
Abstract
Background:
Clostridium difficile infection is a healthcare-associated infection resulting in significant morbidity. Although immunosuppression is associated with Clostridium difficile infection acquisition and adverse outcomes, the epidemiology of Clostridium difficile infection in HIV-infected patients has been little studied in the era of antiretroviral therapy. This study identifies the risk factors for acquisition of Clostridium difficile infection in HIV-infected patients.
Methods:
A retrospective, propensity score–matched case–control study design was employed, with patients selected from our institution’s outpatient HIV clinic. Clostridium difficile infection cases were defined as having positive stool testing plus an appropriate clinical presentation. The propensity score was generated via multiple logistic regression from year of HIV diagnosis, age at first contact, duration of follow-up, gender, and initial CD4 count.
Results:
The 46 cases included were matched to a total of 180 controls. Prior antibiotic treatment was a significant predictor of Clostridium difficile infection (odds ratio: 13, 95% confidence interval: 3.49–48.8, p < .001) as was number of hospital admissions in the preceding year (odds ratio: 4.02, confidence interval: 1.81–8.94, p < .001). Having both proton pump inhibitor use and CD4 count <200 cells/µL significantly increased odds of Clostridium difficile infection in the multivariable model (odds ratio: 15.17, confidence interval: 1.31–175.9, p = .021).
Conclusion:
As in the general population, frequent hospitalizations and exposure to antimicrobials are independent predictors of Clostridium difficile infection acquisition in patients with HIV. Additionally, low CD4 count and proton pump inhibitor use are new potentially modifiable variables that can be targeted for prevention of Clostridium difficile infection in future interventional studies.
Keywords
Introduction
Clostridium difficile infection (CDI) results in significant morbidity, mortality, and cost to the healthcare system. C. difficile was first linked to cases of antibiotic-associated diarrhea in the 1970s; since that time, it has become the leading cause of hospital-acquired diarrhea in the United States.1,2 In 2008, the acute-care direct costs of CDI in the United States were estimated to be US$4.8 billion. 2 As the prevalence of CDI has grown, new epidemic variants have emerged, in particular, the ribotype 027 strain. 2
CDI is thought to occur as a direct result of disturbing fecal microbiota, enabling overgrowth of C. difficile and toxin expression; this has been most strongly associated with antibiotic use. However, several other risk factors have been associated with the development of CDI, including gastric acid suppression, advanced age, hospital exposure, and deficits in cellular or humoral immunity.3–6
In HIV patients, CDI is the leading cause of bacterial diarrhea.3,7 In the pre-antiretroviral therapy (ART) era cohort studies showed a nearly doubled rate of CDI in HIV+ patients than in general inpatients1,4,8–10 despite roughly similar colonization prevalence.4,11 Since ART use has become more prevalent, this association has become less pronounced.1,4,12 Sanchez et al. 7 found an incidence rate of 4.1 cases per 1000 patient-years in a cohort from 1992 to 2002 and found that the incidence rate decreased with increasing CD4 counts. Many factors have been proposed to contribute to a higher rate of CDI in HIV patients, including depressed immune function, increased hospital exposure, and increased antibiotic use. In the pre-ART era, CD4 count <50 was shown to be an HIV-associated, independent risk factor for CDI acquisition.1,13,14 During this time period, CDI recurrence rates in the general population were similar to those in HIV+ patients, even in the cases of low CD4 counts.4,15,16
There have been few epidemiologic studies done after ART increased in popularity and the ribotype 027 strain increased in prevalence. One such study examined incidence and HIV-associated CDI risk factors in a cohort of 4217 patients between July 2003 and December 2010. The incidence of CDI cases was 8.3 cases per 1000 patient-years, higher than the estimate from Sanchez et al. 7 The higher incidence was hypothesized to be related to increasing incidence of CDI in the general population as a result of increasing virulence of C. difficile strains. In this study, risk of CDI was found to be independently increased for CD4 count ⩽50 cells/mm3, residence in hospital or healthcare facility at the time of diagnosis, use of gastric acid suppression, use of immunosuppression, and use of clindamycin, fluoroquinolones, or macrolides. Recurrent CDI occurred in 13% of cases. 13
A 2015 Italian study done in inpatients showed a similar incidence of hospital-associated CDI between HIV and non-HIV patients at around 5.1 cases per 1000 HIV+ hospital admissions. Multivariable analysis within the HIV cohort showed only low gammaglobulin and low albumin to be independently associated with an increased risk of CDI development. 17
The increasing use of ART is likely to have changed the epidemiology for CDI acquisition, but there have been few epidemiologic studies of CDI in HIV-infected patients in the modern era. This study was undertaken to reexamine the relationship between HIV infection and CDI acquisition in the ART era.
Methods
Study design and procedures
We performed a retrospective case–control study in patients who were followed in the University of Michigan HIV primary care clinic. Cases were defined by positive stool testing between 1 January 2000 and 20 September 2014 for either the toxin(s) A/B or the tcdB gene plus symptoms of increased diarrhea, abdominal pain, or fever. Cases included both inpatients and outpatients. Cases were matched up to 1:4 to controls by a propensity score, which was calculated using multiple logistic regression on the following variables: year of HIV diagnosis, age at first contact, duration of follow-up, gender, and initial CD4+ T cell (CD4) count.
Chart review was done to evaluate cases and controls for potential risk factors. The variables for the cases were abstracted within 1 year of their CDI. The variables for the control patients were extracted within 1 year of the CDI of their matched case.
Recurrent CDI was defined as new symptoms and positive stool testing >14 days after but within 8 weeks of the index episode and after the initial symptoms resolved. 18 Severe CDI was defined as CDI occurring in a patient with age ⩾65, white blood cell count >15,000, absolute neutrophil count ⩽500, albumin ⩽2.5, serum creatinine ⩾1.5 times premorbid level, solid organ or bone marrow transplant within 100 days, chronic graft versus host disease, and/or treatment of rejection of solid organ transplant within the preceding 2 months.
Statistical analysis
All analyses were conducted in R, version 3.2.2 (R Foundation for Statistical Computing, Vienna, Austria). Simple and multiple conditional logistic regressions were used to identify variables associated with the development of CDI and other outcomes. The final multivariable model was built using backward elimination with a likelihood ratio test, using α < .05 as the cutoff for variable retention, and all variables were candidates for inclusion in the model. Interaction terms were evaluated and included in the final model where significant. A two-sided p value < .05 was considered significant for all tests.
Results
Between 20 September 1987 and 20 September 2014, 1456 patients were followed in the HIV clinic; within the study period, this amounted to 6461.9 patient-years. Of these, 46 were identified as having a case of CDI between 1 January 2000 and 20 September 2014, consistent with an incidence rate of 7.1 cases per 1000 patient-years. The 46 incident cases were matched with 180 controls. Baseline characteristics of cases and controls are compared in Table 1.
Patient characteristics.

CDI: C. difficile infection; PCP: Pneumocystis pneumonia; CMV: cytomegalovirus; MAC: Mycobacterium avium complex; COPD: chronic obstructive pulmonary disease; IBD: inflammatory bowel disease; PPI: proton pump inhibitor; IVIG: intravenous immunoglobulin; NNRTI: non-nucleoside reverse transcriptase inhibitor; NRTI: nucleoside reverse transcriptase inhibitor; ART: antiretroviral therapy.
All values given as percent (n) or value ± standard deviation.
There were 154 missing values.
Among CDI cases, 36 were male (78%), 9 were female (22%), and the mean age was 44 years. In total, 70% of CDI cases had a history of AIDS and 48% had a CD4 count of less than 200 at the time of CDI diagnosis. In total, 50% of cases were within 3 months of a course of antibiotics. In total, 78% of cases were using ART at the time of CDI and 32% were using a proton pump inhibitor (PPI). The average number of hospitalizations among case patients in the previous year was 2.6.
Unadjusted analysis of predictors of CDI is shown in Table 2. In the unadjusted analysis, elevated viral load at the time of CDI, number of hospitalizations in the previous year, days spent in the hospital in the previous year, having a CD4 count <200 at the time of CDI, use of antibiotics for both prophylaxis and treatment, use of PPI at the time of CDI, use of non-nucleoside reverse transcriptase inhibitor (NNRTI) at the time of CDI, and use of integrase inhibitors at the time of CDI were all significant risk factors for the development of CDI.
Unadjusted analysis of selected predictors for acquisition of C. difficile infection.
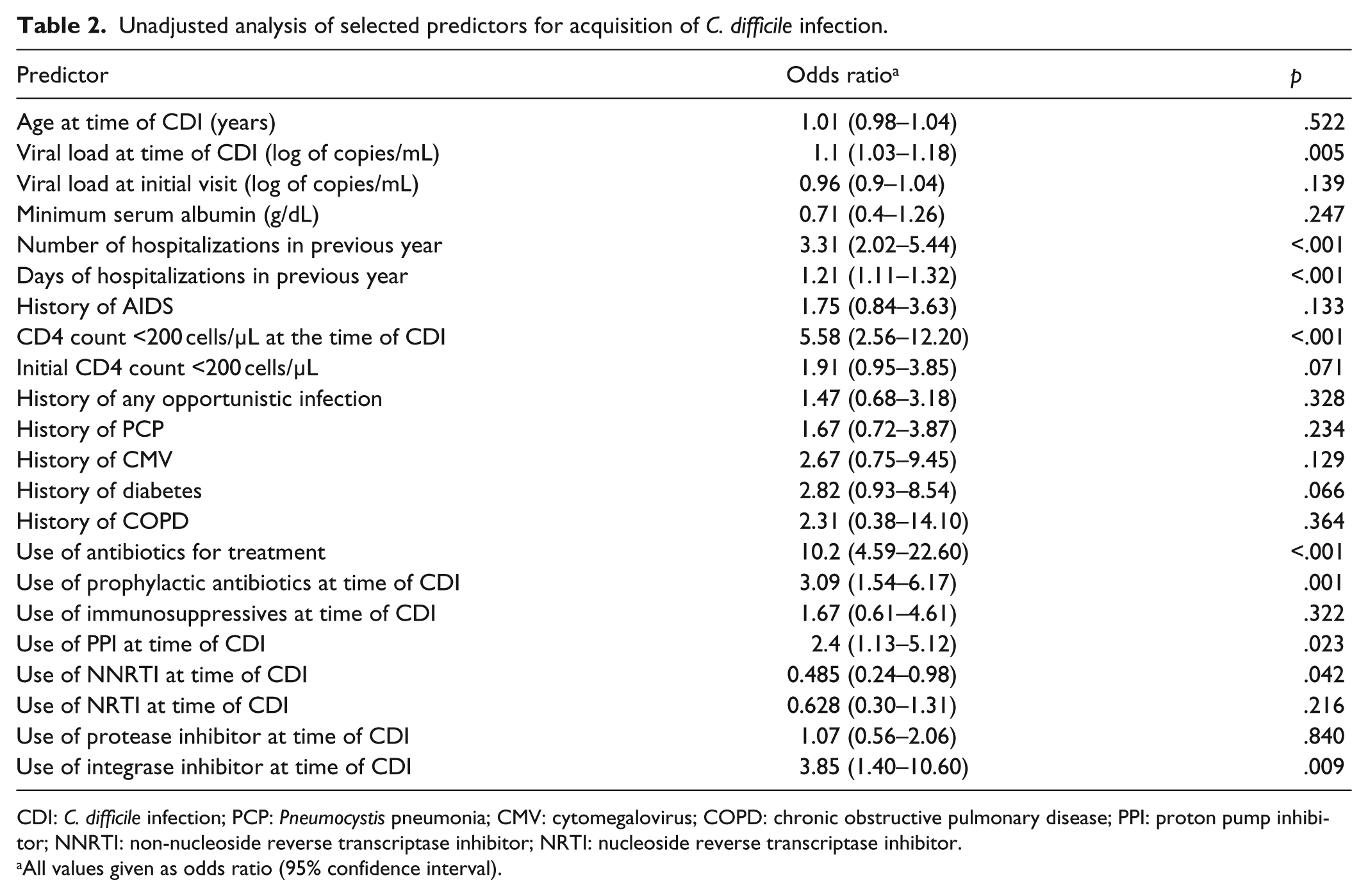
CDI: C. difficile infection; PCP: Pneumocystis pneumonia; CMV: cytomegalovirus; COPD: chronic obstructive pulmonary disease; PPI: proton pump inhibitor; NNRTI: non-nucleoside reverse transcriptase inhibitor; NRTI: nucleoside reverse transcriptase inhibitor.
All values given as odds ratio (95% confidence interval).
The final multivariable model for development of CDI is shown in Table 3. Adjusting for covariates, including age, prior antibiotic treatment was a significant predictor of CDI (odds ratio (OR): 13, 95% confidence interval (CI): 3.49–48.8, p < .001) as was number of hospital admissions in the preceding year (OR: 4.02, CI: 1.81–8.94, p < .001). Neither PPI use nor low CD4 count (<200 cells/µL) were independent predictors of CDI alone, but if both were present, an interaction existed that conferred a significantly increased risk of CDI in the multivariable model (OR: 15.17, CI: 1.31–175.9, p = .021).
Multivariable model for acquisition of Clostridium difficile infection with HIV.
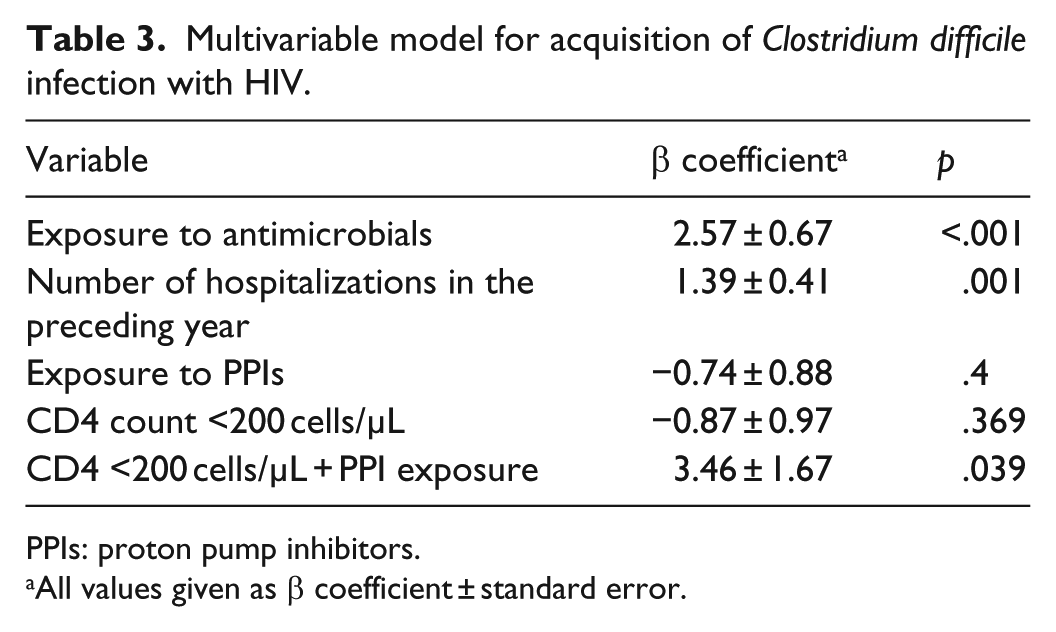
PPIs: proton pump inhibitors.
All values given as β coefficient ± standard error.
Severe CDI occurred in 10 cases (21.7%) and recurrent CDI occurred in 2 cases (4.3%). Only one death occurred (2.2%). Due to few numbers of severe and recurrent CDI cases, no further statistical analyses were done on these patients.
Discussion
Past studies have demonstrated that HIV infection is a risk factor for CDI and that ART use has not decreased this risk to that of the background population.12,17 Although there have been several epidemiologic studies examining CDI in HIV-infected patients, it is valuable to reexamine the relationship in the modern era, when both strains of C. difficile and control of HIV have changed. Our data revealed a similarly high incidence rate of CDI cases in HIV patients as that reported by Haines et al. 13 This likely reflects increased prevalence and virulence of the disease in the general population.
This study re-demonstrated the increased risk of CDI in patients with prior antibiotic and hospital exposure, a finding that has held true in HIV- and non-HIV-infected populations. The data also showed an interaction between CD4 <200 and PPI use. Prior studies have found CD4 counts <50 to be a risk factor for CDI, and higher CD4 counts were protective.
The interaction between CD4 count <200 and PPI use resulting in a 15.17-fold increased odds of CDI is notable. One hypothesis for this finding is that acid suppression allows a greater bacterial load to pass through the stomach, either by increasing counts of C. difficile itself or by increasing other bacterial species that disrupt the gut microbiota, and that deranged cellular and humoral immunity fails to prevent an infection. 2 Since we did not observe an increased risk with each variable in isolation, it is possible that either factor alone is not enough to cause an infection but that both together overwhelm the host defenses. Alternatively, it is possible that the incidence of CDI was too low to see more subtle independent associations, and a larger study would have more power to better tease apart these relationships. In prior studies, older age, use of antibiotics after diagnosis, use of PPIs, and strain of C. difficile were the most frequent risk factors for recurrence. 19 A larger sample would be needed to see whether this was true in our population as well.
Although this study showed an intriguing result, it had limitations. Due to the low frequency of CDI in our population, a case–control study was undertaken instead of a cohort study, which may have been more informative with respect to assessing risk associated with a given variable. We were not able to evaluate severe and recurrent disease due to low sample size of CDI. Although hospital- and community-acquired cases of CDI were included, there were too few samples to consider them separately. The serotypes of C. difficile were not tested but could give insight into whether more virulent strains of C. difficile contributed to lower incidence of infection. Additionally, previous studies have noted associations between hypoalbuminemia and hypogammaglobulinemia with CDI, but since these are not routinely checked on our patient population, these markers were unable to be examined in much detail. 17 Our study did note that patients with higher serum albumin were less likely to have contracted CDI, but the lack of statistical significance and significant number of missing values limited our ability to study this further.
In summary, this study demonstrated an increased risk of CDI associated with PPI use and CD4 count <200, in addition to previously known risk factors of antimicrobial use and frequent hospital exposure. These findings suggest new potential intervention targets to decrease risk of CDI in this population.
Footnotes
Acknowledgements
The authors would like to thank the University of Michigan Health System’s Medical Center Information Technology team for database support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board of the University of Michigan Medical School (approval number/ID: HUM00093724).
Informed consent
Informed consent was not sought for this study because our IRB waived this requirement, as it was low-risk retrospective research involving chart review only.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Claude D. Pepper Older Americans Independence Center (grant number AG-024824) and the Michigan Institute for Clinical and Health Research (grant number 2UL1TR000433). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.