
Abstract
A 69-year-old female with diabetes mellitus underwent off-pump coronary artery bypass grafting for old myocardial infarction and unstable angina with reduced left ventricular wall motion due to triple vessel disease. Although the saphenous vein graft was confirmed to be patent during surgery, it developed occlusion at the distal anastomotic site on postoperative first day. However, recanalization was achieved for this saphenous vein graft following the administration of direct oral anticoagulants in addition to antiplatelet therapy. Anticoagulant therapy, in addition to antiplatelet therapy, should be considered for preventing and dissolving thrombus in postoperative acute period, especially in high-risk patients for thrombotic graft occlusion.
Introduction
Anticoagulant therapy combined with antiplatelet therapy for the purpose of graft patency in coronary artery bypass grafting (CABG) is not recommended in the present guidelines.1,2 Moreover, the COMPASS-CABG study could not show any improvement of early graft failure with direct oral anticoagulants in addition to antiplatelet therapy, although it reduced major adverse cardiovascular events. 3 However, we encountered a very rare case of recanalization of once occluded distal anastomotic site of saphenous vein graft (SVG) in postoperative acute period following administration of anticoagulant therapy. Acute graft occlusion was suspected to be caused by thrombus formation at the anastomotic site of the SVG; therefore, this case was managed, without any invasive intervention, with direct oral anticoagulants in addition to antiplatelet therapy. Subsequently, the thrombus at the distal anastomotic site of the SVG was dissolved, and recanalization was achieved.
Case
A 69-year-old female with diabetes mellitus was diagnosed with inferior old myocardial infarction and unstable angina pectoris. The left ventricular wall motion was reduced and left ventricular ejection fraction was 45.8% in trans-thoracic echocardiography. Coronary angiography revealed the following triple vessel disease: total occlusion of segment 1, 90% stenosis of segment 6, and 50%–75% stenosis of segment 13 (Figure 1).
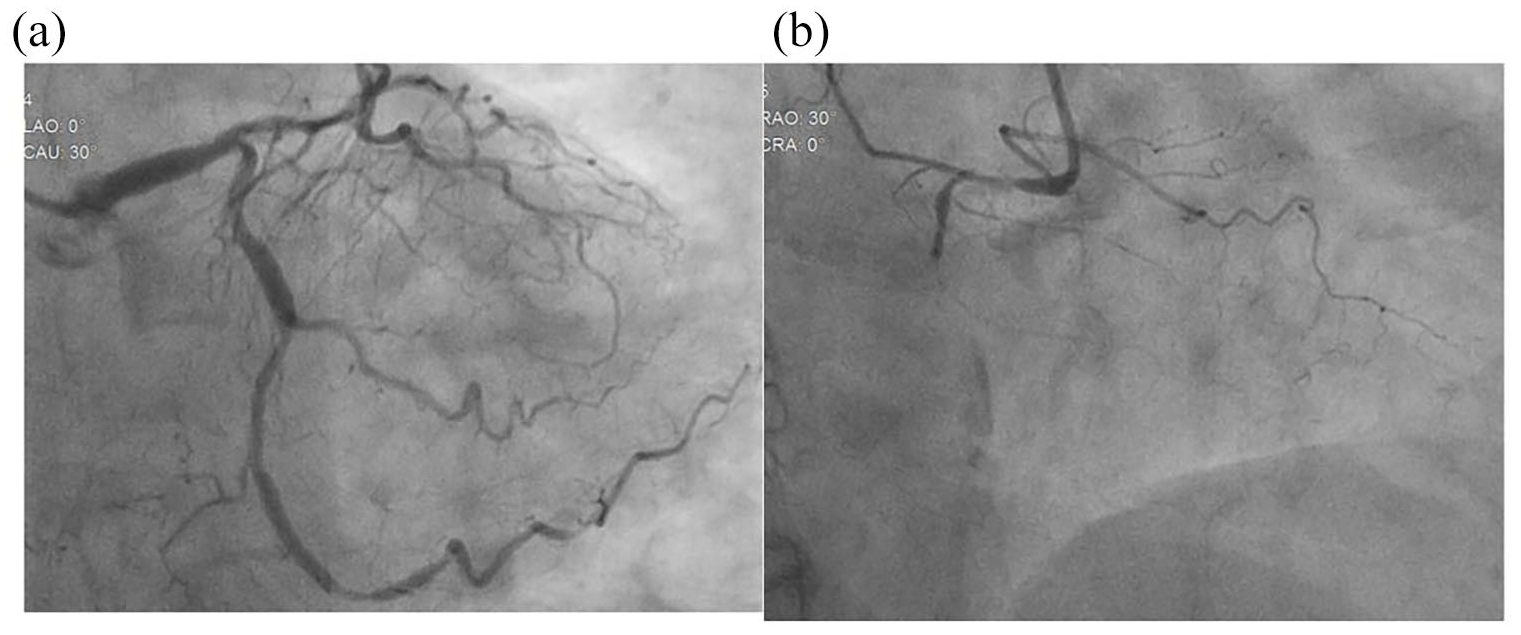
Preoperative coronary angiography of the LCA (a) and RCA (b). Angiography showed triple vessel disease with total occlusion of right coronary artery.
She underwent CABG using an off-pump technique: left internal thoracic artery to left anterior descending coronary artery, SVG to posterior lateral coronary artery (PL), and in-situ right gastroepiploic artery to posterior descending coronary artery. SVG was harvested by conventional manner, and the state of the SVG was normal. Moreover, the state of the coronary artery of each anastomotic site was normal. Graft flow, pulsatility index, and diastolic filling index measured with transit time flow meter were 26 mL/min, 1.8, and 65% in the left internal thoracic artery; 11 mL/min, 2.8, and 50% in the SVG; 9 mL/min, 4.3, and 36% in the right gastroepiploic artery, respectively.
She was transferred to the intensive care unit under stable hemodynamics. Tracheal tube was removed 5 h after surgery.
However, on postoperative first day, routine electrical cardiography revealed slight elevation of ST segment in inferior leads, and routine laboratory data showed elevation of creatine kinase up to 1343 U/L and creatine kinase-MB up to 112.9 U/L. Subsequently, emergent coronary angiography was performed, which revealed that the left internal thoracic artery to left anterior descending coronary artery and the in-situ right gastroepiploic artery to posterior descending coronary artery were patent. However, the distal anastomotic site of the SVG to PL was occluded (Figure 2). Distal perfusion area of the occluded anastomotic site of PL was relatively small, and additional invasive catheter intervention had risk of rupture of anastomotic site; therefore, direct oral anticoagulant (Edoxaban 30 mg/day) in addition to aspirin was initiated expecting thrombolysis. Her clinical course afterwards was quite stable, and trans-thoracic echocardiography revealed no remarkable asynergy in the left ventricular wall motion. Coronary artery computed tomography was performed on postoperative 20th day, and it showed good patency of all grafts including the distal anastomotic site of the SVG to PL (Figure 2). No major adverse cardiac event has occurred since.

Coronary angiography on postoperative first day (a) and coronary artery computed tomography on postoperative 20th day (b). The saphenous vein graft to PL (white arrow) was occluded at the distal anastomotic site in (a). However, the saphenous vein graft to PL (white arrow) achieved obvious recanalization without a collateral vessel in (b).
Discussion
SVG deteriorates over time due to “vein disease” such as intimal hyperplasia and atherosclerosis. 4 Anticoagulant therapy with warfarin in addition to antiplatelet therapy was tried to resolve graft failure; however, it could not improve SVG patency without preventing atherosclerosis of SVG in the post-CABG trial. 5 Consequently, guidelines do not recommend anticoagulant therapy in addition to antiplatelet therapy for graft patency at present.1,2
Conversely, early (<1 month) graft failure sometimes occurs, and the incidence of early SVG failure has been reported to range from 8% to 18%. 6 Anticoagulant therapy with rivaroxaban in addition to antiplatelet therapy could not show improvement of early graft failure in the COMPASS-CABG study. 3 However, the mechanism of early SVG failure is mainly thrombus formation due to endothelial injury of the SVG and slow flow of the SVG arising from caliber mismatch between SVG and native coronary artery.6,7 Therefore, whether anticoagulant therapy is meaningless in regard to the prevention of thrombus at the anastomotic site of SVG, especially in postoperative acute period, remains controversial. Moreover, it has been reported that additional anticoagulant therapy may be required in off-pump CABG because of its regional hypercoagulability. 8
In this case, the distal anastomotic site of the SVG to PL was occluded in postoperative acute period, although the SVG was confirmed to be patent during surgery in transit time flow meter findings under conventional state and proximal clamp state (not recorded as figure). In this case, acute SVG failure may have occurred due to thrombus formation because of caliber mismatch and CABG with off-pump technique. Anticoagulant therapy with direct oral anticoagulants in addition to antiplatelet therapy was chosen, expecting thrombolysis because invasive catheter intervention for the SVG failure had the risk of rupture of the anastomotic site. As a result, obvious recanalization of once occluded distal anastomotic site of the SVG was confirmed by less invasive coronary artery computed tomography on postoperative 20th day. To the best of our knowledge, this is the first case of confirming such a phenomenon in postoperative acute period including our experiences. Moreover, a previous study reported prompt removal of thrombus and recanalization of SVG in late postoperative period using direct oral anticoagulants. 9
Acute SVG failure may be caused by mechanisms such as thrombus formation due to endothelial injury of SVG, blood turbulence of SVG, and hypercoagulability with off-pump technique. Therefore, prevention and dissolution of thrombus using anticoagulant therapy in addition to antiplatelet therapy should be considered in postoperative acute period, especially in high-risk patients.
Conclusion
We encountered a very rare case of recanalization of once occluded distal anastomotic site of SVG in postoperative acute period following the administration of anticoagulant therapy. Prevention and dissolution of thrombus using anticoagulant therapy in addition to antiplatelet therapy should be considered in postoperative acute period, especially in high-risk patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.