
Abstract
Surgical resection appears to be the most effective treatment for early-stage non-small cell lung cancer. Recent studies suggest that perioperative pulmonary rehabilitation improves functional capacity, reduces mortality and postoperative complications and enhances recovery and quality of life in operated patients. Our aim is to analyse and identify the most recent evidence-based physical exercise interventions, performed before or after surgery. We searched in MEDLINE, EMBASE, CINAHL, Cochrane Library and PsycINFO. We included randomised controlled trials aimed at assessing efficacy of exercise-training programmes; physical therapy interventions had to be described in detail in order to be reproducible. Characteristics of studies and programmes, results and outcome data were extracted. Six studies were included, one describing preoperative rehabilitation and three assessing postoperative intervention. It seems that the best preoperative physical therapy training should include aerobic and strength training with a duration of 2–4 weeks. Although results showed improvement in exercise performance after preoperative pulmonary rehabilitation, it was not possible to identify the best preoperative intervention due to paucity of clinical trials in this area. Physical training programmes differed in every postoperative study with conflicting results, so comparison is difficult. Current literature shows inconsistent results regarding preoperative or postoperative physical exercise in patients undergoing lung resection. Even though few randomised trials were retrieved, treatment protocols were difficult to compare due to variability in design and implementation. Further studies with larger samples and better methodological quality are urgently needed to assess efficacy of both preoperative and postoperative exercise programmes.
Introduction
Lung cancer is the leading cause of cancer death in males, and in females, its mortality burden is as high as cervical cancer. 1 In 2012, an estimated 1.8 million people were diagnosed with lung cancer, resulting in 1.6 million deaths. 2 Lung cancer is the leading malignant cause of death in 93 countries, accounting for one-fifth of the total global burden of disability-adjusted life years from cancer. 2 Non-small cell lung cancer (NSCLC) 2 comprises 85% of all lung cancers. Up to 63% of patients diagnosed with lung cancer also present chronic obstructive pulmonary disease (COPD). 3 If we consider all stages of NSCLC, the prognosis is poor, with an overall 5-year survival rate of 15%. 4 Lobectomy for initial stages demonstrates higher survival rates, but only 15%−25% of patients are surgical candidates because of cardiopulmonary impairment due to coexisting COPD. Therefore, patients undergo medical treatment or marginal lung resection, with minor functional impact but possible ineffective control of disease.5–7 Furthermore, coexisting COPD is associated with increased postoperative morbidity and mortality.5,6
Improvements in early diagnosis and surgical techniques have increased post-surgery survival rates. Therefore, in recent years, there has been a growing interest towards interventions that aim at improving health-related quality of life (HRQoL) and lessening morbidity for patients affected by lung cancer, either before or after surgery.8,9
‘Pulmonary Rehabilitation (PR) is a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies, that include, but are not limited to, exercise training, education and behaviour change designed to improve physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviours’. 10 PR goals include minimising symptom burden, maximising exercise performance, promoting autonomy, increasing participation in everyday activities, enriching HRQoL and influencing long-term health-enhancing behaviour change.7,10 It is widely recognised that physical exercise is the cornerstone in PR programmes. 11
It has been shown that preoperative PR ameliorates functional parameters that establish operability in COPD patients; therefore, candidates for surgery could benefit from this functional improvement in terms of larger possible lung resection and lower incidence of postoperative complications.7,11
Recent guidelines by Spruit et al. 10 highlight findings of uncontrolled trials reporting that PR after lung resection surgery improves walking endurance and peak exercise capacity, while reducing dyspnoea and fatigue. Likewise, postoperative PR significantly improves respiratory function and exercise capacity in treated patients, but the effect on long-term functioning and HRQoL is still under debate.10,12 Nonetheless, exercise training during cancer treatment has demonstrated to be safe, feasible and associated with significant improvement in exercise capacity, symptoms and some domains of HRQoL.7,9,13,14
Furthermore, it has been confirmed that peak oxygen consumption is a strong independent predictor of overall long-term survival for individuals with NSCLC, while low exercise tolerance is associated with poor thoracic surgical outcomes.10,15
Lung cancer is one of the most prevalent types of cancer and research that investigates effects of exercise intervention or aims at developing PR programmes specific to these patients is increasing. However, optimal design of exercise intervention, tailored to lung cancer patients, either pre- or post-surgery, has yet to be established.9,13
In recent years, Crandall et al. 9 have published a systematic review of literature regarding effectiveness of exercise in patients surgically treated for NSCLC, either pre- or post-surgery. Crandall et al. 9 concluded that there is insufficient evidence to design the most suitable exercise intervention for patients surgically treated for NSCLC, suggesting that higher quality randomised controlled trials (RCTs) are required. 9
Furthermore, Cavalheri et al., 16 in 2014, published a Cochrane review about the effects of postoperative exercise training in NSCLC patients. The authors concluded that exercise training may potentially increase physical capacity of individuals following surgery, but their results should be interpreted with caution due to disparities of studies, methodologic limitations, significant risk of bias and small sample sizes of clinical trials analysed in that review. 16
Our final aim is to define and implement the most updated and evidence-based physical exercise interventions directed at patients surgically treated for NSCLC, both pre- and post-surgery. These programmes will become part of an experimental intervention in a future clinical trial designed to investigate the effects of physical therapy on surgical candidates with lung cancer.
The Cochrane Collaboration recommends periodic updating of literature search (e.g. every 2 years) to determine whether any new relevant information is available. 17 Thus, considering the good methodological quality of the previous systematic review of Crandall et al. 9 and similarities with the objectives this study, we have chosen to update their review and to take into consideration the previous results of Cavalheri et al. 16
Accordingly, we have carried out this systematic review, examining the best evidence regarding PR, focusing mainly on the physical training component for preoperative and postoperative interventions in patients with lung cancer undergoing surgery.
Materials and methods
We searched the following databases from May 2013 to May 2016:
MEDLINE;
EMBASE;
CINAHL;
Cochrane Library;
PsycINFO.
The search strategy is reported in Appendix 1 and is identical to the strategy used by Crandall et al. 9 up to May 2013.
Inclusion criteria
Studies were included in the review according to the following criteria:
Population. Trials that included participants who underwent surgery for NSCLC with curative intent. We excluded trials which included patients who underwent exclusively chemotherapy and/or radiotherapy because of the impact of these therapies would have on outcome measures and different prognosis of this population.
Intervention. Any supervised or unsupervised, inpatient or outpatient or home-based PR exercise-training programme. The exercise programme had to be described in sufficient detail in order to be reproducible.
Outcome measures. Exercise capacity, lung function, HRQoL and postoperative pulmonary complications (PPCs).
Methodology. Since this study investigates treatment efficacy, only RCTs were searched.
Language. Reports published in English, French, Italian, Portuguese and Spanish.
Study selection
Two reviewers (P.F.S.R., C.M.) reviewed all the records retrieved in order to check for inclusion criteria. They preliminarily screened titles and abstracts and then retrieved and analysed the full text of studies judged appropriate for study purposes. In case of disagreement, the opinion of a third reviewer was asked (S.C.).
Assessment of methodological quality
Two reviewers (P.F.S.R., C.M.) assessed methodological quality of each study according to the Cochrane Collaboration risk of bias tool. 18 In case of disagreement, the opinion of a third reviewer was asked (S.C.).
Data extraction
For every RCT included, two reviewers (P.F.S.R., C.M.) extracted the following data:
Participants: gender, age, type of surgery;
Intervention: type of exercise, intensity, length of intervention, duration of session, frequency, supervision (provided/not provided), individual versus group session, inpatient versus outpatient and/or home-based regimen;
Outcome measures collected;
Results.
When essential data were missing, the investigators requested them from authors.
Results
Bibliographic search results
We retrieved 556 references without duplicates. After preliminary review of titles and abstracts, we excluded 461 studies because their main subject was not related to our research question, 68 because they did not meet inclusion criteria, 5 because they were already present in the review by Crandall et al. 9 and 1 study because only protocol was published. 19 Of the remaining 21 studies, 2 were editorials20,21 and 5 were published as abstracts22–26 and therefore data were not complete. Regarding these abstracts, two22,26 were excluded because they were already included as full texts27,28 in our initial bibliographic research. Concerning the three remaining abstracts, we contacted the corresponding authors in order to obtain complete data. In one case, 25 the authors provided the requested data, whereas in the other two cases, our attempts were unsuccessful.22,23 Consequently, we analysed 15 studies. Upon reading the full text, nine studies were excluded from our review because they did not meet inclusion criteria: six studies were not RCTs,29–34 two studies did not entirely focus on patients who underwent surgery for NSCLC, as it also included patients receiving exclusively chemotherapy and/or radiotherapy,35,36 and one study 28 because it was only a feasibility study and was not focused on the effectiveness of exercise training. Therefore, six RCTs were included in this review.8,25,27,37–39 The flow chart representing selection process of studies is reported in Figure 1.
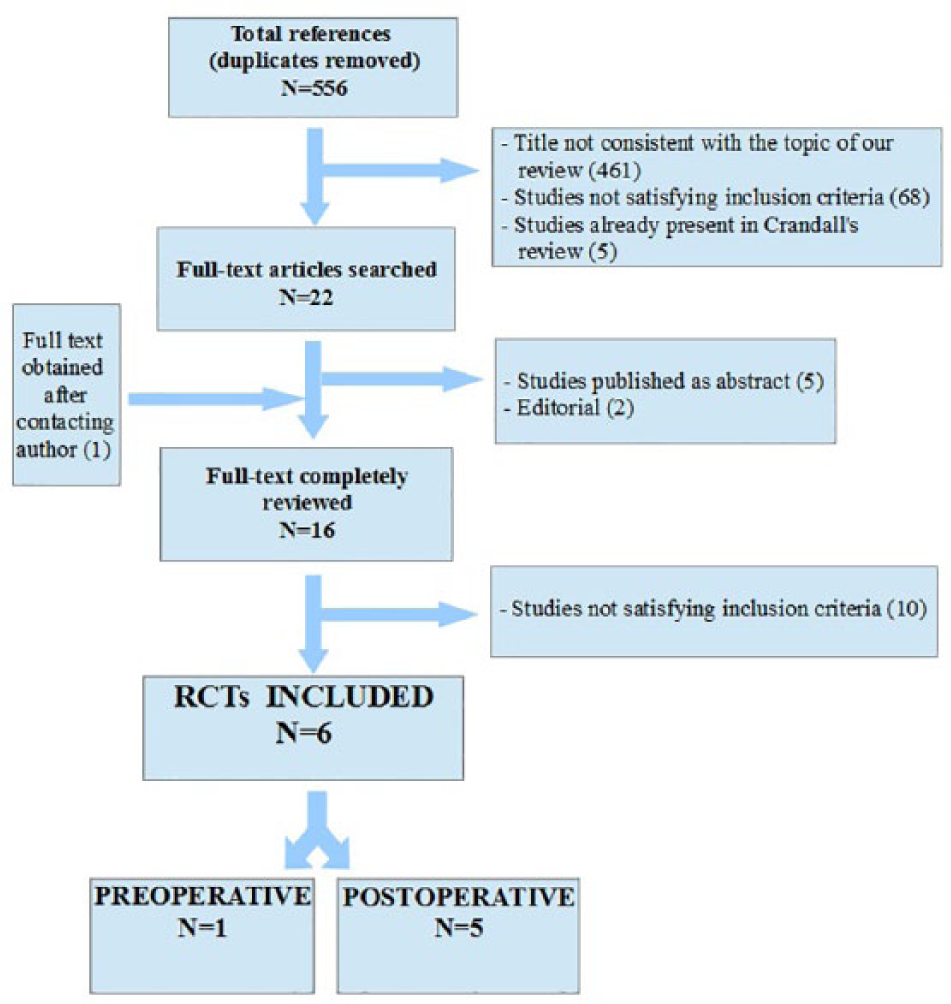
Flow chart of study selection.
Characteristics of included studies
The included studies were parallel RCTs and participants were randomised into an experimental intervention group (IG) or control group (CG).
One of the included studies focused on preoperative PR, 37 while the other five focused on postoperative PR.8,25,27,38,39 Detailed study characteristics are presented in Table 1.
Study characteristics.

PRE: preoperative; POST: postoperative; SD: standard deviation; IG: intervention group; CG: control group; VATS: video-assisted thoracoscopic surgery.
Participants
The sample size of preoperative trial consisted of 40 participants with an average age of 65 ± 7 years. 37 Overall, the five postoperative trials included 374 participants (range, 17–131); 191 were randomised into the experimental IG and 183 into the control one. In all, 278 of the 374 randomised patients completed follow-up (74.3%). Follow-up took place at different time points: at 4 weeks after surgery, 39 at 6 weeks after surgery, 27 at 8 weeks after baseline assessment, 25 at 20 weeks after intervention 38 and 1 year after the baseline assessment. 8 In all, 139 of these follow-up patients were allocated to the IG and 139 to the control one. Studies recruited both males and females, and average age of participants was 66 ± 10 years.
Methodologic quality
Methodologic quality of the included studies is reported in Figures 2 and 3.
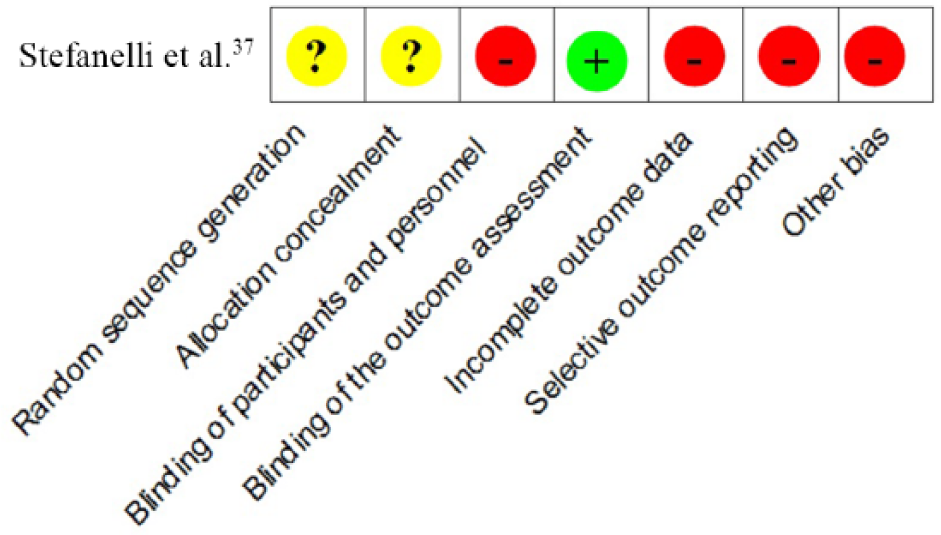
Risk of bias analysis of preoperative study.
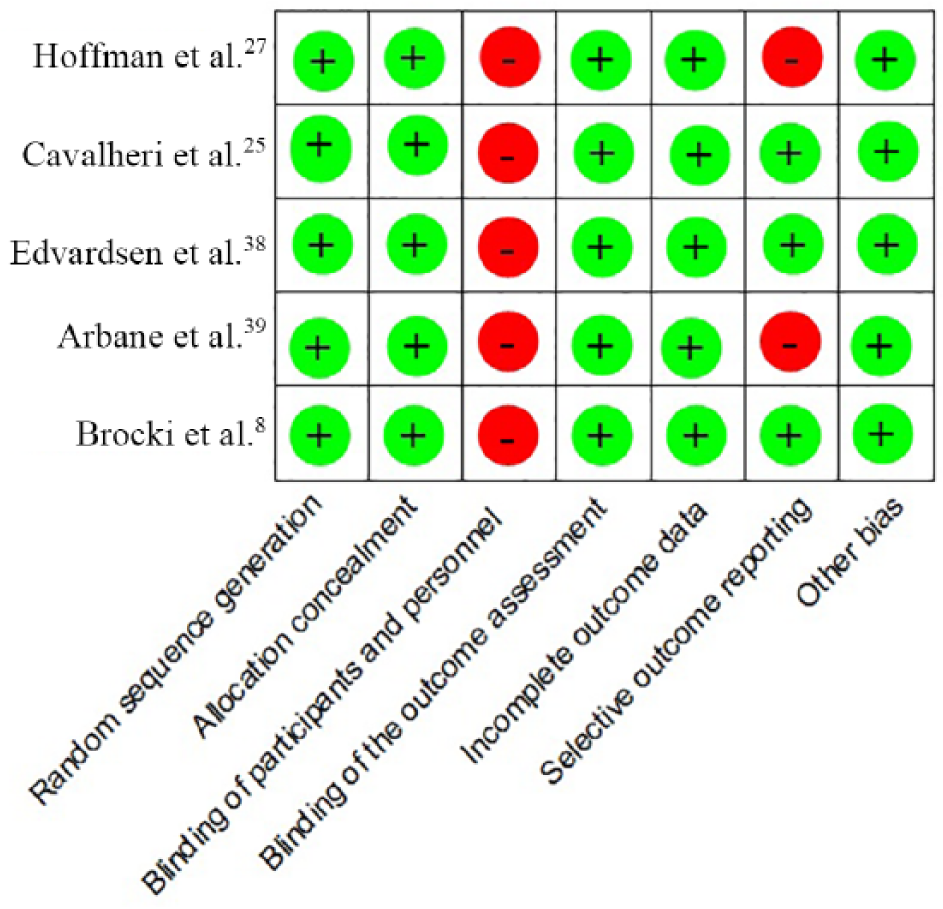
Risk of bias analysis of postoperative studies.
None of the studies reported blinding of participants and personnel. Four8,25,27,38,39 out of five 27 postoperative studies reported blinding of outcome assessors, and the preoperative study 37 did not report sufficient information to evaluate this aspect. However, the studies of Stefanelli et al. 37 and Hoffman et al. 27 were deemed as a low risk for detection bias, since outcomes analysed in these studies are usually measured in an objective manner. Risk of bias for included studies is reported in Appendix 2.
Characteristics of PR programmes
Table 2 summarises the characteristics of PR programmes described by the included studies.
PR programme characteristics.
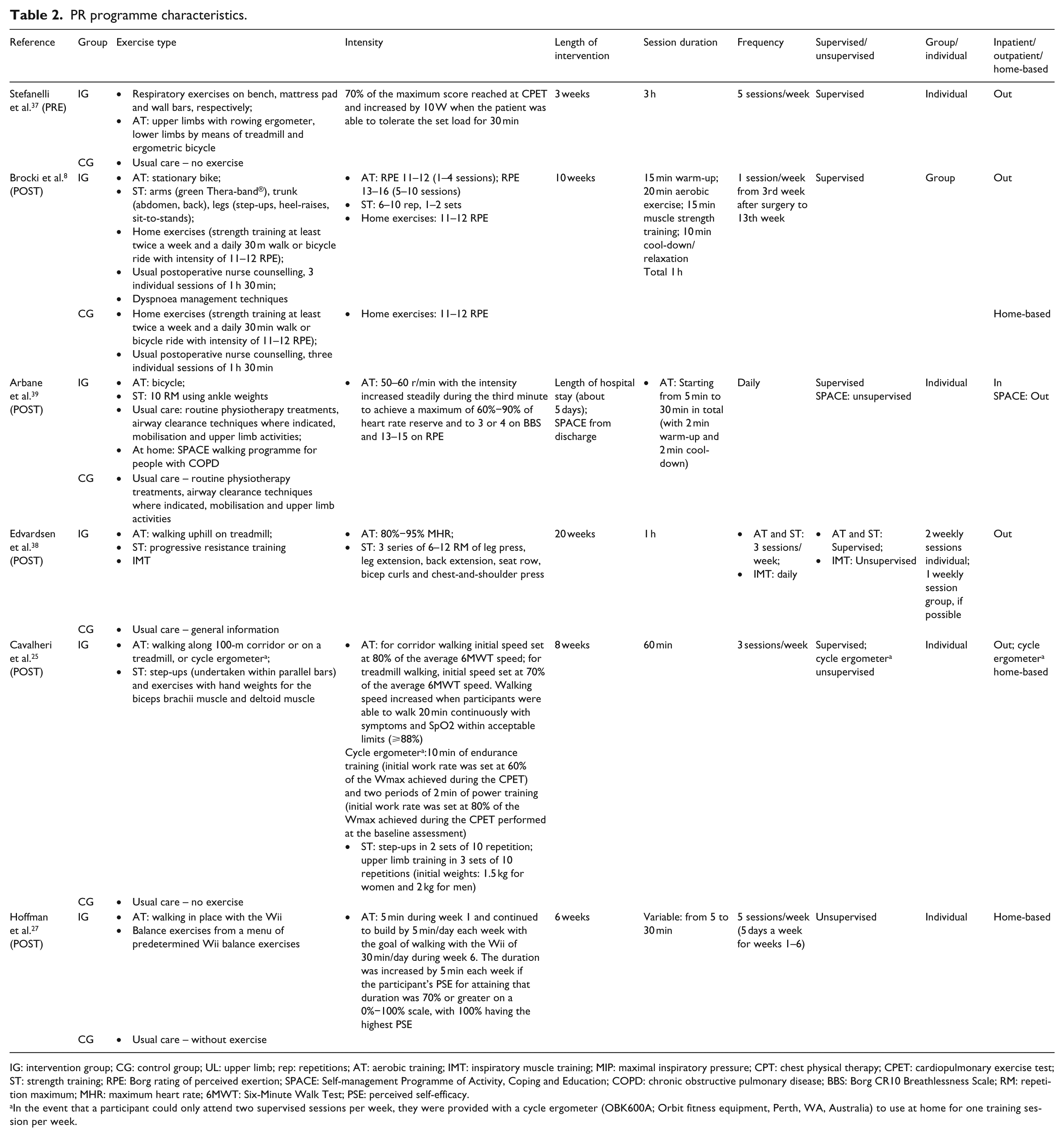
IG: intervention group; CG: control group; UL: upper limb; rep: repetitions; AT: aerobic training; IMT: inspiratory muscle training; MIP: maximal inspiratory pressure; CPT: chest physical therapy; CPET: cardiopulmonary exercise test; ST: strength training; RPE: Borg rating of perceived exertion; SPACE: Self-management Programme of Activity, Coping and Education; COPD: chronic obstructive pulmonary disease; BBS: Borg CR10 Breathlessness Scale; RM: repetition maximum; MHR: maximum heart rate; 6MWT: Six-Minute Walk Test; PSE: perceived self-efficacy.
In the event that a participant could only attend two supervised sessions per week, they were provided with a cycle ergometer (OBK600A; Orbit fitness equipment, Perth, WA, Australia) to use at home for one training session per week.
Preoperative rehabilitation programme
Regarding the preoperative PR, Stefanelli et al. 37 included incremental high-intensity aerobic training, both for lower and upper limbs and respiratory exercises. The PR programme lasted 3 weeks, consisting of five supervised individual sessions per week, conducted in an outpatient setting. The CG received usual care but further details were not reported.
Postoperative rehabilitation programmes
Postoperative programmes included aerobic and strength or balance training. Regarding the respiratory component, Edvardsen et al. 38 included inspiratory muscle training (IMT), Arbane et al. 39 incorporated routine physiotherapy treatments and Brocki et al. 8 incorporated dyspnoea management techniques.
The intervention described by Hoffman et al. 27 was a 6-week, home-based, unsupervised, walking and balance exercise programme using Nintendo Wii Fit Plus. The walking programme started off at 5 min/day for the first 5 days in week 1. Duration was increased every week in order to reach the goal of continuous walking for 30 min/day by week 6. Participants also performed a series of programmed balance exercises 5 days a week from week 1 to week 6. The CG performed usual care and was not given any advice concerning exercise.
The intervention programme of Cavalheri et al. 25 consisted in an 8-week individual, supervised, inpatient training 3 days/week comprising aerobic and resistance training. If some participants could only attend two supervised sessions per week, they were provided with a cycle ergometer (OBK600A; Orbit fitness equipment, Perth, WA, Australia) to use at home for one training session per week. The CG was instructed to continue performing their usual activities; in addition, they received weekly phone calls from a research assistant who asked them general questions about their health and well-being.
The intervention described by Edvardsen et al. 38 was a 20-week, high-intensity programme consisting of three outpatient sessions per week, one being a group session, when possible. Aerobic and strength training were supervised, whereas IMT was unsupervised and performed daily. CG performed usual care and was not given any advice regarding exercise, besides routine general information.
The intervention programme of Arbane et al. 39 consisted first in daily inpatient sessions, lasting about 5 days, up to discharge; after that, patients initiated Self-Management Programme of Activity, Coping and Education (SPACE) in an unsupervised and outpatient setting. The CG received usual care including routine physiotherapy treatments, airway clearance techniques, mobilisation and upper limb activities.
The intervention programme of Brocki et al. 8 consisted of weekly group rehabilitation sessions lasting 10 weeks, starting from the third post-surgery week. Sessions were supervised in an outpatient setting. This programme also included three individual sessions of postoperative nurse counselling, lasting one and a half hours, as part of usual care provided for both groups. Furthermore, the CG was given a home-based exercise programme including aerobic and strength training.
Outcome measures
Table 3 summarises outcome measures analysed in included studies.
Outcome measures.

PRE: preoperative; POST: postoperative; HRQoL: health-related quality of life; CPET: cardiopulmonary exercise test; 6MWT: Six-Minute Walk Test; SF-36: Short Form 36; FACT-L: Functional Assessment of Cancer Therapy – Lung scale; EORTC QOL: European Organisation for Research and Treatment of Cancer Quality Of Life; ISWT: Incremental Shuttle Walk Test.
Preoperative study
Exercise capacity was analysed by Stefanelli et al. 37 by means of VO2peak (maximum consumption of O2 at exercise peak) using the cardiopulmonary exercise test (CPET).
Regarding lung function, Stefanelli et al. 37 analysed forced expiratory volume in first second (FEV1) and diffusing lung capacity of carbon monoxide (DLCO).
Postoperative studies
All trials measured exercise capacity. Edvardsen et al. 38 analysed VO2peak using a continuous graded exercise protocol on a treadmill. Brocki et al. 8 and Hoffman et al. 27 used Six-Minute Walk Test (6MWT). Cavalheri et al. 25 used 6MWT and VO2peak performing also CPET. Arbane et al. 39 measured exercise capacity with Incremental Shuttle Walk Test (ISWT). They also recorded activity levels with an Actiwatch that was given to patients to wear at least 48 h preoperatively and then for 5 days post-surgery (or until discharge, if earlier). Participants were given the Actiwatch again 1 week prior to the 4-week postoperative assessment and were asked to wear it for at least 5 days.
Lung function was analysed in three trials. Cavalheri et al. 25 analysed FEV1, functional vital capacity (FVC), total lung capacity and DLCO. Edvardsen et al. 38 reported FEV1 and DLCO and Brocki et al. 8 analysed FEV1 and FVC.
HRQoL was assessed through Short Form-36 questionnaire (SF-36) in all trials8,25,27,38,39 and three of them also used the European Organisation for Research and Treatment of Cancer questionnaire (EORTC).25,38,39 Cavalheri et al. 25 analysed HRQoL using also the Functional Assessment of Cancer Therapy – Lung scale (FACT-L).
PR programme effectiveness
Preoperative study
Stefanelli et al. 37 trial reported that differences between groups were null at baseline. Instead, at T1 (after preoperative rehabilitation and pre-surgery) and at T2 (60 days post-surgery), it showed a significant difference in VO2peak between groups in favour of the IG (p < 0.001 and p < 0.01, respectively). Furthermore, in the IG, they observed a within-group significant improvement in VO2peak from baseline to T1. This improvement was not maintained after surgery, when patients in the IG fell back to their baseline values. On the contrary, within the CG, VO2peak registered a continuous decrease at both time points. Significant worsening after surgery brought this group to a level lower than baseline. Regarding lung function, this trial failed to report any between-group differences. Yet, it reported a significant within-group decrease of DLCO and FEV1, from baseline to T1 and from T1 to T2 for both IG and CG.
Postoperative studies
Regarding exercise capacity, Hoffman et al. 27 reported a significant delta difference in distances at 6 weeks post-surgery versus pre-surgery (p < 0.001). Cavalheri et al. 25 reported greater gains favouring IG for VO2peak (mean difference (95% confidence interval (CI)) 0.19 (0.04–0.33) L/min), O2 pulse (2 (0–3) mL/beat) and anaerobic threshold (11 (1–21)% of VO2peak); regarding 6MWT, the authors reported greater favouring IG for distance walked (mean difference (95% CI of difference) 52 (12–93) min). Edvardsen et al. 38 reported a significant difference between groups in VO2peak after postoperative PR (p = 0.02), favouring IG. Arbane et al. 39 did not clearly report exercise capacity levels measured by ISWT. We tried to contact the corresponding author to obtain complete data but our attempts were unsuccessful. Nevertheless, from data presented graphically in this study, it seems that, after postoperative PR, CG did not improve exercise capacity, whereas in IG, it improved by 60 min. However, we do not know if this difference was statistically significant. Also, using intention-to-treat analysis, they found no between or within-group significant differences for total active time, measured by Actiwatch, 4 weeks post-surgery. Brocki et al. 8 showed an improvement in walking distance 4 months and 1-year post-surgery in both groups, with no between-group differences at any time.
Lung function, analysed in Cavalheri et al., 25 Edvardsen et al. 38 and Brocki et al. 8 trials, did not present significant changes in FEV1 and FVC; only DLCO, reported by Edvardsen et al., 38 presented significant differences between groups after PR (p = 0.01), supporting IG.
In relation to HRQoL, the study by Hoffman et al. 27 showed a within-group improvement in IG after intervention for mental and physical domains of SF-36, but we cannot determine if this difference was statistically significant between groups because data were not completely reported. The study by Cavalheri et al. 25 reported no between-group differences in the three rating scales used. The study by Edvardsen et al. 38 reported significant differences between groups after intervention in both physical and mental domains of SF-36 (p = 0.006 and 0.02, respectively), supporting the experimental programme. Moreover, this trial analysed dyspnoea dominium of EORTC and found a significant improvement in IG (p = 0.03). The trial conducted by Brocki et al. 8 found no statistical differences between groups in any of the SF-36 domains, except for the one dealing with body pain, which revealed a statistically significant improvement favouring IG 4 months post-surgery (p = 0.01). Arbane et al. 39 stated no significant differences in quality of life between IG and CG, measured either by SF-36 or EORTC. However, when the subgroup with airflow obstruction was analysed, they found that the experimental exercise programme significantly prevented a decline in both mental and physical domains of SF-36 (0.01 and 0.04, respectively). Table 4 summarises HRQoL data collected by all the included studies using SF-36.
SF-36 data.
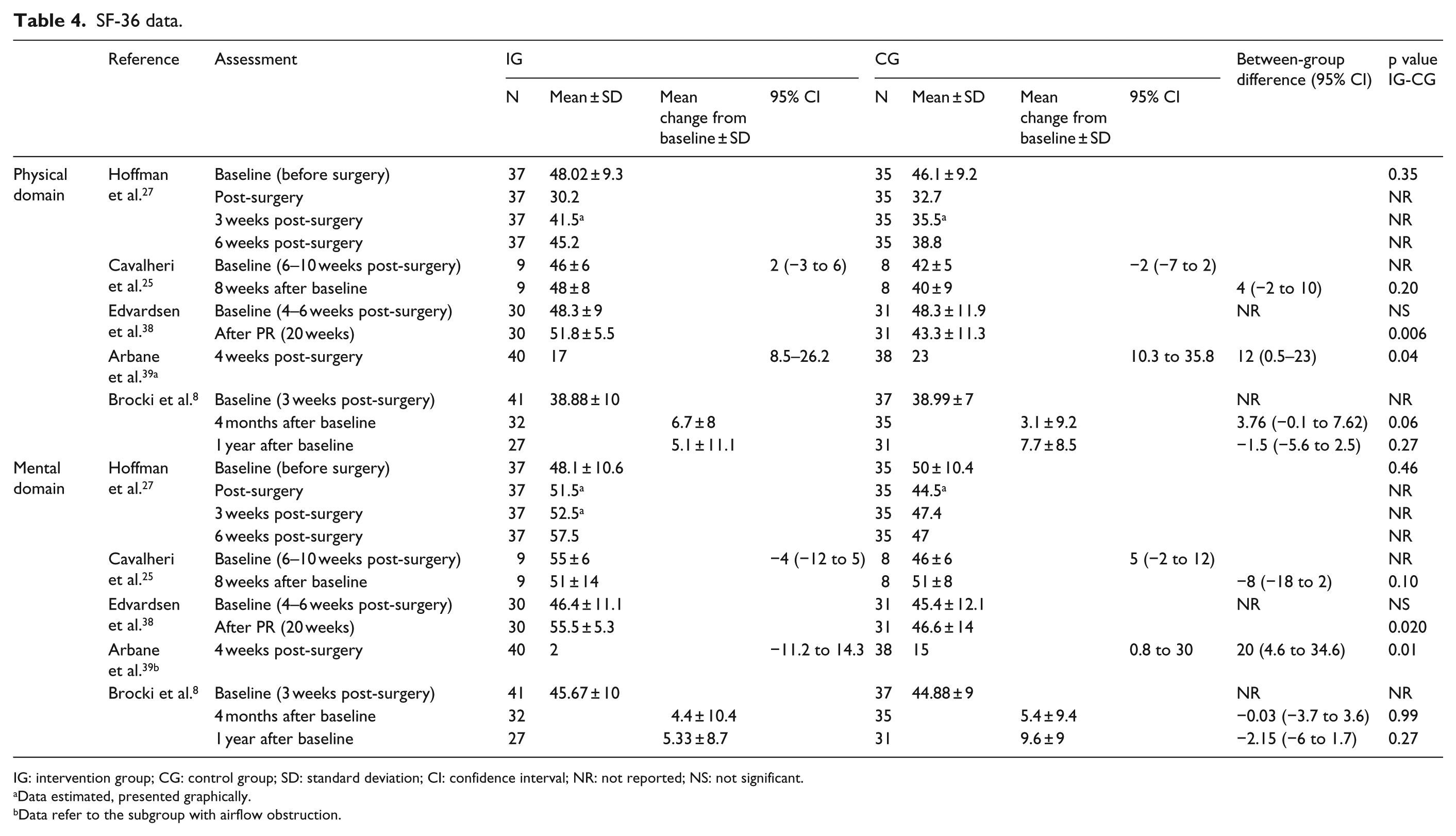
IG: intervention group; CG: control group; SD: standard deviation; CI: confidence interval; NR: not reported; NS: not significant.
Data estimated, presented graphically.
Data refer to the subgroup with airflow obstruction.
Appendix 3 summarises detailed results for every outcome collected by the included studies in order to assess effects of experimental interventions.
Discussion
This systematic review aimed at determining the best evidence-based physical exercise interventions directed at patients treated surgically for NSCLC, both pre- and post-surgery.
Regarding preoperative and postoperative PR, our review demonstrates that in this field literature is lacking a sufficient number of randomised clinical trials. Therefore, beyond the previous conclusions of Crandall et al., 9 highlighting the need for further high-quality RCTs and suggesting that an optimal rehabilitation programme should include aerobic, strength and breathing exercises, 9 we cannot add any relevant evidence. However, our results allow us to support previous findings of Cavalheri et al., 16 suggesting inclusion of exercise training in PR programmes after lung resection for NSCLC. 16
Preoperative PR
Concerning the effects of exercise training for people undergoing lung resection, we found only one RCT published in the last 2 years. 37 Moreover, findings of this study should be analysed with caution due to questionable methodologic quality, since randomisation method was not clearly described and attrition and reporting biases are likely to have affected results. Furthermore, the authors did not provide any information about blinding of assessors. However, outcomes measured in this study were instrumentally determined by precise guidelines, consequently blinding of assessors may not have been so essential. Regarding exercise-training programme, this trial followed current physical activity guidelines for PR in cancer patients (2–4 weeks, 5 times/week). 10 This training modality is feasible, although its efficacy has not yet been clearly confirmed by large sample size studies. 10 The trial of Stefanelli et al. 37 exhibited a beneficial effect of preoperative PR on physical performance in patients with COPD and NSCLC, even if no improvements in lung function were revealed. This result should be interpreted in light of the fact that exercise training was associated with significant increase in VO2peak, as confirmed by previous studies.40,41 Also, it is well documented that cardiorespiratory fitness is a strong independent predictor of postoperative complications and survival in NSCLC patients after lung resection.15,42,43 So, even if Stefanelli et al. 37 did not assess PPCs, we may infer that preoperative PR could reduce postoperative respiratory morbidity, length of hospital stay and health-care costs due to improvements in cardiorespiratory fitness induced by enhanced physical performance.44,45
Even though our research focused mainly on exercise training, we noticed that preoperative PR programmes often integrate a respiratory component, which frequently includes IMT.44,45 Indeed, a previous meta-analysis concluded that preoperative IMT significantly improves respiratory muscle function. 46 Hence, we suggest including this specific component in preoperative PR programmes.
Postoperative PR
Regarding postoperative PR, the five RCTs included in our review showed a good methodologic quality.8,25,27,38,39 These five studies were classified at low risk of bias for almost every parameter, except for the risk of performance bias. However, it is necessary to point out that, in the rehabilitation field, it is very difficult to guarantee participant and personnel blinding. For this reason, it is critically important to assure blinding of outcome assessors, as seen in four8,25,38,39 out of five 27 studies included in our review.
Concerning the effect of postoperative PR on physical capacity, the variability in PR programmes and outcome measures applied in the included studies prevented us from adding any relevant evidence to the previous systematic reviews.9,16 One of the included studies showed beneficial effects on cardiorespiratory fitness after supervised endurance and strength training, measured by VO2peak 38 and another one 27 showed an increase in the walking distance up to preoperative levels. Another study showed beneficial effects in both CPET and 6MWT. 25 These results are in accordance with the meta-analyses performed by Cavalheri et al., 16 supporting increase in physical capacity through exercise training in this population. Conversely, the other two trials8,39 revealed no differences between groups for physical capacity, with similar increases in walking distance and recovery up to preoperative functional levels in both groups. However, the results of Arbane et al. 39 should be considered with caution, since this study reported high number of lost to follow-up patients (27% in CG and 17% in IG); so, the risks of attrition bias and type II error cannot be entirely excluded. Regarding the trial of Brocki et al., 8 it is important to point out that some form of physical training was included in both IG and CG. Indeed, the authors intended to compare supervised versus unsupervised exercise training and outpatient versus home-based settings. Their results were not statistically significant but tended to show a slightly faster recovery through supervised exercise.
Concerning pulmonary function, our review does not demonstrate any changes after postoperative PR programmes, in accordance with Crandall et al. 9 and Cavalheri et al. 16 reviews and with previous research conducted on COPD patients. 47
Regarding HRQoL, our review suggests that exercise training could be advantageous. Even if results were not exactly identical in the included trials, four8,27,38,39 out of five 25 studies reported a certain degree of change in HRQoL using SF-36, always favouring IG. Certainly, there is still little evidence concerning the effects of exercise training on HRQoL, as also observed by Crandall et al. 9 and Cavalheri et al. 16 In addition, it has been shown that lung resection for NSCLC has a greater detrimental impact on quality of life compared to other major visceral surgeries. 4 Perhaps for this reason, research in this field has started to focus not only on functional outcome measures but also on quality of life as perceived by patients. Although NSCLC survivors are extremely vulnerable and, consequently, need time to recover from treatment, 4 there is now a growing body of evidence regarding this topic. Possibly, more prolonged treatments over time may have more decisive effects on this outcome.
The five postoperative trials included in our review presented various forms of PR programmes. They were similar only in one type of exercise included (aerobic), but each study also added different kinds of training (strength or balance) and they also differed in setting, session duration, intensity, length of intervention and frequency. These dissimilarities made it difficult to identify the best exercise intervention design. Even if it was not possible to establish the best evidence-based physical exercise intervention, previous studies support the inclusion of aerobic exercise training combined with other forms of exercise,11,31 such as strength training, as suggested by recent guidelines 10 and systematic reviews9,48 on optimal perioperative PR programmes for lung cancer patients. Considering that the majority of patients affected by lung cancer also present COPD, 3 exercise-training programmes specific for this population are often based on COPD training programmes and are frequently associated with a respiratory component. This component is usually made up of IMT,12,38 incentive spirometry, 49 airway clearance techniques 39 and respiratory exercises. 19
Regarding location of exercise intervention, there is no evidence that allows us to indicate the best setting or any other features of rehabilitation programmes. In any case, a recent review by Maguire et al. 50 analysed needs of people living with lung cancer and highlighted the importance of addressing fatigue, dyspnoea, pain, difficulties in daily activities, psychological distress and return to work issues. These domains should be included in any rehabilitation programme. Moreover, educational sessions would be useful in order to empower people to cope better with their disease. This review also pointed out difficulties in accessibility to health-care programmes due to transportation problems. Therefore, when defining and choosing an intervention programme, it is of utmost importance to consider patient needs and availability of local health-care services. Thus, the best PR programme would probably reflect a combination of supervised outpatient and unsupervised home-based training. Furthermore, bearing in mind the psychological condition of NSCLC patients, the inclusion of group sessions might be beneficial for sharing experiences and facilitating social domain. 51 Supporting this theme, a study conducted by Swenson et al. 52 reported that patients attending group sessions were more likely to complete the programme. Furthermore, the authors declare that group setting was acceptable and beneficial for this population. 52
Recent literature has demonstrated that either pre- or post-operative exercise training for NSCLC patients is safe, feasible and acceptable.7,9,13 In our review, none of the included studies reported data regarding safety of the applied intervention. In all, 96 of the 374 patients randomised dropped out. Surely, a drop-out rate of 26% might indicate limited acceptability or feasibility, although in this population a similar rate of withdrawal might be considered normal, as also reported by a recent study of Sommer et al. 28 Nevertheless, the majority of patients lost to follow-up were found in only one study 39 and the reason for this drop-out rate concerned, in most cases, loss of inclusion criteria.
This review has some limitations. First, we only analysed the last 3 years of published literature; however, we choose not to search for older publications because two extensive and well-done systematic review had been published in recent years.9,16 Second, although we only focused on collecting evidence regarding exercise training programmes, we recognise that other rehabilitation interventions (i.e. chest physiotherapy, educational or psychological programmes, nutritional interventions) might be beneficial in this population. Finally, the clinical trials included in this review showed different quality levels and were not completely free of risk of bias, although we know that a certain risk of bias may almost always be present in studies conducted in the field of rehabilitation. Regardless of different quality levels of evidence, this review suggests that inclusion of exercise-training programmes should be considered for this population, both pre- and post-surgery. In particular, exercise training may have an important role for patients that already have compromised functional capacity or present comorbidities, such as COPD.9,11,16,53
In conclusion, this review has shown that, because of insufficient number of RCTs and substantial heterogeneity between types of interventions, it is not possible to establish the best exercise intervention programme, either pre- or post-surgery, for patients surgically treated for NSCLC. Nevertheless, this review further emphasises the complexity of PR for this population. Interventions often include several interacting components such as exercise training, IMT, incentive spirometry, airway clearance techniques and respiratory exercise. This systematic review highlights the urgent need for additional and larger RCTs with better methodology, in order to collect stronger evidence and clarify the role of exercise-training programmes for these patients. Finally, we should highlight the value of both pre- and post-surgery physical training programmes, implemented in a multidisciplinary environment, that include aerobic training as the most relevant component to improve exercise capacity.
Clinical messages
Urgent need for additional and larger RCTs with better methodological quality in order to identify the best physical exercise interventions design for surgically treated NSCLC patients.
Literature suggests inclusion of both aerobic and strength training in an optimal perioperative PR programme.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Acknowledgements
We thank Dr Vincent Corsentino and Dr Lorena Palladini for their skilled linguistic revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Italian Ministry of Health. We would like to thank very much for funding the project ‘Effects of early pulmonary rehabilitation and long-term exercise on lung function, quality of life and postoperative outcome in lung cancer patients’ (Project Code: GR-2011-02351711) within Bando Ricerca Finalizzata e Giovani Ricercatori 2011/2012.