRGs constituted approximately 45% of all Georgia Medicaid LTAC admissions and included the following: (All DRG codes are from the Tricare version 30 DRG grouper.)
DRG 542—tracheostomy with mechanical ventilation for more than 96 h or principal diagnosis except face, mouth, and neck
DRG 565—respiratory system diagnosis with ventilator support for more than 96 h
DRG 87—pulmonary edema and respiratory failure
DRG 541—extracorporeal membrane oxygenation or tracheostomy with mechanical ventilation for more than 96 h or principal diagnosis except face, mouth, and neck with major operating room procedure
DRG 566—respiratory system diagnosis with ventilator support for less than 96 h
To examine differences in severity of illness between ACH and LTAC patients, we calculated the Chronic Illness and Disability Payment System + Rx (CDPS + Rx) score using 2011 and 2012 claims data. The CDPS + Rx incorporates demographic information, 15,000 International Classification of Diseases (ICD)-9 codes, and pharmacy data into diagnostic buckets in order to generate a risk score for each patient.15–17 We report average CDPS + Rx risk scores for each setting of care. As a sensitivity analysis, we restricted the range of conditions to conduct a sub-analysis using only one DRG (565—respiratory system diagnosis with ventilator support for more than 96 h).
This research was reviewed and approved by the Georgia State University Institutional Review Board.
Results
Descriptive analysis
We identified six LTACs that provided services to Medicaid members between 2011 and 2012. One LTAC specialized in neurological and spine care. Given that the diagnoses served by this LTAC were substantially different than the other five LTACs, and that respiratory care is more common nationally at LTACs, 18 we excluded this facility from the remainder of the analysis. The remaining five LTACs provided inpatient services for 458 Medicaid patients during the study period (see Table 1). Seventy-one percent of these patients were eligible for Medicaid due to blindness or disability. While approximately 52% of patients receiving LTAC inpatient services were dually eligible for both Medicaid and Medicare, the average age of patients receiving LTAC services was 56 years old. We calculated the total 2-year Medicaid expenditures for non-dual members who received care from an LTAC as a benchmark for their total Medicaid costs. The median total Medicaid cost for these members was US$149,312. The range of expenditures was wide, from US$86,811 in the 25th percentile to US$242,927 in the 75th percentile.
Descriptive characteristics, outcomes, and costs of patients who received LTAC inpatient services.
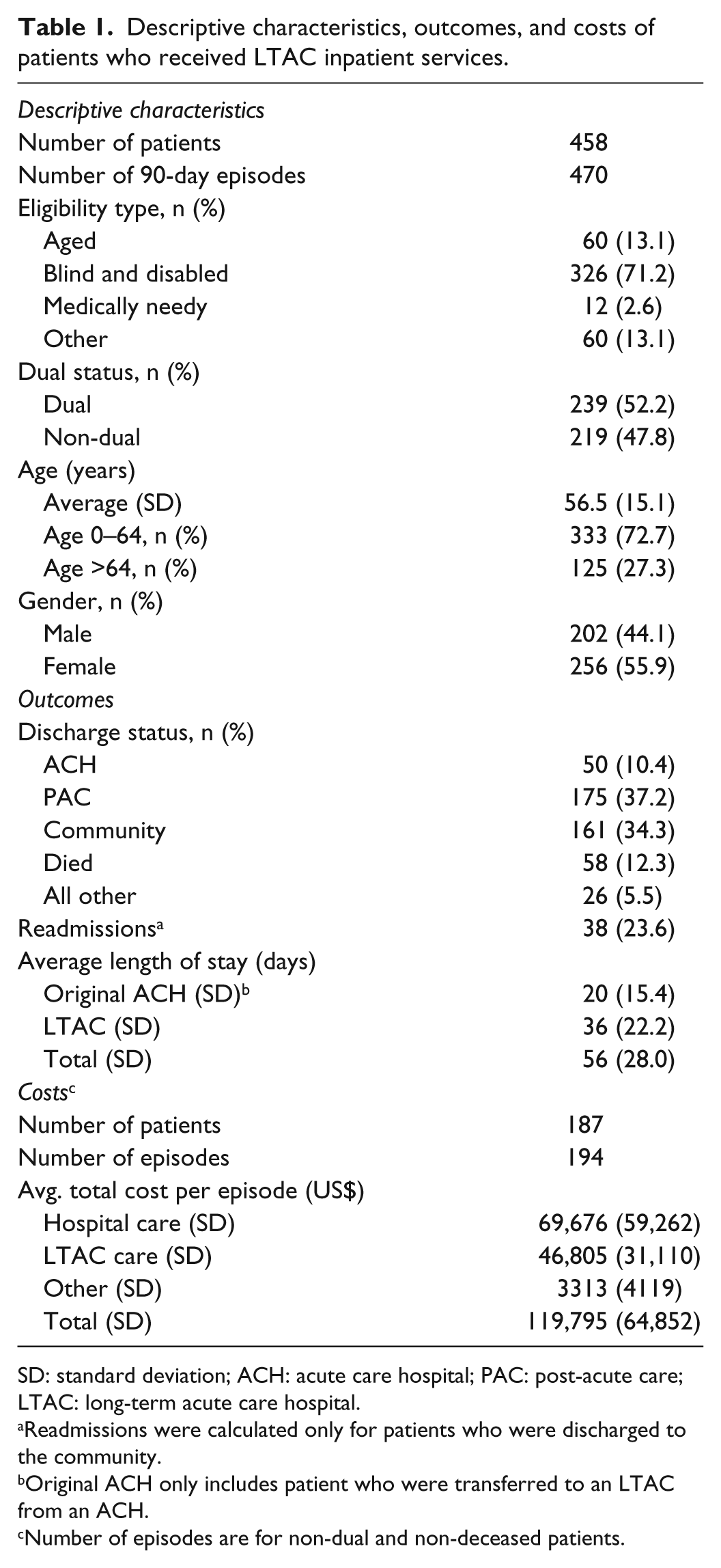
SD: standard deviation; ACH: acute care hospital; PAC: post-acute care; LTAC: long-term acute care hospital.
Readmissions were calculated only for patients who were discharged to the community.
Original ACH only includes patient who were transferred to an LTAC from an ACH.
Number of episodes are for non-dual and non-deceased patients.
Outcomes analysis
The five LTACs admitted 458 patients for 470 episodes, ranging from 46 to 258 episodes at each LTAC. Overall, 37.2% of the patients were discharged to another PAC, and 34.3% were discharged to the community. Just over 10% were discharged back to an ACH, 12.3% died, and 5.5% had other discharge statuses. Of the 161 patients who were discharged to the community, 38 (23.6%) were readmitted to an ACH within 30 days. There were 47 readmissions among these 38 patients, indicating multiple readmissions for certain patients.
The average length of stay at an ACH prior to discharge to an LTAC was 20 days. Once at the LTAC, Medicaid patients stayed for 36 days on average. Among the five LTACs, the average length of stay ranged from 29 to 40 days.
The average overall cost of a 90-day episode for a non-dual not deceased Medicaid member, including ACH, LTAC, and other costs, was US$119,795. This figure includes average ACH costs of US$69,676, LTAC costs of US$46,805, and all other costs (including any outpatient services at any provider) of US$3313.
Comparative analysis
The LTACs treated 211 respiratory-related episodes for 208 patients in 2011 and 2012 (see Table 2) compared to 821 episodes for 808 patients at ACHs. Patients who were treated at an LTAC were older and more likely to be eligible for Medicaid through a disability and had higher risk scores on average than patients who remained in the ACH. The average risk score among the patients treated at an LTAC was 13.1, compared to 9.0 for patients who stayed at the ACH (p < 0.01). While the distribution of the five DRGs was different between the ACH and LTAC groups, the risk scores within each DRG were significantly higher for those that received care at an LTAC.
Comparison of risk scores, discharge status, and readmissions for patients who received ACH only versus ACH and LTAC inpatient services for select respiratory conditions.

ACH: acute care hospital; LTAC: long-term acute care hospital; SD: standard deviation; CDPS + Rx: Chronic Illness and Disability Payment System + Rx.
Tests of statistical significance for discharge status and readmissions are chi-squared tests. A two-tailed t-test was used for differences in average risk scores. Certain figures are suppressed to protect patient confidentiality because of low observation numbers.
DRG 542—tracheostomy with mechanical ventilation for more than 96 h or principal diagnosis except face, mouth, and neck.
DRG 565—respiratory system diagnosis with ventilator support for more than 96 h.
DRG 87—pulmonary edema and respiratory failure.
DRG 541—extracorporeal membrane oxygenation or tracheostomy with mechanical ventilation for more than 96 h or principal diagnosis except face, mouth, and neck with major operating room procedure.
DRG 566—respiratory system diagnosis with ventilator support for less than 96 h.
CDPS + Rx scores were calculated for 807 patients who remained at the ACH.
Readmissions were calculated only for patients who were discharged to the community.
p < 0.01.
Among the comparison group, 51.8% of episodes at ACHs resulted in a discharge to the community, compared to 28.4% of LTAC admissions (p < 0.01; see Table 2). LTACs discharged patients more frequently to another PAC (37.4% versus 13.9%; p < 0.01), while a greater proportion of ACH patients died before being discharged (18.2% versus 15.6%; p < 0.01). Of the 425 patients discharged to the community from ACHs, 87 (20.5%) were readmitted within 30 days of discharge. However, because there were 105 total readmissions, it is clear that some patients experienced multiple readmissions. LTACs discharged 60 patients (28.4%) to the community, 14 (23.3%) of whom were readmitted within 30 days of discharge for 18 total readmissions. Differences in readmissions rates between ACHs and LTACs were not statistically significant.
Non-deceased patients who received all their care at the ACH had an average length of stay of 38 days, compared to non-deceased patients admitted to an LTAC who had an average length of stay of 19 days at the ACH followed by 42 days at the LTAC (see Table 3). The length of stay at the ACH varied by discharge location. For example, those individuals discharged to the community from the ACH or LTAC had an average length of stay of 37 and 56 days, respectively, compared to those discharged to a PAC (42 and 64 days). Among non-dual not deceased patients, the average total cost of a 90-day episode at an LTAC was US$143,898, compared to US$115,056 for patients who remained at the ACH. Costs related to the original hospitalization and post-discharge from the LTAC were lower on average for LTAC patients compared to those that remained at the ACH.
Comparison of length of stay and costs for patients who received ACH only versus ACH and LTAC inpatient services for select respiratory conditions, by discharge location.

ACH: acute care hospital; LTAC: long-term acute care hospital; SD: standard deviation; PAC: post-acute care.
Tests of statistical significance between overall ACH only and ACH and LTAC are two-tailed t-tests. Length of stay totals may not sum correctly due to rounding errors. Length of stays include non-deceased patients only, and costs include non-deceased and non-dual patients only. Certain figures are suppressed to protect patient confidentiality because of low observation numbers.
p < 0.1; **p < 0.01.
The results of the sensitivity analysis using only DRG 565 were consistent with the comparative analysis presented above (data not shown). Among 73 LTAC and 202 ACH episodes, a greater proportion of patients at ACHs were discharged to the community (59.7% versus 32.9%). The average combined inpatient length of stay was 59 days at LTACs versus 25 days at ACHs. Readmission rates were higher among LTAC patients (20.8%) than ACHs (13.0%), although sample sizes were small (24 and 123 patients were discharged to the community, respectively). Finally, average 90-day costs among non-dual not deceased patients were higher at LTACs (US$169,467) than at ACHs (US$76,304).
Discussion
Due to a lack of studies in the literature, little is known about the population of Medicaid patients who receive care at LTACs. Even less is known about the costs or outcomes of their care. Our study contributes to the literature on LTAC patients by describing the Medicaid population in Georgia who receive care at LTACs. We also compared costs and outcomes for Medicaid patients receiving select respiratory care in LTACs as opposed to those receiving similar care in an ACH.
Our study revealed that the Medicaid population seeking care at LTACs is markedly different than the Medicare populations described in other LTAC studies, not just based on patient age. Of the Medicaid patients who received care in Georgia LTACs during the study period, we found that 71% of them were blind or disabled. Our study also showed more patients discharged to the community (34.3%) than prior studies of Medicare patients (22%), 6 as well as a much lower mortality rate—12.3% as opposed to 48.2%−52.2% found by Kahn et al. 7 However, we found readmissions and costs to be higher for Medicaid patients than those found in prior studies of Medicare patients.2,7,9 In fact, the average episode payments to an LTAC were approximately 20% higher for this population than Medicare’s average payment in 2011 (US$46,805 versus US$39,000). 1 Although many reasons may exist for these differences, they demonstrate that prior research using Medicare patients may not be appropriate for informing state Medicaid policy for LTAC coverage.
In addition to differences with the Medicare population, our study also revealed that Medicaid patients receiving select respiratory care at an LTAC were distinct from Medicaid patients receiving similar care at an ACH. We found marked differences in terms of patient condition, discharge location, length of stay, and costs. In fact, our comparison of risk scores (both overall and within DRGs) shows that these Medicaid patients are more seriously ill than those who receive similar care at an ACH (13.1 for LTACs versus 9 for ACHs; p < 0.01). Therefore, it appears that LTACs are treating a different and more complex set of Medicaid patients.
The results of our study also imply that the Medicaid population receiving care at LTACs is more likely to experience certain outcomes than their Medicare counterparts. This is born out in the higher rate of discharge to the community for this population (34.3%) as compared to Medicare patients (22%). However, it is not clear why readmission rates are higher for Medicaid patients. It may be that they are more likely to be disabled than those on Medicare or that their economic condition makes them less likely to seek appropriate and timely follow-up care with their primary care physician. Our comparative analysis with ACH patients does show LTAC Medicaid patients to have more serious conditions than their ACH counterparts, but we did not have information on risk scores for Medicare patients to make similar comparisons.
Our results have implications for providers and policy makers. Although not required to do so, LTACs in Georgia seemed to limit their Medicaid admissions to respiratory cases of greater complexity than those observed in an ACH. It is possible that physicians and hospitals are only referring these difficult cases to LTACs, because they believe that their patients are likely to receive better care, or that LTACs are screening for these patients. In Georgia’s case, it may not be necessary for the state Medicaid agency to impose admission restrictions on LTACs. In fact, Georgia places no more admission restrictions on LTACs than they do for other acute care facilities. Finally, much of the added expense of episodes that involve an LTAC transfer can be attributed to the Medicaid program’s practice of paying two separate DRGs, which may only save costs if the transfer is able to avoid an outlier payment to an ACH. Therefore, Medicaid programs may want to consider bundled payments for LTAC transfers. A bundled payment would avoid paying two separate DRGs, would cover transfers back to the original ACH—which happened frequently in our study population (10.4%)—and would cover readmissions post-discharge to the community.
There are several limitations to this study. We only examined claims data for Georgia Medicaid patients enrolled in fee-for-service Medicaid; thus, our results may not be generalizable to Medicaid patients in other states or in managed care. More specific to our data, we excluded episodes where a patient was discharged to multiple LTACs within the same episode. Although this was likely a very small number of patients, it removes a potentially informative population from our analysis. In addition, costs were calculated only for non-dual Medicaid patients, as we did not have access to Medicare payment information, the primary payer for dual-eligibles. Finally, our sample size for comparative analysis was small, thereby limiting our ability to discuss associations between settings of care and patient outcomes. Additional work including modeling that controls for the impact of demographic and socioeconomic factors along with patient severity is needed for more robust discussions that assess the value of LTAC care on patient outcomes.
In spite of these limitations, our study found that Medicaid patients who receive care at an LTAC are different from Medicare patients, as well as Medicaid patients receiving comparable care at an ACH. These findings may be informative to providers and policy makers when determining who is best suited for LTAC care and what services Medicaid should cover. However, further research is needed to determine whether these differences between populations contribute significantly to the differences in outcomes and costs that we observed. Specifically, whether patient risk scores and other demographic differences are predictive of outcomes and costs for this population needs to be researched and analyzed. Further research should also focus on Medicaid patients from multiple states in order to determine whether our findings are generalizable to the broader Medicaid population and thus informative for providers and state Medicaid policy makers in other states.
Footnotes
Acknowledgements
The authors thank The Georgia Health Policy Center Research Team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Georgia State University Institutional Review Board (334510).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is made possible by the Georgia Department of Community Health (DCH) through a contract managed by Georgia State University. DCH is not responsible for any misuse or copyright infringement with respect to the publication.
Informed consent
Informed consent was not sought for this study because it only involved secondary de-identified data.