
Abstract
Trichodysplasia spinulosa is a rare cutaneous disease caused by the trichodysplasia spinulosa–associated polyomavirus. It occurs more frequently in immunocompromised patients, particularly in solid organ transplants. A few successful treatments have been described in the literature. In our report, we present a biopsy-proven trichodysplasia spinulosa case in a kidney transplant recipient who rapidly responded to a reduction of his immunosuppressive therapy.
Introduction
Trichodysplasia spinulosa (TS) is a rare cutaneous disease characterized by folliculocentric papules with keratin spicules primarily involving the central face. This condition is associated with the trichodysplasia spinulosa–associated polyomavirus (TSPyV), although precise mechanisms remain unknown. Here, we present a case of TS in a kidney transplant recipient who rapidly responded to a reduction of his immunosuppressive therapy.
Case report
A 61-year-old man with a past medical history of a kidney transplant in 2015 for polycystic kidneys presented to the dermatology clinic with complaints of multiple asymptomatic skin-colored papules on the face and ears, and some slightly pruritic pink papules on the trunk and extremities. These lesions appeared 1 year after transplant and were progressing for the past 2 years. In the last months, he also noticed hair loss on his eyebrows and limbs. His immunosuppressive regimen included tacrolimus, mycophenolate mofetil (MMF), and prednisone.
On clinical examination, there were multiple millimetric folliculocentric hyperkeratotic skin-colored to pink papules on the face (Figure 1), ears (Figure 2), trunk and extremities (Figure 3). Some of the papules also had a white central spicule. Furthermore, alopecia was noted on the eyebrows and extremities. Cutaneous biopsies of the thigh and back showed dilated follicles with eosinophilic trichohyalin granules and keratin debris that were replacing the hair shaft (Figures 4 and 5). Unfortunately, our center could not provide us with the real-time polymerase chain reaction (PCR) targeting the viral protein 1 (VP1) gene, so the diagnosis of TS associated with immunosuppression was made by clinical and histological findings.

Folliculocentric hyperkeratotic skin-colored to pink papules on the face.

Folliculocentric skin-colored papules with central spicules on the ears.

Folliculocentric hyperkeratotic pink papules on the extremities.
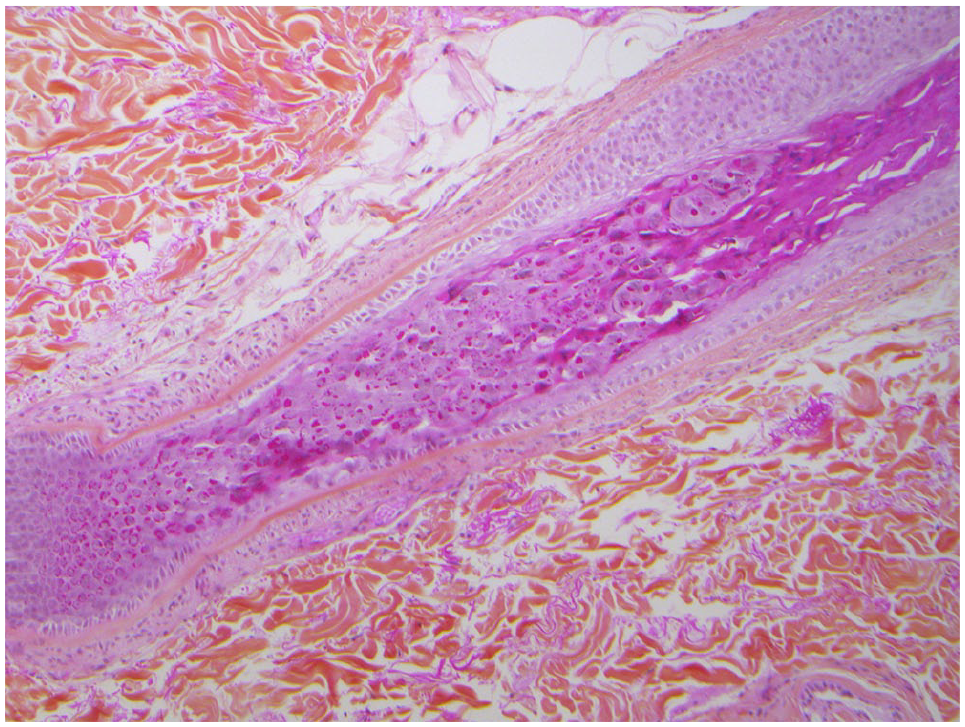
Cutaneous biopsy of the thigh showing dilated follicles with eosinophilic trichohyalin granules and keratin debris replacing the hair shaft (HPS: hematoxylin phloxine saffron staining, 20× magnification).

Cutaneous biopsy of the thigh showing dilated follicles with eosinophilic trichohyalin granules and keratin debris replacing the hair shaft (HPS: hematoxylin phloxine saffron staining, 40× magnification).
After a discussion with the patient’s nephrologist, she preferred a reduction of the immunosuppressive medication instead of treating with a systemic retinoid. The MMF was reduced from 720 to 360 mg twice a day, and the tacrolimus from 4.5 to 4 mg once a day. A topical tretinoin gel 0.1% was also applied daily on facial lesions. At follow-up, 4 months later, a spectacular improvement of the facial lesions was noted. However, many papules persisted on the trunk and limbs. At the 6-month follow-up, there was a complete resolution of the facial, ears, and trunk lesions (Figures 6 and 7). Because some of the papules still persisted on the extremities, the tretinoin gel was pursued there.

Complete resolution of the ears lesions.

Complete resolution of the nose lesions.
Discussion
TS is a rare entity first described in 1995 by Izakovic et al. 1 Seen in a renal transplant patient, it was regarded as a side effect of cyclosporine. In 1999, Haycox et al. 2 used electron microscopy to identify small (38 nm), intracellular virus particles in the cutaneous biopsies belonging to the Papovaviridae family. Even though many immunohistochemical analyses were realized, distinction between papillomaviruses and polyomaviruses could not be made at that time. In 2010, Van der Meijden et al. 3 used rolling-circle DNA amplification to isolate the virus from the spicules and named it TSPyV.
TS is almost exclusively observed in a context of immunosuppression, either in association with solid organ transplantations or hematologic malignancies. However, in 2014, one case of perioral TS was also described in a patient with the Gorlin syndrome undergoing treatment with vismodegib 4 and another case in a patient with systemic lupus erythematous under different immunosuppressants. 5 This condition affects adults and children equally, and seems to appear between 6 months and 9 years post-transplant or after a diagnosis of hematologic malignancy.6,7
The seroprevalence of TSPyV appears rather high in the general population, ranging from 70% to 90%, most frequently with exposure during childhood. 8 However, instead of being caused by the reactivation of the virus, TS is thought to result from a primary infection in immunosuppressed patients.9,10
Typically, TS diagnosis is made based on the combination of clinical and histopathologic evidence. However, other recent diagnosis methods—such as immunohistochemistry, scanning electron microscopy, and PCR—have been used to confirm the viral etiology. 11 Clinically, TS is characterized by an eruption of follicular flesh-colored or pink papules frequently featuring central keratotic spicules. It mainly affects the central face, ears, and, in a lesser proportion, the trunk and the extremities. The lesions are most often asymptomatic although occasionally associated pruritus has been reported. Typical complications include varying degrees of nonscarring alopecia, most frequently affecting the eyebrows, and skin thickening that can lead to a disfiguring leonine facies.12,13 Histopathology shows dilated hair follicles, with an expanded inner root sheath cells, keratotic debris, and enlarged eosinophilic trichohyalin granules. 13
There are currently no established guidelines regarding TS treatment. Case reports have shown successful results with topical cidofovir 1%–3%, oral valganciclovir, and reduction in the immunosuppressive therapy.13–15 Other reported therapies included spicule extraction, 16 oral and topical retinoids, and leflunomide. 15 Finally, topical steroids, tacrolimus, antibiotics, imiquimod, and oral minocycline showed little or no improvement.10,17 In our case, a conservative treatment was privileged. After careful review of the patient’s renal condition and discussion with his nephrologist, we reduced immunosuppression, and added a tretinoin gel for facial lesions. The results were impressive since the patient was almost clear of lesions after 6 months. Our case report demonstrates that an extensive case of TS can resolve completely with a more conservative approach. So, instead of adding another medication, if the nephrologist or transplant physician is more inclined to securely reduce the immunosuppression and monitor it, this therapeutic strategy could be tried first before undergoing more aggressive treatments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A written informed consent for the patient informations and images was provided by the patient.